Particle Deposition onto the Mucociliary System Depends on Particle Size and Occurs by Impaction, Sedimentation, and Diffusion
Harmful material is inhaled as aerosols suspended in air or as toxic gases. The term aerosol refers to collections of particles or liquid droplets that are small enough to remain suspended in air for a period of time.
For epidemiological purposes, particles are generally described as inhalable or respirable. Inliala- ble particulates have a mass median diameter of K) microns (micrometers, μm) or less (referred to as PiMlO). Respirable particulates have a diameter of 2.5 μm or less (PM2.5). Ample evidence now indicates that increases in the atmospheric concentrations of PMlO or PM2.5 are associated with worsening of respiratory disease and increased hospital admissions for cardiopulmonary disease in people. Intensively housed animals often are exposed to PM 10 and PM2.5 concentrations greater than those known to cause respiratory disease in humans.Particles and aerosols are removed from the air when they contact the moist epithelial surface of the tracheobronchial tree (Figure 50-1). The distance that particles and aerosols travel into the tracheobronchial tree depends on particle size. larger particles, greater than 5 μm in diameter, contact the airway wall by inertial impaction. Inertial impaction occurs at the bends in the large airways because large particles traveling at high velocity have so much momentum that they fail to negotiate the turns. Sites of inertial impaction are provided with lymphoid tissue, such as tonsils and bronchus-associated lymphoid tissue. As airflow rates diminish deeper in the lung, particles 1 to 5 μm in diameter settle onto the walls of the airways by sedimentation. The smallest particles reach the peripheral airways and alveoli, where they either contact the epithelial surface by diffusion or are exhaled again. Inhaled drugs must be delivered in a form with a particle size of 1 to 5μm to be deposited onto the airway wall and remain in the lungs.
The deposition of particles within the respiratory tract is influenced by the pattern of breathing. Slow, deep breathing transports particles deep into the lung, whereas rapid, shallow breathing enhances inertial deposition in the larger airways. Bronchoconstriction enhances deposition of particles in more central airways, whereas bronchodilation favors more peripheral distribution.
The deposition of toxic gases depends on their solubility and concentration. Highly soluble gases, such as sulfur dioxide (SO2), in low concentrations are removed by the nose, but in higher concentrations they can penetrate deeper into the lung. Less soluble gases can gain access to the alveoli. Toxic gases stimulate a variety of protective mechanisms, such as bronchospasm, mucus hypersecretion, coughing, and sneezing.
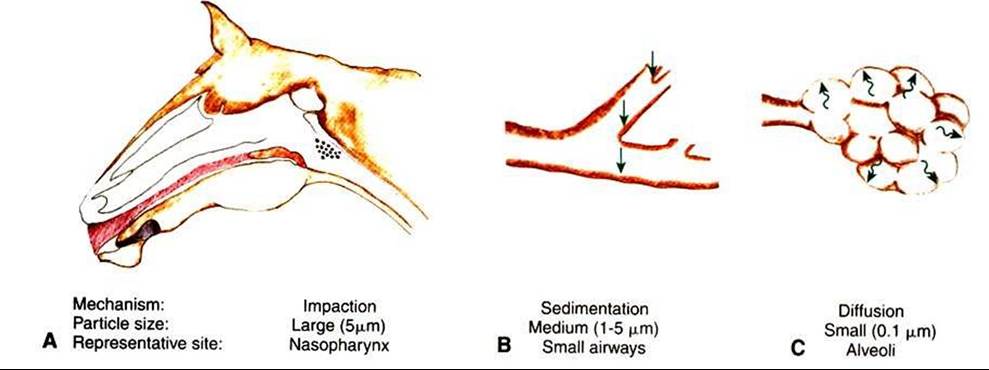
FIGURE 50-1 Mechanisms of particle deposition in the tracheobronchial tree. A, Large particles are deposited by impaction in the bends in the larger airways. B, Medium-sized particles are deposited in the smaller airways by sedimentation. C, Small particles contact the walls of the alveoli by diffusion.
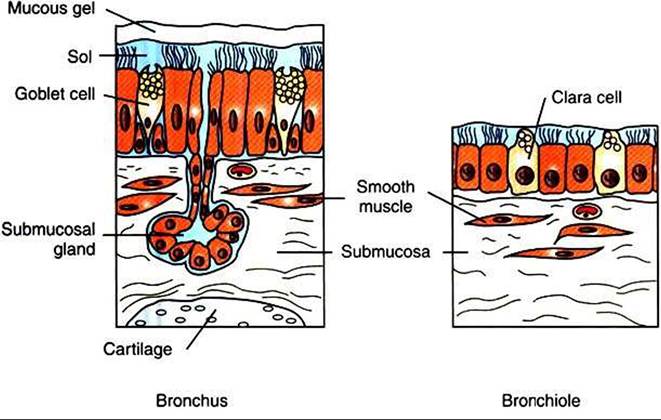
FIGURE 50-2 Diagram of the epithelium and submucosa of a bronchus and bronchiole. In the bronchus the epithelium is pseudostratified columnar and includes goblet cells, ciliated cells, and basal cells that do not reach the surface of the epithelium. A bronchial gland is shown in the submucosa with its duct passing through the smooth muscle. Cartilage underlies the mucosal IayenThe cilia beat within a sol layer over which is a layer of gel-type mucus. In the bronchiole the epithelium is Cuboidal and is a mixture of ciliated cells and secretory Clara cells. Smooth muscle is shown in the submucosa. Bronchioles normally do not have submucosal glands or goblet cells, and there is no cartilage in their walls.