Regulation of Arterial Blood Pressure and Blood Volume
Arterial blood pressure is a function of cardiac output (CO) and total peripheral vascular resistance (TPR), usually written as MAP = CO ? TPR, where MAP is mean arterial pressure.
To understand the basis for this function, recall that arteries are relatively noncompliant and function as a reservoir of blood under pressure. The pressure depends on the amount of blood being pumped into the reservoir (Co) and the rate at which blood is permitted to flow out of the reservoir (Fig. 18-9). Recall also that the resistance of the arterioles, which contribute the most to the total vascular resistance, regulates the rate of blood flow out of the arteries. Thus, the level of cardiac function and the degree of arteriolar constriction are the two determinants of MAP. Changes in MAP can be brought about by changes in cardiac function, the degree of arteriolar constriction, or some combination of these determinants. Any chemical regulator (e.g., hormone or paracrine agent) or neural reflex that affects cardiac activity or the smooth muscle of arterioles has the poten-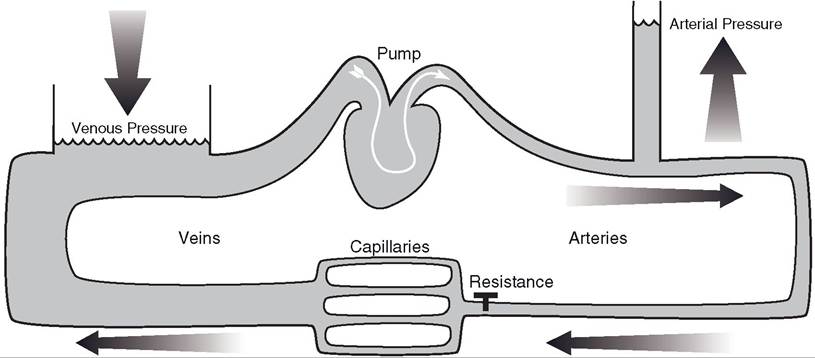
Figure 18-9. Model of circulatory system with pump vessels regulating outflow from arteries (arterioles), and the pump. Height of fluid columns in arteries and veins pump depends in part on the venous pressure.
supplying low-compliance vessels (arteries), off-on valve low-pressure compliant vessels (veins) returning fluid to indicates relative pressures in these vessels. Filling of the
tial to alter blood pressure. The large number of therapeutic agents used to treat high blood pressure in humans and animals, and the different mechanisms by which these agents have their effects, illustrate the diversity of factors that can alter blood pressure.
in normal animals, blood volume and arterial blood pressure are directly related.
increases or decreases in blood volume tend to produce similar changes in cardiac output and therefore in arterial blood pressure. in light of this relation and the goal of biologic systems to maintain homeostasis, it is predictable that decreases in blood pressure elicit physiologic responses designed to increase blood volume and increases in blood pressure elicit responses designed to reduce blood volume. The organs primarily responsible for bringing about changes in blood volume are the kidneys. Thus, blood volume regulation by the kidneys is one factor in the ultimate determination of arterial blood pressure. Many of the chemical agents and neural reflexes that regulate mean arterial pressure by their action on the heart and blood vessels also affect the ability of the kidneys to regulate blood volume by altering the rate of urine formation.This chapter discusses only some of the major regulators of arterial blood pressure and blood volume and for didactic purposes will classify these as neural reflexes, circulating (humoral) agents, and paracrine (locally produced) agents. Such classifications require generalizations, and there are many subtle interactions among these classes that will not be explored in this text.
Neural Reflexes
The arterial baroreceptor reflexes are the neural reflexes primarily responsible for the short-term or immediate regulation of arterial blood pressure. Neural receptors in the aorta and carotid arteries respond to changes in arterial pressure in these vessels, and this information is relayed to reflex centers in the brainstem. The efferent nerves for these reflexes are the autonomic nerves to the heart and the sympathetic vasoconstrictor nerves to both arterioles and veins. Decreases in arterial blood pressure bring about adjustments in these efferent nerves to increase heart rate, increase cardiac contractility, and promote arteriolar vasoconstriction and Venoconstriction. The overall effect tends to increase both CO and TPR so that blood pressure can be restored to its original level. increases in arterial blood pressure above some original level should elicit reductions in cardiac activity and relaxation of the vessels.
inhibition of vasoconstrictor and venoconstrictor nerves is the mechanism by which the reflex permits relaxation of the vascular smooth muscle.Neural receptors in the atria of the heart respond to changes in the volume of blood filling the atria, and afferent information from these receptors is relayed to brainstem reflex centers. The primary efferents involved in these reflexes are the sympathetic nerves to the kidneys. increases in atrial filling bring about reductions in sympathetic nerve stimulation of the kidneys, and this permits an increase in the urinary excretion of sodium chloride and water. This tends to reduce blood volume and therefore cardiac filling, cardiac output, and blood pressure. Reductions in atrial filling bring about increases in sympathetic nerve activity to the kidneys. This reflex also affects the secretion of renin from the kidneys (discussed later).
Humoral Agents
Renin is an enzyme released from the kidneys, and its release is regulated in part by sympathetic nerve activity to the kidneys and arterial blood pressure in the vessels perfusing the kidneys. increases in renal sympathetic nerve activity and/or reductions in arterial blood pressure to the kidneys elicit increases in renin secretion. Renin acts on a plasma protein substrate to produce a peptide, angiotensin i, which an enzyme converts to angiotensin II. Angiotensin ii constricts vascular smooth muscle, so it tends to increase TPR and arterial blood pressure. Angiotensin II also reduces the urinary loss of sodium chloride and water by its action on tubules in the kidney and by promoting the release of aldosterone from the adrenal cortex. The overall biologic effect of angiotensin II is to increase arterial pressure and blood volume.
At rest, the plasma levels of epinephrine and norepinephrine are relatively low, so their effects on cardiac function and vascular smooth muscle are relatively minor. However, plasma levels can increase significantly in highly stressed animals or in response to severe reductions in blood pressure or blood volume.
In these conditions, circulating epinephrine and norepinephrine promote increases in cardiac function and constrict vascular smooth muscle.Atrial natriuretic peptides (ANPs) are released from the atria of the heart in response to increases in blood volume and atrial filling. ANPs promote an increase in the urinary excretion of sodium and water by a direct action on tubules in the kidney. ANPs also reduce TPR by relaxing arteriolar vascular smooth muscle that was constricted by vasoconstrictor agents.
Paracrine Agents
Endothelial cells lining many blood vessels produce and release nitric oxide, a local vasodilator. Nitric oxide release by endothelial cells is subject to regulation by a variety of agents, and the importance of its overall role in the regulation of TPR in normal animals is controversial. Bacterial endotoxins are lipopolysaccharide components of the bacterial cell wall that are released when the cell is lysed. These endotoxins stimulate macrophages throughout an animal’s body to produce and release unusually large amounts of nitric oxide. General overproduction of nitric oxide causes widespread vasodilation and a severe drop in arterial blood pressure. These cardiovascular changes are part of a clinical syndrome, endotoxic or septic shock.
Endothelial cells also secrete a peptide, endo- thelin, which constricts vascular smooth muscle of arterioles. As with nitric oxide, a variety of agents (e.g., angiotensin II and norepinephrine) are known to stimulate endothelin release. Interestingly, circulating vasoconstrictors tend to increase the release of this locally produced vasoconstrictor.