Somatic motor systems
General anatomy and function
Key points
■ The motor system supports the body against gravity, establishes posture and allows voluntary movement to occur.
■ In general, UMN tracts in the lateral funiculus facilitate flexion, and those in the ventral funiculus facilitate extension.
The dorsolateral system of the spinal cord influences skilled and semiskilled movements of the distal limbs and the ventromedial system influences truncal and proximal limb muscles.The main functions of the somatic motor system are to:
(a) maintain tone to support the body against the effects of gravity;
(b) provide a stable postural background against which movement can occur;
(c) initiate, modify and terminate voluntary movement (Fig. 5.3).
Fig. 5.3 Hector (inside the box) using somatic motor systems to perform function ‘a’, especially for the neck muscles, while Harriet is doing all three functions as she explores outside the box.
The UMN system functions to initiate, regulate, modify and terminate the activity of the LMN. In turn, the UMNs are controlled by the executives of the motor system (Chapter 4), which plan and coordinate static and dynamic motor function. The UMNs of primary importance in quadrupeds arise from nuclei in the brainstem and the motor cortex of the forebrain. They influence LMNs supplying striated muscle of the head, body and limbs using cranial and spinal nerves.
The UMNs may stimulate or inhibit the LMNs. The LMNs connect to flexor or extensor muscles. In the spinal cord, UMN tracts are found in the lateral and ventral funiculi. As a general rule, UMN tracts in the lateral funiculus facilitate flexion and those in the ventral funiculus facilitate extension. An alternative nomenclature for spinal cord motor tracts is the dorsolateral and ventromedial systems based on their location in the spinal cord.
The dorsolateral system (corticospinal and rubrospinal tracts) influences skilled and semiskilled movements, especially of the distal limb muscles, and these are primarily flexor muscle although the lateral corticospinal tract influences both extensors and flexor muscles of the distal limb. The ventromedial system (vestibulospinal, reticulospinal and tectospinal tracts) influences truncal and proximal limb muscles; these are primarily extensors (see Fig. 4.5).UMN: Pyramidal and extrapyramidal systems
Key points
■ UMN systems of the spinal cord are classified anatomically into the extrapyramidal and pyramidal systems.
■ Extrapyramidal fibres, originating from UMN nuclei located throughout the brain, do not pass through the pyramids of the medulla oblongata. They influence LMNs of cranial and spinal nerves and function primarily to regulate posture and rhythmical, semi-automatic motor movements. The extrapyramidal system is the dominant system in domestic animals.
■ Pyramidal fibres, originating in the motor cortex of the cerebrum, pass through the pyramids into the spinal cord forming the corticospinal tract. Corticonuclear fibres arise in the motor cortex and synapse on cranial nerve nuclei in the brainstem. These tracts are responsible for complex, learned, voluntary movements. These pathways are more important in primates and humans than quadrupeds.
■ With the exception of the vestibulospinal tract, both systems decussate and principally innervate γ-LMN.
Functionally and anatomically, UMN systems are divided based on their origin, into those systems originating from the motor cortex and those originating from other UMN centres throughout the brain. Fibres originating from the motor cortex and synapsing on LMN (corticonuclear and corticospinal tracts) are used for learned, skilled movement, whereas the other UMN systems are more important in posture, locomotion and semi-automatic movements such as breathing. Both systems influence cranial nerve nuclei of the brainstem and travel caudally into the spinal cord.
The continuation of the corticospinal tract in the medulla oblongata is through the pyramids; the tracts originating from other brain areas do not pass through the pyramids. This has given rise to classifying the two systems into pyramidal and extrapyramidal, however, most corticonuclear fibres do not pass through the pyramids, thus the nomenclature is not precise.The output from the motor cortex travels via the corona radiata, internal capsule and crus cerebri to the brainstem (see Figs. 1.13, A3, A15-18). There the corticonuclear fibres synapse on cranial nerve nuclei (CN III-VII, IX-XII) in the midbrain, pons and medulla oblongata. The remaining fibres form the corticospinal tract and continue caudally as two longitudinal bands of axons on the ventral surface of the medulla oblongata. In cross-section, these bilateral bands are somewhat triangular in shape, especially in humans, and are known as the pyramids, hence ‘pyramidal system’ (see Figs. A3, A21-25). The corticospinal/corticonuclear system functions in skilled, voluntary movement and hence dexterity in a species is related to its degree of pyramidal development. Corticospinal fibres account for 20-30% of the total spinal cord white in primates but only about 10% in carnivores. The corticospinal tract is also well developed in raccoons, an animal noted for its dexterity, and the horse has a well-developed corticonuclear system synapsing in the facial nucleus, for lip movement.
The extrapyramidal system comprises diverse tracts originating from UMN nuclei located throughout the brain. The extrapyramidal system functions to stimulate postural muscles for tonic support against the effects of gravity (aiding stretch reflexes), to generate a stable postural platform against which other movement can occur, and recruit spinal reflex circuitry for voluntary movement. It can also initiate, modulate and terminate voluntary movement (e.g. locomotion) and controls muscular activity associated with visceral activities such as cardiac and respiratory function and urination.
In animals of traditional veterinary interest, the extrapyramidal system is far more important for motor function than is the pyramidal system (Fig. 5.4).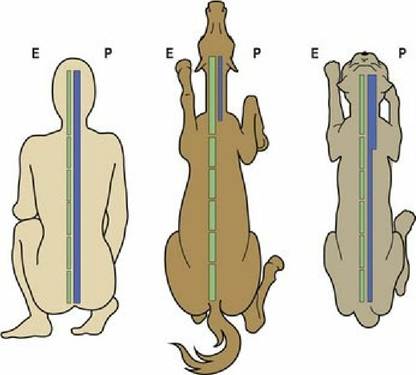
Fig. 5.4 The degree of development of the extrapyramidal and pyramidal tracts varies markedly in the human, horse and cat. The dashed line represents the extrapyramidal tract (E) on the left in each figure, while the solid line represents the pyramidal tract (P) on the right in each figure
(redrawn with permission from Figure 8.50, Dyce, Sack and Wensing, Textbook of Veterinary Anatomy, Fourth Edition, Saunders).
Note that the red nucleus of the midbrain receives direct input from the ipsilateral motor cortex and projects the length of the spinal cord as the rubrospinal tract in the lateral funiculus, adjacent to the corticospinal tract. It is of major importance in domestic species. In dogs, it is considered to be the main tract controlling voluntary movement and acts as an indirect corticospinal tract.
In summary, the extrapyramidal system is responsible for maintaining and changing posture, rhythmical activities such as locomotion and chewing, and semi-automatic activities such as feeding. The rubrospinal tract also appears to have a role in semi-skilled movements of the distal limb. The pyramidal system is responsible for complex, learned, voluntary movements, such as the kitten playing with the Christmas tree ornament or feather (see Fig. 9.2). These voluntary movements are superimposed on an appropriate postural platform that is coordinated by the cerebellum and enacted by the extrapyramidal system.
Termination of UMN tracts on LMN: Descending UMN tracts usually synapse on interneurons, most of which then connect to γ-LMNs. The vestibulospinal tract also connects to α-LMN. Stimulation of the γ- LMNs increases the stretch of the muscle spindle causing firing of the 1a afferents; this stimulates the α- LMNs causing the muscle to contract.
Significant amplification of the descending UMN input occurs via γ-1a-α circuit activation. It has been suggested that in dogs only 10-20% of descending UMN pathways need to be intact after a severe spinal cord lesion for locomotion to occur. Thus, animals with chronic, severe spinal cord compression, as in Fig. 5.5 may still be able to ambulate.
Fig. 5.5 Dog, cervical spinal cord. Myelogram in which the spinal cord is outlined by radio-opaque
contrast agent; there is marked compression of the C6-C7 spinal cord. This dog was still walking quite well despite the lesion; it did, however have moderate proprioceptive deficits.
Tract decussation
Many motor tracts (e.g. corticospinal, rubrospinal, tectospinal) decussate as they travel between the origin and termination, thereby influencing the contralateral side of the body. The vestibulospinal tract is largely ipsilateral in that it stimulates the ipsilateral α-LMNs supplying extensor muscles, but it also inhibits contralateral extensor tone. The reticulospinal tracts are considered to influence both sides by some authors, or be mainly ipsilateral.
Inhibition versus excitation
The inhibitory pathways tend to dominate the excitatory/facilitatory pathways. This is necessary to decrease the effect of extensor (antigravity) muscle dominance over the flexor muscles, especially in the limbs. The main inhibitory pathway is the medullary reticulospinal tract. This tract exerts a massive inhibitory influence on γ-LMNs and hence indirectly on α-LMNs. The vestibulospinal, tectospinal, pontine reticulospinal and rubrospinal tracts are facilitatory to LMNs (see Table. 4.3). Severe spinal cord lesions can block the influence of descending inhibition, thus the animal may exhibit some spasticity/increased extensor muscle tone and exaggerated spinal reflexes (see Fig. 4.2).
UMN tracts
Table 5.1 lists the tracts of the non-cortical (extrapyramidal) and cortical (pyramidal) systems, their pathways and their functions.
Table 5.1 Motor tracts of the pyramidal and extrapyramidal systems
| Tract | Function |
| Extrapyramidal tracts | These tracts form the bulk of the caudaliy directed fibres in domestic animals |
| 1. Rubrospinal tract (LF) Originates in the red nucleus (midbrain), axons decussate immediately and pass through the brain stem, synapsing on cranial nerve nuclei (V, VII and nucleus ambiguus). The tracts continue into the lateral funiculus extending the length of the spinal cord | Facilitatory to flexor muscles. It functions in semi-skilled movements in cats (less so in dogs) and humans, and in postural control (e.g. squatting/sitting) and locomotion (limb protraction) in other domestic animals |
| 2. Medullary reticulospinal tract (LF) Originates from the medial medullary reticular formation. The fibres mostly decussate within the reticular formation and descend in the lateral funiculus to terminate on interneurons along the length of the spinal cord | Strongly inhibitory to γ-LMNs of extensor muscles (ipsilateral and contralateral). This tract functions to suppress standing and other antigravity activities |
| 3. Pontine reticulospinal tract (VF) Originates in the pontine reticular formation, with ipsilateral projection throughout the ventral funiculus of the spinal cord terminating on interneurons | Facilitatory to ipsilateral γ-LMNs of anti-gravity/extensor muscles to maintain standing posture |
| 4. Lateral vestibulospinal tract (VF) Originates primarily from the lateral vestibular nucleus, descends ipsilaterally in the ventral funiculus to all levels of the spinal cord terminating on interneurons especially at the intumescences. Some fibres decussate to inhibit contralateral LMNs | Facilitatory to ipsilateral extensors (α- and γ-LMNs), inhibitory to ipsilateral flexors and contralateral extensors It is always active as there constant input to the vestibular nuclei about static head position from the sacculus and utriculus (see Chapter 8) |
| 5. Medial vestibulospinal tract (VF) Originates primarily from the other three vestibular nuclei (medial, rostral and caudal), the tract descends in the medial aspect of ventral funiculus and the medial longitudinal fasciculus of the VF, primarily to cervical and cranial thoracic segments | The neurons of this tract are activated by angular acceleration of the head, which is detected in the ampullae of the semi-circular ducts. Stimulation reinforces activity in the cervical and thoracic limb muscles helping to maintain posture despite changing positions of head |
| 6. Medial longitudinal fasciculus (VF) Originates from all four vestibular nuclei (and other nuclei including CNN nuclei). It descends in the ventral funiculus terminating on interneurons at different cord levels. For example, in the cervical and cranial thoracic cord (cat) or extends the length of the cord (dog) | Functions in conjunction with the medial vestibulospinal tract to coordinate trunk and limb movement with head and eye movement |
| 7. Lateral tectotegmentospinal tract (LF) Originates from the rostral colliculus of the midbrain tectum, travels ventrally into the tegmentum through brainstem into lateral funiculus of the spinal cord, terminating in the intermediate horn of C8-T2 segments | Functions as UMN to sympathetic innervation supplying smooth muscle of the head, and the eye for pupillary dilation |
| 8. Medial tectospinal tract (VF) Originates from the rostral and caudal colliculi of the midbrain, decussates and travels in the ventral funiculus to terminate in the cervical segments | Function: the tectal neurons receive input from visual and auditory pathways and their output is involved in reflex postural movements of head and neck in response to auditory and visual stimuli |
| Pyramidal tracts | These tracts comprise only a small proportion of motor tracts in non-primates |
| 1. Corticonuclear tract Originates in the motor cortex of the cerebrum, travels via the internal capsule, crus cerebri, longitudinal fibres of the pons, without synapsing to terminate on brain stem motor nuclei (III, IV, V, VI, VII, and nucleus ambiguus (IX, X, XI) and XII, usually bilaterally | Function: primarily involved in discrete/skilled voluntary movement affecting the head, limbs, neck and trunk |
| The corticonuclear tract is related to discrete movements of the facial muscles. It is well developed in animals such as horses in which it aids skilled lip movement | |
2. Corticospinal tract (LF, VF (DF)
Originates as above and descends without synapsing via the medullary pyramids into the spinal cord, travelling via the named funiculus, to terminate on spinal cord grey matter. May synapse directly onto α-LMNs.
(a) lateral corticospinal tract (70-90% of pyramidal fibres)
(b) ventral corticospinal tracts (of much less importance and species variable)
(c) a small dorsal corticospinal tract is found in some types of animals (e.g. rodents) extending as far caudally as C5
Lateral CST: Fibres facilitating skilled, discrete movement of the extremities are located in the lateral aspect of the lateral CST. These may act in conjunction with the rubrospinal tract. In primates/humans this system is responsible for fine digital movement. The lateral CST is not well developed in most quadrupeds except for highly dexterous animals like raccoons Ventral CST: Fibres mediating neck and trunk movements (including urinary bladder function) are usually located in the ventral CST. In the absence of a ventral CST, they are located in the medial aspect of the lateral CST
LF = lateral funiculus; VF = ventral funiculus.
See also Fig. 4.5 for tract location in the spinal cord and Table 4.3.
Both the extrapyramidal and pyramidal spinal pathways usually have three neurons. Neuron one is the motor command centre (motor cortex or motor nuclei of the brainstem); neuron two is a short interneuron in the grey matter; neuron three is a ventral horn neuron, which are mostly γ-LMN, but some tracts (e.g. vestibulospinal) may stimulate α-LMN.
Additional comments on certain motor tracts are listed below.
1. Lateral vestibulospinal tract: This is a phylogenetically ancient tract, and facilitates extensor (antigravity) muscle activation. Such activation had to occur as soon as animals became subject to prominent forces of gravity, i.e. land-dwellers. The lateral vestibular nucleus receives input from sacculus and utriculus of the inner ear, which sense static head position. As vestibular input from the sacculus and utriculus is constant, so is the outflow via this tract. Thus the vestibulospinal tract plays a significant role in maintenance of posture against the effects of gravity and activation of extensor muscles to cope with changes in posture. It is usually strongly inhibited by the cerebellum and the cerebrum. Unsuppressed function of the lateral vestibulospinal tract is partly responsible for the limb and spinal extension observed in decerebrate rigidity.
2. Rubrospinal tract: Phylogenetically, this is the youngest of the extrapyramidal tracts, but older than the corticospinal tract. It is somatopically organised within the cord with the pelvic limbs being lateral to the thoracic limbs. In dogs, it is the most important pathway for the execution of voluntary movement. In the decerebrate animal, if the red nucleus is preserved, then sitting, crouching, walking, climbing and the righting reflex can still occur. In humans, the rubrospinal tract is responsible for infants crawling and adults swinging their arms while walking; irregular arm swing is a prominent symptom in humans with dysfunction of the extrapyramidal system (Parkinson’s disease).
3. The corticonuclear/corticospinal systems: The pyramidal system is only present in mammals; it is not found in birds, reptiles, amphibians or fish. Within mammals there is a great deal of variation in its development and location. In cats the tract extends the length of the cord, but in ungulates it ends in the cervical region. Its greater development in humans and primates reflects the fact that, phylogenetically, it is the youngest tract. Like the motor cortex, it is somatopically organised.
This is a three-neuron system in animals. The first neuron is in the motor cortex, which is located just rostral to the cruciate sulcus. In humans two additional motor areas are also present. The supplementary and second motor areas are located on the medial surface of the cerebral hemisphere adjacent to the primary motor area. The cat also has a supplementary motor area. The primary motor areas are somatopically arranged, giving rise to the homunculus in humans and felunculus in cats (see Fig. 4.14). The second neuron is an interneuron usually located in the base of the dorsal horn in the spinal cord, or within the motor nucleus of brainstem cranial nerve nuclei. The third neuron is located within the cranial nerve motor nucleus or the ventral horn of the spinal cord. This neuron is usually a γ-LMN but may occasionally be an α-LMN. The interneuron may be missing in the primate corticospinal tract controlling hand and foot movement, resulting in a two-neuron system with shorter conduction times. This suggests a trend to greater specialisation and is reflected clinically. Damage to the corticospinal system will have more profound effects on animals that have well-developed, two-neuron systems, such as humans and primates (see Fig. 4.9).
The corticonuclear tract projects to midbrain, pontine and medullary nuclei associated with cranial nerve motor function. Decussation occurs just before the fibres reach the motor nucleus. It influences all cranial nerve nuclei innervating striated muscle, controlling voluntary movement of the eyes, face, tongue, jaws, pharynx and larynx.
The corticospinal tract functions in voluntary movement of the limbs, trunk and tail. The tract is facilitatory to both flexors and extensors and used for fine distal control of the digits.
Lateral corticospinal tract: In the dog, 75% of fibres cross in the pyramidal decussation at the medulla/spinal cord junction to form the lateral corticospinal tract in the lateral funiculus (see Figs. A24- 25). This tract has overlapping distribution with rubrospinal tract. The lateral corticospinal tract projects throughout the spinal cord, but is concentrated in the cranial region.
Ventral corticospinal tract: The remaining 25% of fibres from the medullary pyramids travel ipsilaterally in the ventral funiculus as far as the mid-thoracic region and decussate just before terminating.
A dorsal corticospinal tract is found in some ungulates and rodents.
Clinical signs of disease in the pyramidal system. In humans, damage to the pyramidal system is much more significant than in domestic mammals. We are prone to ischaemic lesions affecting the motor cortex or internal capsule (e.g. cerebrovascular accident or ‘stroke’), which can result in contralateral paresis/paralysis. In domestic mammals, ischaemic lesions are much less common and pyramidal function is less important. Experimentally, destruction of the motor cortex in animals results in signs that are relatively mild, but may include stumbling, dysmetria and altered tone on the contralateral side. Dogs had no deficit in the gait after experimental removal of the motor area, but did have deficits in contralateral postural reactions. Experimental sectioning of crus cerebri or pyramids in dogs had no effect on gait.
4. Other caudally directed tracts in the spinal cord
(a) Fibres from the locus ceruleus in the pons travel caudally in the lateral funiculus synapsing in both the dorsal and ventral horns. The fibres release norepinephrine at the termination, which inhibits neuronal function, especially that created by noxious stimuli.
(b) Fibres from the raphe magnus nucleus in the rostral medulla oblongata travel caudally in the lateral funiculus to synapse in the dorsal horn. They release serotonin which increases the threshold of response to noxious stimuli.
Dysfunction of UMNs and LMNs
Key points
■ UMNs are the managers and may be considered as ‘central motor neurons’ due to their location. LMNs are the workers and may be considered as ‘peripheral motor neurons’.
■ Clinically, the loss of LMNs is more significant than equivalent damage to UMNs.
■ The different clinical signs resulting from UMN and LMN dysfunction can be remembered by the mnemonic the ‘Neuro RAT’: Reflexes, Atrophy and Tone.
The LMN is regarded as the final common pathway. Upper motor neurons of many tracts may influence a LMN, but the final manifestation of their activity is mediated through that LMN. The LMN can be either inhibited or stimulated, causing the decreased or increased muscle contraction, respectively. The concept of the LMN being the final common pathway is clinically relevant. A lesion that is cranial to the location of the LMN damages UMN tracts affecting that LMN. Even if many of the UMN tracts are lost, the LMN and neuromuscular junction is still intact, therefore the muscle can be stimulated to contract. The number of interneuronal connections to that LMN is vast, thus UMNs can influence it by diverse routes (see Fig. 4.9). However, if the LMN is lost, then the NMJ will degenerate and the muscle will not contract, even if the UMN circuitry is intact. Thus LMN disease usually has a worse prognosis than UMN disease.
UMN versus LMN signs
When a nerve is badly damaged, then distal to the site of the lesion, the axon and its synaptic connections will degenerate. A lesion in the thoracolumbar spinal cord can cause neurological signs in the pelvic limbs by damaging cranially directed sensory tracts and caudally directed UMN tracts. The animal will show proprioceptive deficits, sensory deficits and paresis or paralysis, depending on the lesion severity. A lesion in the lumbosacral spinal cord will also cause sensory and motor deficits in the pelvic limbs, but certain motor signs will be different to those arising from thoracolumbar lesions. The thoracolumbar lesion will damage UMN tracts causing UMN signs to the pelvic limbs while the lumbosacral lesion will damage LMNs causing LMN signs to the pelvic limbs. The distinction between UMN and LMN signs is critical for localising a spinal cord lesion (Fig. 5.6 and Table 5.2).

Fig. 5.6 The ‘Neuro RAT’ is a useful mnemonic for remembering the differences between upper and lower motor neuron signs: Reflexes, Atrophy, Tone.
Table 5.2 Clinical signs due to UMN versus LMN lesions - remember the ‘Neuro RAT’. Note: thinking of UMNs as central motor neurons and LMNs as peripheral motor neurons may facilitate understanding where a lesion is sited and how that lesion may cause dysfunction
| ⅛l | UMN disease (damage to the UMNs) | LMN disease (damage to the LMNs) |
| Reflexes | Normal to increased | Decreased to absent |
| Atrophy | Disuse: Mild, generalised | Neurogenic: severe, specific muscles |
| Tone | Normal to increased | Decreased to absent |
Affected limbs in animals with neurological disease may be described as having upper motor neuron signs or lower motor neuron signs. This classification means that there is damage to either the UMNs or the LMNs, respectively.
Upper motor neuron signs
The UMN tracts are excitatory or inhibitory to LMNs, and LMNs innervate either extensor (antigravity) or flexor muscles. In animals extensor (anti-gravity) muscles are stronger than flexor muscles, therefore loss of UMN inhibition after a lesion can result in increased tone and reflex activity in the limbs caudal to the lesion (see Fig. 4.2). Characteristically, UMN lesions may cause exaggerated stifle extension in the patellar reflex, especially with chronic lesions. Loss of other UMN tracts that facilitate LMNs and recruit spinal reflex circuitry for locomotion results in reduced or complete loss of movement (paresis or paralysis). In animals, such as horses, in which it is difficult to assess the patellar reflex, UMN paresis is assessed by testing the ability of the horse to resist pulling on the tail. Horses with acute UMN lesions are commonly profoundly paretic, far more so than an ambulant horse with a LMN lesion; if a horse had such profound LMN paresis, it would be recumbent (Fig. 5.7). Increased muscle tone and reflex activity are two cardinal signs of UMN dysfunction. The third sign used to differentiate UMN and LMN lesions is the type of muscle atrophy in the affected limbs. The atrophy in UMN disease is due to disuse. Thus it is generalised caudal to the lesion and is usually mild. Note that lameness in horses and loss of correct weight-bearing may also result in marked disuse atrophy; this atrophy needs to be distinguished from atrophy due to UMN lesions.

Fig. 5.7 (A) Normal horse, (B) horse with UMN paresis. Pulling the tail while the horse is moving should result in ipsilateral pelvic limb extension, as is demonstrated by the horse in (A). Horses with UMN dysfunction (B) are unable to achieve this and can easily be pulled to the side. Horses with LMN paresis that are still strong enough to ambulate are able to resist this tail pull better than horses with UMN dysfunction.
Lower motor neuron signs
Dysfunction of LMNs can occur either due to damage to the nerve cell body in the CNS, or due to damage to the axon in the periphery. Distal to the lesion, both the axon and the neuromuscular junction will degenerate. The efferent portion of any reflex arcs involving these muscles is lost, resulting in decreased or absent reflexes. Due to degeneration of the neuromuscular junction, acetylcholine will not be released from the nerve terminal, and the muscle fibres will not be stimulated to contract. Muscle tone will be reduced or absent (depending on how many axons are lost) due to loss of γ-LMN activation. Denervation of muscles usually results in rapid, severe muscle atrophy. Atrophy may cause as much as 50% of muscle bulk being lost within 2-4 weeks of injury. This is called LMN or neurogenic atrophy and will affect only those muscles that have lost their LMN input. Identifying the specific muscles that are atrophied can be used to identify precisely the involved nerves and/or spinal cord segments. For example, damage to LMN in the suprascapular nerve, supplying the supraspinatus muscle can occur with lesions affecting the caudal cervical spinal cord segments or the cranial brachial plexus (see Figs 5.8, 4.7A and 13.4).
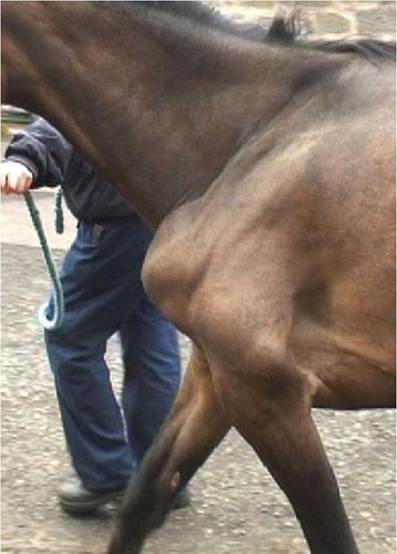
Fig. 5.8 Horse with brachial plexus lesion secondary to trauma resulting in LMN signs and neurogenic atrophy of the musculature of the proximal thoracic limb and shoulder. The limb was abnormally abducted and had severe, specific muscle atrophy.
Executive motor function
The neural circuitry involved in planning motor activity is located in the forebrain. This executive manager of the motor system draws on a variety of sensory inputs (from association areas) as well as the limbic system and cerebellum that deal with behaviour and movement coordination (Chapter 7 and 11). It also draws on memory centres of the limbic system and parietal lobe. The motor planning centres also have a database in the basal nuclei which are thought to store fragments of complex, ritual-like motor programmes. Thus the motor planning centres have a number of neural loops that connect to different areas of the brain. It uses the loops to access information from those diverse regions and bring that information back to the executive management for use in planning motor activity.
The cerebral cortex has two main feedback loops to the cerebellum that ultimately influence UMN function. The first loop involves the corticopontocerebellar pathway and is used specifically for motor function that will be expressed via the corticonuclear/corticospinal tracts. Consequently, the development of this system is much greater in humans and primates than in domestic mammals. Output from the cerebral cortex, travelling through the internal capsule and crus cerebri, synapses in nuclei of the pons. The second neurons in this corticopontocerebellar pathway decussate and ascend via the middle cerebellar peduncle into the cerebellum. The return pathway from the cerebellar cortex synapses in the deep cerebellar nuclei (e.g. dentate nucleus). Post-synaptic fibres decussate and exit the cerebellum via the rostral cerebellar peduncle, travel rostrally to the synapse in the thalamus and then to the cerebral cortex.
The second loop from the motor planning centres to the cerebellum ultimately influences extrapyramidal function. It travels to the olivary nucleus in the medulla oblongata, via the caudal cerebellar peduncle to the cerebellum and back via the thalamus to the cerebral cortex or basal nuclei. Again, these pathways decussate twice. The functions of these feedback loops are covered in Chapter 7 on the cerebellum.
Basal nuclei and corpus striatum
Key point
■ Basal nuclei comprise grey matter deep in the forebrain and midbrain. They function in feedback circuits with the cerebrum to modify cortex output.
Most of the grey matter of the cerebrum is superficially located in the cerebral cortex; the basal nuclei form some of the deeply located, telencephalic grey matter. The basal nuclei comprise structures located in the forebrain and midbrain, but the main components are the caudate and lentiform nuclei (globus pallidus and putamen) in the cerebrum. The caudate nuclei are prominent and bulge into the ventrolateral aspect of the lateral ventricles (Fig. 5.9).
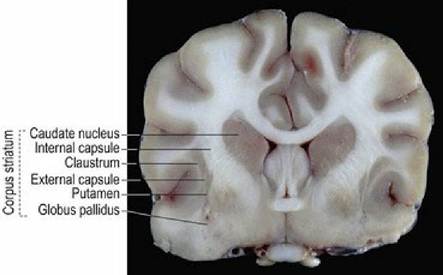
Fig. 5.9
Transverse section of the canine brain at the level of the rostral commissure (see Figs. A14-16).
The basal nuclei and intervening white matter are arranged from medial to lateral, as the caudate nucleus, the internal capsule (white matter tracts comprising both afferent and efferent fibres connecting between the cerebral cortex and the brainstem), the lentiform nuclei, the external capsule and the claustrum. This alternating arrangement of grey and white matter is called the corpus striatum (L = striated body).
Inputs to the basal nuclei originate mainly in the cerebrum, the thalamus and the midbrain and most are delivered to the caudate nucleus. The globus pallidus is the only basal nuclear component from which efferent fibres leave to connect with other areas of the brain.
Despite their size and prominence, the functions of the basal nuclei are not clearly defined in animals. They seem to function in feedback circuits with the cerebrum (via the thalamus) ultimately modifying motor cortex output. They may also be involved in arranging complex movements that are in frequent use (e.g. feeding or territorial behaviour) and may be considered to store fragments of programmes used for running motor functions that have a specified sequence (ritual) of movements. Unlike the situation in humans and primates, the subcortical centres in domesticated animals can function to a greater extent without cortical input, thus the functional impact of even large motor cortex lesions may be negligible in those species. Additionally, primary lesions in the basal nuclei causing clinical dysfunction are not commonly recognised in animals compared with humans (e.g. Parkinson’s disease). However, dysfunction of connections between the basal nuclei and cerebrum may cause circling and propulsive activity in animals with forebrain lesions (see Fig. 4.10). In horses, ingestion of plants of the Centaurea family causes severe necrosis of the basal nuclei; this results in devastating rigidity of muscles associated with eating and swallowing.