Lesion location in the hierarchy and its clinical effect on locomotion
(See Tables 13.4 and 13.5 for all clinical signs associated with lesions in different parts of the nervous system.)
Forebrain lesions in quadrupeds have little effect on basic locomotion as this is primarily directed by senior management in the brainstem.
Cortical lesions may result in mild motor signs such as a stumbling gait and contralateral postural reaction deficits (‘knuckling’) occur if ascending proprioceptive systems are compromised. Walking in wide circles may also be noted due to effects on basal nuclei. Note that circling occurs with forebrain and vestibular disease. With forebrain lesions, circles tend to be large diameter while tighter circles occur with vestibular disease. Additionally, forebrain lesions will not have other signs of vestibular dysfunction, such as head tilt or nystagmus.For example, a calf was presented walking in large-diameter circles to the right, displaying, left-sided visual deficits and reduced awareness (see Chapter 11). The function of cranial nerves III-XII, and spinal cord reflexes were normal. These findings indicate that the brainstem and spinal cord were not affected (see Fig. 13.1). The signs of dysfunction point to a lesion in the forebrain, specifically the right cerebral hemisphere, accounting for the reduced awareness, circling, and the left-sided visual deficits (the optic pathways decussate en route to the visual cortex.) An abscess in the right occipital cortex was confirmed on MRI scan (Fig. 9.5).
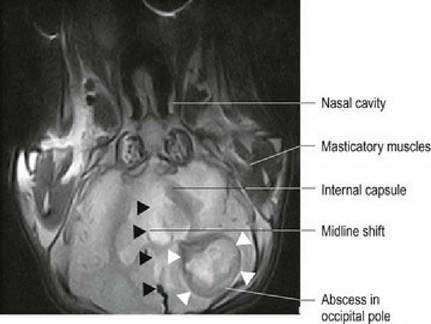
Fig. 9.5 Magnetic resonance image in the dorsal plane of calf brain depicting an abscess in the right forebrain. White arrowheads outline the abscess, and black arrowheads indicate the distortion of the brain,
with a shift of the midline towards the left, due to the mass effect of the abscess
(courtesy of Dr.
Michael Hewetson, University of Finland).Lesions involving basal nuclei often have minimal effect on voluntary movement and do not usually lead to adventitious (unexpected) movements such as seen in humans. Occasionally, lesions may cause the animal to have torticollis and be curved to one side or circle to one side, or have bizarre, complex movements with dystonia and chorea (involuntary, jerky, uncoordinated movements). Experimentally, lesions in the caudate nucleus and putamen can result in hyperactivity, whereas lesions in the globus pallidus can cause hypoactivity. For example, bilateral lesions of the putamen may result in obstinate progression with the animal trying to continue to walk even when it has come up against a wall (‘head-pressing’). Bilateral lesions of the globus pallidus can result in the animal remaining in a fixed posture for prolonged periods even if the posture is abnormal.
Lesions in the midbrain can cause decerebrate rigidity by disconnecting the forebrain from the caudal brainstem. The UMN nuclei facilitating extensor activity (e.g. pontine reticular formation and vestibular nuclei) are released from cerebral inhibition, while the UMN nuclei facilitating flexor activity are no longer facilitated by cerebral input. The animal will have opisthotonus with hyperextended limbs, trunk and neck
(Fig. 9.6).
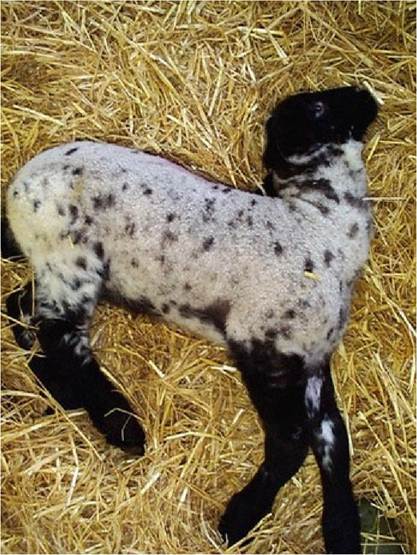
Fig. 9.6 Lamb with opisthotonus
(courtesy of Dr Phil Scott, University of Edinburgh).
Lesions in the cerebellum will affect motor coordination, specifically the rate, range and force of movement. However, executive and senior management of the motor systems are still functioning. The UMN centres can still talk to junior management (spinal interneuronal circuitry) and the workers (LMNs) so movement is strong and purposeful, but it lacks coordination and is ataxic. Failure of coordination of agonistantagonist muscle function may result in tremor.
Spasticity may occur due to loss of the cerebellum’s inhibitory influence on UMN nuclei of the brainstem. This results in excessive output from UMN nuclei and extensor dominance. Lesions in the vestibulocerebellum or caudal cerebellar peduncle can result in vestibular signs (see Chapter 8).Paresis is reduced voluntary movement, whilst paralysis is loss of voluntary movement. ParesisZparalysis occurs due to loss of motor systems associated with initiation and facilitation of movement (UMNs) or due to the loss of LMNs and neuromuscular unit that carries out the movement.
Lesions in the brainstem affecting UMN nuclei will result in paresis in the limbs and trunk and perturbed locomotion. Bilateral lesions of caudal brain stem can cause tetraparesis/plegia.
ParesisZparalysis due to spinal cord lesions is usually described based on the character of the clinical signs; these signs differentiate into upper or lower motor neuron lesions. Damage to UMNs causes UMN signs, and loss of LMNs causes LMN signs (Fig. 9.7). The two types of lesions are differentiated by the Neuro RAT (Reflexes, Atrophy, Tone) (see Fig. 5.6 and Table 5.2). With UMN lesions (involving ‘central motor neurons’), although the myotatic reflex and other limb reflexes will be intact and extensor muscle activity may dominate, this is not sufficient to support the animal, thus the animal will be paretic or recumbent. Input from supraspinal motor systems is required to achieve sufficient and coordinated activity to maintain balance and posture and to initiate and terminate movement. With LMN lesions (affecting ‘peripheral motor neurons’), loss of innervation to the muscles results in reduced muscle tone, loss of reflexes and rapid (neurogenic) atrophy. The animal will be obviously weak in the affected areas (Fig. 9.7).

Fig. 9.7 Dog with UMN lesion to pelvic limbs. This dog had severe spinal cord damage, such that an extensive area of the TL cord had been destroyed by a process called ascending/descending myelomalacia.
The destruction of LMNs in the TL region has caused LMN signs to the abdominal wall muscles. This is evidenced by loss of tone in the abdominal wall and the resulting pot belly.Tetraparesis/plegia can occur with lesions sited anywhere from caudal brainstem to T2, whereas paraparesis/plegia can occur with lesions sited between T2 and the sacral segments. Unilateral lesions of the spinal cord can result in ipsilateral paresis or paralysis (hemiparesis/plegia).
Table 13.5 lists the specific signs for lesions in the different regions of the spinal cord.
The Schiff-Sherrington syndrome may be seen in animals with severe, acute spinal cord lesions in the thoracolumbar spinal cord. This syndrome is characterised by spasticity of the thoracic limbs when recumbent, although these limbs may function normally when the animal is assisted to stand. The extension is due to loss of inhibitory influences from neurons in the cranial lumbar area that inhibit LMNs supplying thoracic limb extensors. Within the first few hours of sustaining the lesion, the animal may also have reduced tone and reflexes in the pelvic limbs, despite the lesion being cranial to the lumbar intumescence. This is a form of spinal shock, which occurs to a much greater extent in primates and humans than in domestic animals. Schiff- Sherrington syndrome indicates severe damage, but not necessarily permanent loss of function of the spinal cord and usually resolves within 1-2 weeks.