PULMONARY VENTILATION
1. What makes up dead space ventilation?
2. Is physiologic dead space volume less than anatomic dead space volume?
3. What are the components of tidal volume?
4. What functions are served by dead space ventilation?
5.
How do intrapulmonic and intrapleural pressures change during a respiratory cycle?6. What provides for the recoil tendency of the lungs during expiration?
7. How could a condition of pneumothorax be corrected?
8. How does a decrease in mediastinal pressure (as occurs during inspiration) assist in the return of blood and lymph to the heart?
Ventilation is generally regarded as the process by which gas in closed places is renewed or exchanged. As it applies to the lungs, it is a process of exchanging the gas in the airways and alveoli with gas from the environment. The main function of breathing is to provide for ventilation. When cattle are stunned at the time of slaughter, it has been observed that breathing often stops. The heart continues to beat for 4 to 10 minutes longer, but it also stops when the oxygen available from the functional residual capacity has been depleted. Therefore, a nonbreathing animal still has resuscitation potential if the heart continues to beat.
Dead Space Ventilation
The tidal volume is used to ventilate not only the alveoli but also the airways leading to the alveoli. Because there is little or no diffusion of oxygen and carbon dioxide through the membranes of most of the airways, they compose part of what is called dead space ventilation. The other part of dead space ventilation is made up of alveoli with diminished capillary perfusion. Ventilating these alveoli is ineffective in producing changes in the blood gases. Ventilation of nonperfused alveoli and the airways, because neither accomplishes exchange of the respiratory gases, is referred to as physiologic dead space.
Physiologic dead space is defined as the volume of gas that is inspired but takes no part in gas exchange in the airways and alveoli. Therefore, the tidal volume (Vr) has a dead space component (Vd) and an alveolar component (Va), or Vt = Vd + Va.Dead space ventilation is a necessary part of the process of ventilating the alveoli and is not totally wasted. It assists in tempering and humidifying inhaled air and in cooling the body under certain conditions, such as when panting is necessary. During panting, the respiratory frequency increases and the tidal volume decreases so that alveolar ventilation remains approximately constant.
Pressures That Accomplish Ventilation
The pressure within the lungs is referred to as intrapulmonic pressure and pressure outside the lungs but within the thoracic cavity (between the visceral and parietal pleura) is referred to as intrapleural pressure. Contraction of the diaphragm and external intercostal muscles is followed by air flow into the lungs during inspiration because the pressure within the lungs, the intrapulmonic pressure, becomes lower than the atmospheric pressure. Similarly, air flows out of the lungs during expiration because the intrapulmonic pressure exceeds atmospheric pressure at that time.
The intrapulmonic pressure decreases during inspiration because the volume of the lungs increases. The lungs can increase in volume because they are elastic structures that can stretch. Also, the pressure around them, the intrapleural pressure, is being reduced because the volume of the intrapleural space increases in response to contraction of the diaphragm and external intercostal muscles (see Figure 10-11). When contraction of the inspiratory muscles ceases, expiration begins.
To permit air to flow out of the lungs during expiration, the intrapulmonic pressure must become positive. Positive pressure is primarily generated by the recoil tendency of the lungs, which were previously stretched during inspiration. The recoil tendency is produced not only by the elastic fibers within the lung but also by surface tension of fluid that lines the alveoli.
Retraction of the lungs can also be assisted by expiratory muscles. The diaphragm is an inspiratory muscle and its contraction assists only inspiration; conversely, its relaxation permits expiration. During eupnea the intrapulmonic pressure can be about -1 mm Hg (below atmospheric) during inspiration and it can be.+1 mm Hg during expiration. During this time, the intrapleural pressure changes from -2 mm Hg at the end of expiration to about -6 mm Hg at the end of inspiration. Thus, the intrapleural pressure changes slightly more than the intrapulmonic pressure changes. The intrapleural and intrapulmonic pressures associated with inspiration and expiration are shown in Figure 10-13.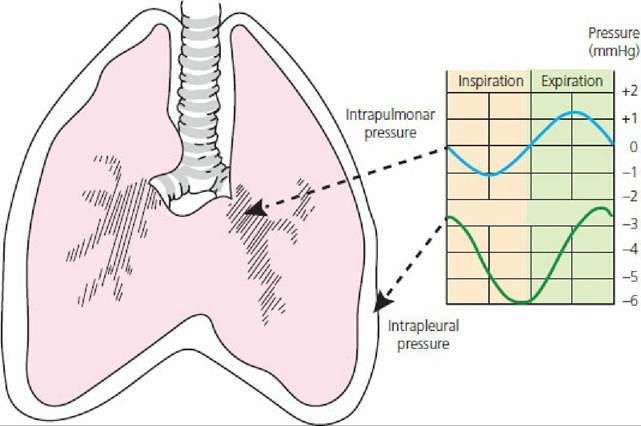
■ FIGURE 10-13 Intrapleural and intrapulmonic (intrapulmonary) pressures associated with inspiration and expiration. (Adapted from Ganong WF. Review of Medical Physiology. 20th edn. New York: McGraw-Hill, 2001.)
Intrapleural pressure (pressure in a closed space) is normally lower than atmospheric pressure, even at the end of expiration and before inspiration. This is a result of the constant recoil tendency of the lungs and of the absorption of gases from closed spaces caused by the existence of a diffusion gradient between the closed space and venous blood. The total pressure in the intrapleural space is in equilibrium with venous blood. It is lower than atmospheric pressure because the reduction of PO2 caused by oxygen absorption is greater than the increase in PCO2. The reduced total pressure of the intrapleural space is comparable with that of a slight vacuum.
Pneumothorax
If the intrapleural space is opened to the atmosphere (e.g., during certain surgical procedures), it would not be possible for diaphragmatic contraction to generate a greater vacuum in the intrapleural space and the lungs would not inflate.(Figure 10-14). This condition is known as pneumothorax.
A respirator would be necessary to ventilate the lungs or the animal could die. Correction of pneumothorax involves effecting final closure of the unnatural opening simultaneously with reestablishing negative pressure in the intrapleural space allowing for normal lung expansion. Once corrected, the next inspiration would increase the negative pressure in the intrapleural space and the lungs would expand because the trachea would be the only passageway available for air intake.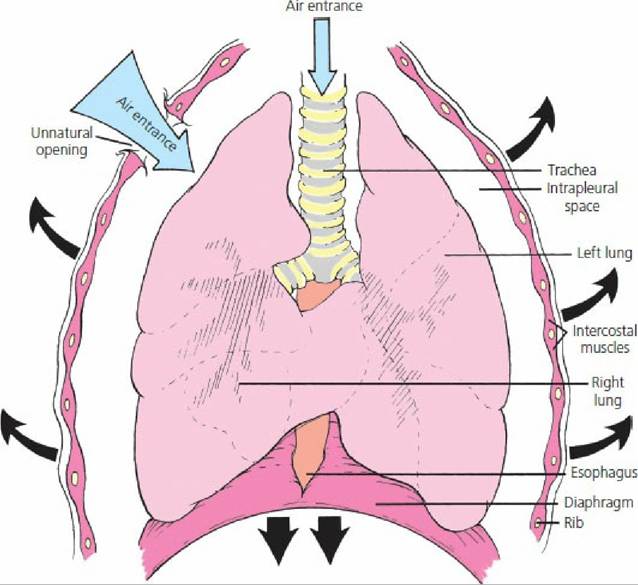
■ FIGURE 10-14 Pneumothorax (ventral view). The volume of air that enters at the unnatural opening exceeds that which enters the trachea when the intrapleural volume is increased during inspiration. The intrapleural pressure reduction is then not sufficient to permit lung inflation. The dark arrows show the directions of thoracic enlargement when the diaphragm and inspiratory intercostal muscles contract during inspiration.
Mediastinal Pressure
During inspiration, when intrapleural pressure is reduced, mediastinal space pressure is also reduced. Reduction of the mediastinal space pressure is followed by the expansion of volume and reduction of pressure within the distensible structures of the mediastinal space (venae cavae, thoracic lymph duct, esophagus). This reduction in pressure assists in the return of blood and lymph to the heart. During regurgitation in ruminants (see Chapter 12), reduced pressure in the esophagus, associated with an exaggerated inspiration with a closed glottis, also assists in this process.
■