Pulse Pressure IncreasesWhen the StrokeVoIume Increases, Heart Rate Decreases, Aortic Compliance Decreases, or Total Peripheral Resistance Increases
Because the arterial pulse is so frequently palpated in patients, it is important for the veterinary clinician to understand the factors that typically influence pulse pressure. First, an increase in stroke volume tends to increase pulse pressure.
Because cardiac ejections create the arterial pulsations in the first place, it is not surprising that larger ejections create larger pulsations. Figure 22-9, A, depicts this effect and shows that an increase in stroke volume also increases mean arterial pressure. Mean pressure increases because an increased stroke volume increases cardiac output.A second factor that tends to increase pulse pressure is a decrease in heart rate. Between cardiac ejections, blood
continues to run out of the aorta and through the systemic circulation, and aortic pressure decreases. It falls to a minimal (diastolic) level before being boosted again by the next cardiac ejection. When heart rate decreases, there is a longer time between ejections and therefore a longer time for blood to run out of the aorta and into the systemic circulation. The blood pressure in the aorta falls to a lower level before the next cardiac ejection, and pulse pressure is increased (Figure 22-9, B). A decrease in heart rate decreases the mean arterial pressure because a decreased heart rate results in a decreased cardiac output.
Figure 22-9, C, shows the effect of a simultaneous increase in stroke volume and decrease in heart rate. In this example, cardiac output, which is stroke volume multiplied by heart rate, remains unchanged. Therefore, mean arterial pressure remains unchanged. However, pulse pressure is greatly increased as a result of the combined effects of an increase in stroke volume and a decrease in heart rate. Aerobic conditioning in humans, and in some animals, leads to increased stroke volume and decreased heart rate at rest.
Therefore, in a well- trained athlete, mean arterial pressure is typically normal, but pulse pressure is greater than normal. Palpation of the arteries of an athlete at rest reveals a strong, slow pulse.A decrease in arterial compliance (stiffening of the arteries) is a third factor that tends to increase pulse pressure (see Figure 22-9, D). With each ventricular systole, the heart ejects blood into the aorta and large arteries, which distends these vessels. If these vessels become stiff, a greater increase in pressure is required to distend them. Arterial stiffening also decreases diastolic arterial pressure. This effect is more difficult to grasp intuitively but should not be surprising, lust as aortic pressure rises to higher-than-normal levels when the heart ejects blood into a stiff aorta, so does aortic pressure fall to lower-than-normal levels when blood runs out of the stiff aorta between cardiac ejections. The higher systolic pressure and lower diastolic pressure are simply two direct consequences of the same phenomenon: decreased arterial compliance. The major arteries tend to become stiffer as a result of the normal aging process, which accounts for the increase in pulse pressure that is typical in older humans and some animals.
In general, cardiac output is not affected by arterial stiffening. A healthy ventricle is able to generate the higher systolic pressures needed to eject blood into a stiff arterial system, although ventricular hypertrophy is sometimes triggered. Moreover, arterial stiffening generally has very little effect on TPR because the arterioles remain normal. The arteries, although stiff, retain their large diameters and therefore low resistance. Mean arterial pressure, the product of cardiac output and TPR, is therefore generally unchanged by arterial stiffening.
Arteriolar vasoconstriction is a fourth factor that typically increases pulse pressure (Figure 22-9, E). In actuality, vasoconstriction does not affect pulse pressure directly but acts through a stiffening of the arteries.
Vasoconstriction increases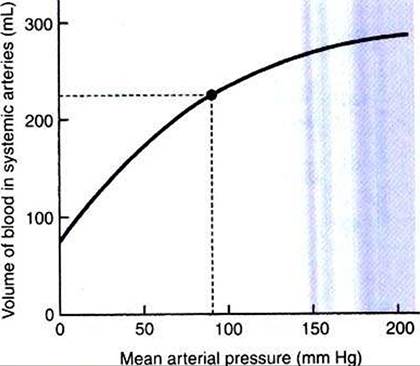
FIGURE 22-10 This volume-pressure graph shows that normal systemic arteries become stiffer (less compliant) when mean arterial pressure increases above its normal value (dot). (Recall that compliance is equal to the slope of a volume-pressure curve.)
TPR» and blood backs up or accumulates in the large arteries. Mean arterial pressure increases, and the arteries become more distended than normal. Distention forces the arteries toward their elastic limit; they become stiffer than arteries under normal pressurization (Figure 22-10). This stiffening of the arteries causes pulse pressure to increase. Because TPR is elevated, mean arterial pressure also increases.
Many human patients develop both stiffening of arteries (as a consequence of aging) and essential hypertension (caused by increased TPR). This combination produces dramatic increases in pulse pressure (Figure 22-9, F). An older person with severe hypertension might have a pulse pressure of 110 mm Hg (200 mm Hg systolic minus 90 mm Hg diastolic). Arterial hypertension and arterial stiffening both are less common in veterinary species.
In summary, pulse pressure lends to be increased by increased stroke volume, decreased heart rate, decreased arterial compliance, or vasoconstriction.
Some of the cardiac defects that produce murmurs also cause characteristic changes in a pulse pressure. For example, a patient with patent ductus arteriosus has a large left ventricular stroke volume, which elevates aortic systolic pressure. Aortic diastolic pressure is much lower than normal because, between cardiac ejections, blood runs out of the aorta by two pathways: into the systemic circuit and through the open ductus. Pulse pressure is dramatically increased. Aortic regurgitation causes a similar, characteristic increase in pulse pressure (Figure 22-9, G). During diastole, blood leaves the aorta through two pathways: forward into the systemic circuit and backward (through the incompetent valve) into the left ventricle. Stroke volume is elevated because, with each systole, the left ventricle ejects both the blood that has returned to it through the normal pathway and the regurgitant blood.