Structure of the Foot
Bones and Cartilages
Anatomy of the carpus and tarsus are discussed in Chapters 4 and 6. In the thoracic limb, the large metacarpal III (cannon bone) and medial (II) and lateral (IV) metacarpal bones (splints) articulate proximally with the carpus, and the cannon bone articulates distally with the proximal phalanx and two proximal sesamoid bones.
similarly, in the pelvic limb metatarsals II to IV articulate proximally with the tarsus, and the cannon bone (metatarsal III) articulates distally with the proximal phalanx and the two proximal sesamoid bones. As a rule, metatarsal III is somewhat longer and rounder in cross-section than metacarpal III.The three phalanges include (1) the proximal phalanx (long pastern bone), (2) the middle phalanx (short pastern bone), and (3) the distal phalanx (coffin bone) (Fig. 14-2). The proximal phalanx articulates with the cannon bone at the fetlock (metacarpophalangeal and metatarsophalangeal joints) and with the middle phalanx at the pastern (proximal interphalangeal joint). Middle and distal phalanges articulate at the coffin joint (distal inter- phalangeal joint).
The two proximal sesamoid bones lie at the palmarIplantar surface of the fetlock. The unpaired distal sesamoid (navicular) bone lies at the palmar or plantar aspect of the coffin joint.
The distal phalanx features medial and lateral palmarIplantar processes to which are attached rhomboidal ungual cartilages (formerly collateral cartilages) (Fig. 14-3). The dorsal margins of these cartilages extend proximal to the hoof, where they are palpable under the skin near the heels of the foot. Flexibility of the ungual cartilages probably aids in pumping blood away from the foot.
Trauma (by either direct injury or chronic heavy work) may ossify the ungual carti-
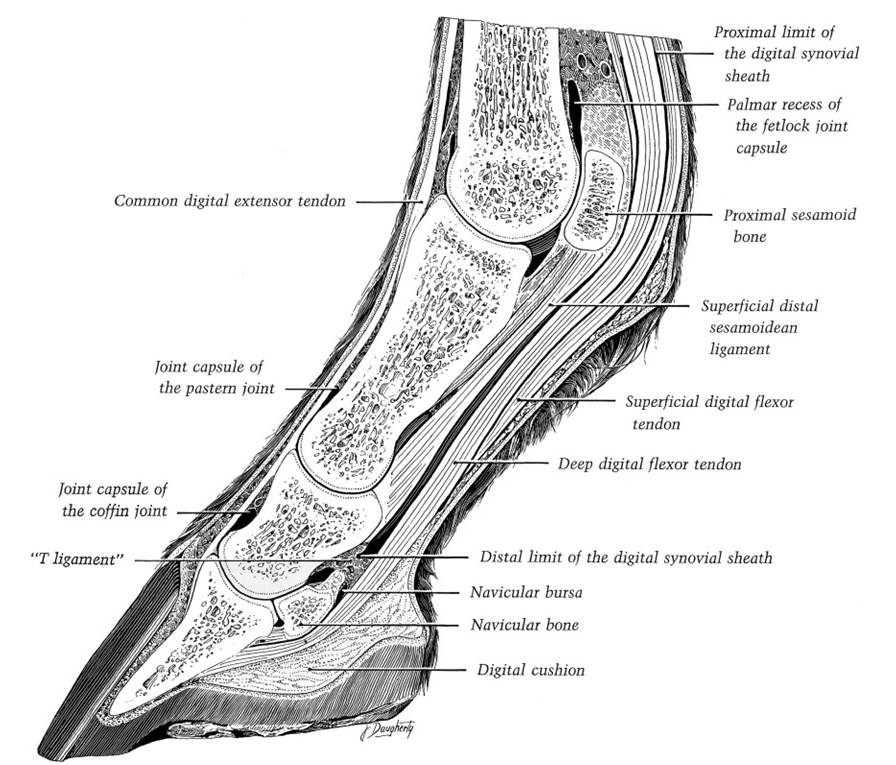
Figure 14-2.
Sagittal section of the equine digit. (Reprinted with permission of Wiley-Blackwell from StashakT.S. Adams’ Lameness in Horses. 5th ed. Baltimore: Lippincott Williams & Wilkins, 2002.)
lages; this produces a condition called sidebone (Fig. 14-4). Lameness may or may not accompany sidebone. Penetrating injury in the region of the coronary band may lead to infection of the ungual cartilage and the development of chronic draining tracts. This is called quittor.
Cornified Tissues
The hoof is a cornified modification of epidermis, under which lies a vascular layer, the corium (Fig. 14-5). The region where hairy skin changes to hoof is the coronary band (or coronet). The hoof wall is the portion of the hoof that is visible when the horse is standing. it is divided into a toe in front and medial and lateral quarters on the sides, and medial and lateral heels behind that turn sharply forward at the angles to be continued by the bars on the bottom of the hoof (Fig. 14-6).
Pigmentation of the germinal layer of epidermis determines the color of the hoof wall. White hoofs are found where the hair at the coronary band is also white, and dark
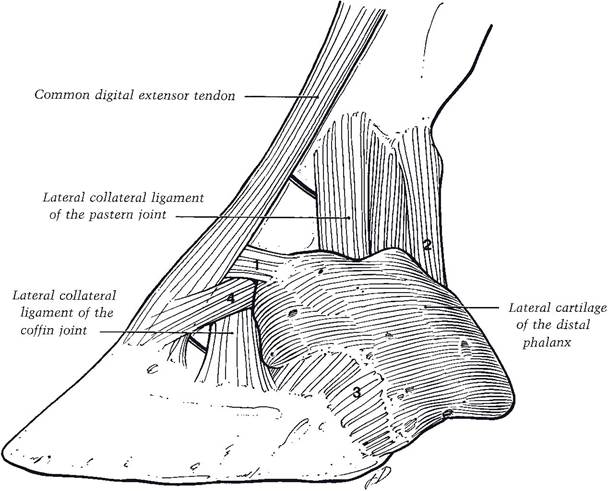
Figure 14-3. Lateral view of the equine digit. The ungual cartilage (lateral cartilage of distal phalanx) is stabilized by four ligaments. (Reprinted with permission of Wiley-Blackwell from Stashak T.S. Adams’ Lameness in Horses. 5th ed. Baltimore: Lippincott Williams & Wilkins, 2002.)
hoofs are associated with dark hair in this area. The widely held conviction that black hoofs are stronger than nonpigmented (white) hoofs has no scientific basis but remains a strongly held belief with much anecdotal support.
A thin band of perioplic corium at the coronary band is associated with the layer of epidermis that produces the thin, waxy periople (stratum tectorium) on the surface of the hoof wall. A wider band of coronary corium underlies the portion of the epidermis that generates the bulk of the hoof wall (often called the stratum medium).
The coronary corium features very prominent papillae that interdigitate with the coronary epidermis; hoof wall produced by epidermis adjacent to these papillae assumes a tubular configuration. This tubular horn can be distinguished from surrounding intertubular horn on microscopic examination. Both contribute to the stratum medium (Fig. 14-7).The periosteum on the convex surface of the distal phalanx blends with longitudinal leaves of corium called the laminar corium, which, because it is well innervated, is often called the sensitive laminae of the hoof. The sensitive laminae interdigitate with epidermal laminae (Figs. 14-7 and 14-8), which, because they are not innervated, are described as insensitive laminae. The large surface area afforded by the thousands of interdigitating laminae creates a strong connection between the distal phalanx and the hoof wall. Most of the weight of the horse is transferred by the laminae to the hoof wall rather than directly to the sole of the foot.
Inflammation of the laminae is laminitis. Because the hoof is a relatively closed space, such inflammation is extremely painful. Laminitis of sufficient severity can result in detachment of insensitive from sensitive laminae so that the intimate association between hoof wall and distal phalanx is lost (Fig. 14-9). In such a case, the distal phalanx may rotate downward, and the hoof wall grows abnormally, producing an irregular
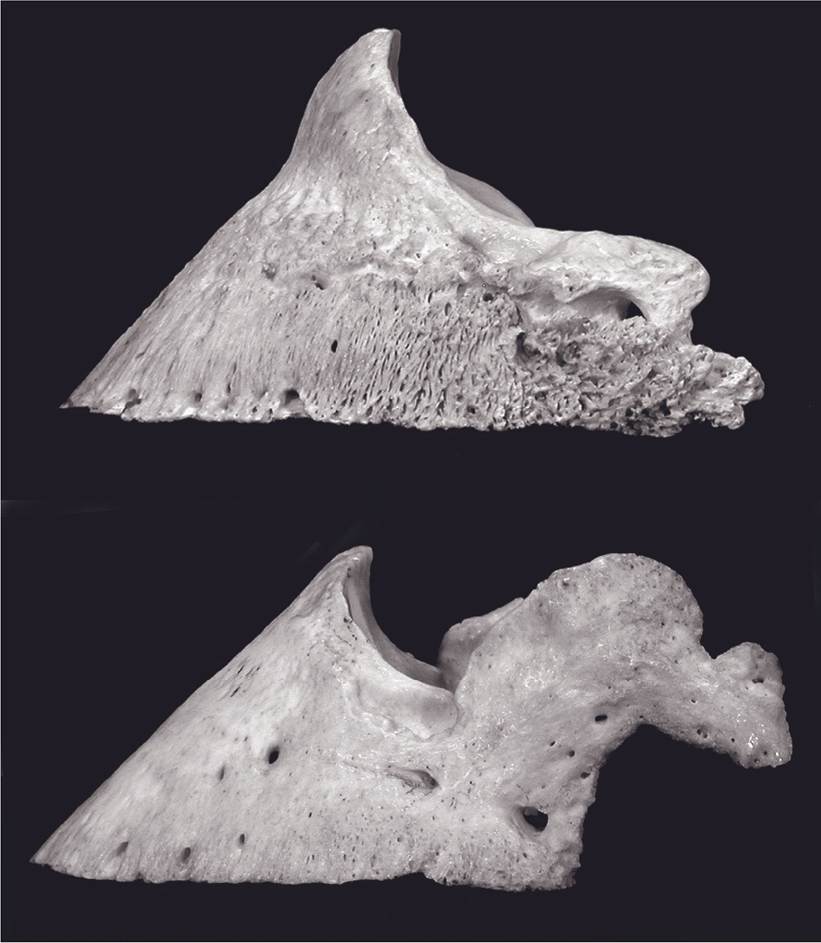
Figure 14-4. Lateral views of distal phalanges. Top) Normal distal phalanx. Bottom) Ossification of ungual cartilage seen as an irregular bony projection from the palmar process of this phalanx. This condition is known as sidebone. (Photo supplied by A. Fails. Colorado State University, Fort Collins, CO.)
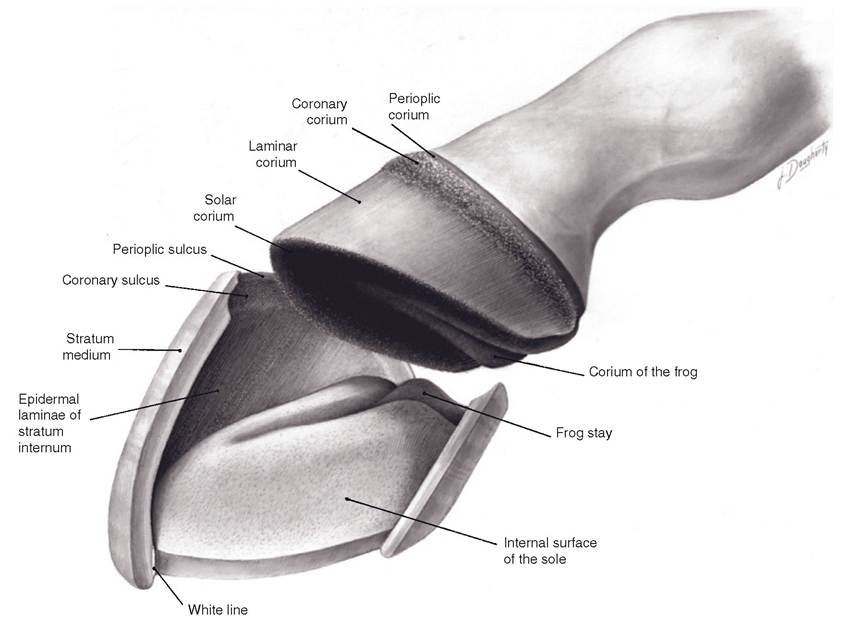
Figure 14-5. Dissected view of the relation of the hoof to the underlying corium.
(Reprinted with permission of Wiley-Blackwell from Stashak T.S. Adams’ Lameness in Horses. 5th ed. Baltimore: Lippincott Williams & Wilkins, 2002.)flared wall and up-curled toe. This chronic condition is founder.
The sole of the foot is a concave keratinized plate that attaches to the palmarIplantar surface of the third phalanx. it includes the entire ground surface of the foot not occupied by the wall or the frog (discussed later). Normally, the concavity of the sole allows the wall and frog to bear most of the weight and wear (Fig. 14-6).
Laypeople and farriers recognize a narrow band of the deepest part of the stratum medium, which is typically slightly lighter in coloration than the rest of the hoof wall. This is the white line. The white line is useful as a landmark for driving nails in shoeing. A properly directed nail started at or outside the white line will not touch any sensitive structures of the foot.
The frog (cuneus unguis) is a specialized, wedge-shaped pad near the heels of the foot (Fig. 14-6). The horn of the frog is relatively pliable, and the compression of the frog against the ground is important for return of blood from the foot. Deep grooves (collateral sulci or para- cuneal sulci) demarcate the sides of the frog from adjacent sole, and a single central sulcus corresponds to a spine of tissue called the frog stay on the dorsal (deep) side of the frog (Fig. 14-5). Deep to the frog is the digital cushion, a thick wedge of fibrofatty tissue (Fig. 14-2).
Tendons
No muscle bellies extend below the carpus or tarsus in the mature horse. The tendons of
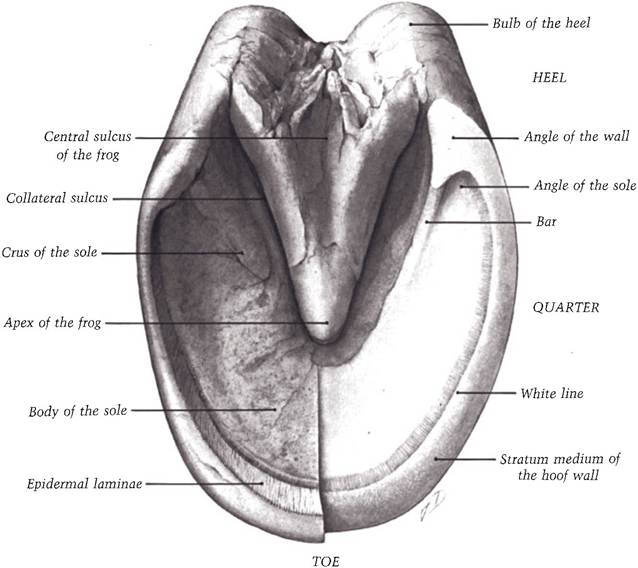
Figure 14-6. Gross anatomy of the ground surface of the equine hoof. The right side of this hoof is shown freshly trimmed. (Reprinted with permission of Wiley-Blackwell from Stashak T.S. Adams’ Lameness in Horses. 5th ed. Baltimore: Lippincott Williams & Wilkins, 2002.)
several muscles in the thoracic and pelvic limbs continue into the foot, where each tendon inserts on one or more phalanges, as described in Chapter 7 (see Figs.
7-8 and 7-10).The common digital extensor tendon passes down the dorsal aspect of the metacarpus, over the fetlock, and inserts on the extensor process of the distal phalanx. The long digital extensor tendon has the same course and insertion in the pelvic limb.
in the thoracic limb, the lateral digital extensor tendon inserts on the proximal end of the proximal phalanx after pursuing a course lateral to the common digital extensor tendon. in the pelvic limb, the lateral digital extensor tendon merges with the tendon of the long digital extensor muscle and inserts on the extensor process of the distal phalanx.
The tendon of the deep digital flexor muscle (in both thoracic and pelvic limbs) passes down the palmar/plantar side of the cannon bone and crosses the fetlock; it inserts on the palmar/ plantar portion of the distal phalanx. in this path, it passes superficial to the proximal and distal sesamoid bones.
The superficial digital flexor tendon passes distad on the cannon bone just superficial to the deep digital flexor tendon with which it shares a synovial sheath. Distal to the fetlock the superficial digital flexor tendon divides into two branches, which pass on each side of the deep digital flexor tendon and insert at the proximal end of the middle phalanx and the distal end of the proximal phalanx.
Strain of the flexor tendons can result in tendonitis (more correctly called tenosynovitis to acknowledge the role of inflammation of synovial structures). The inflammation produces a convex profile to the normally straight tendons. This bowed tendon is most
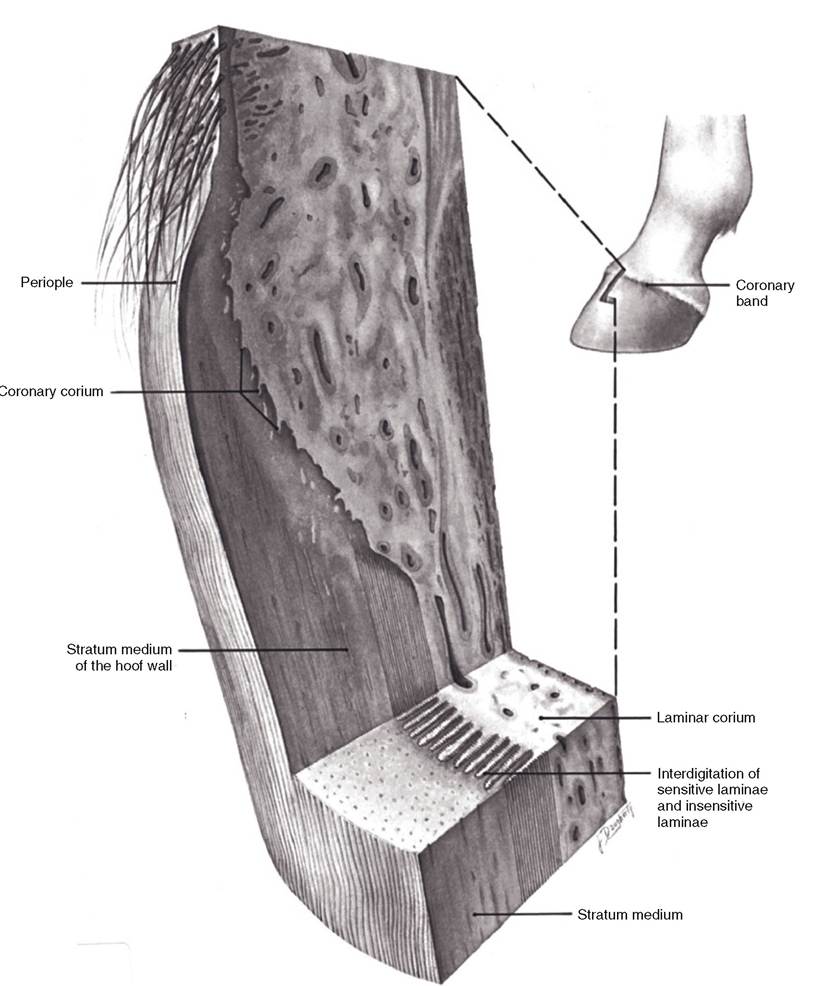
Figure 14-7. Relationship between the corium of the coronary region (coronet) and the hoof wall. Insert) The gross location of this section. Note the cross-sectional appearance of the laminae. (Reprinted with permission of Wiley-Blackwell from Stashak T.S. Adams’ Lameness in Horses. 5th ed.
Baltimore: Lippincott Williams & Wilkins, 2002.)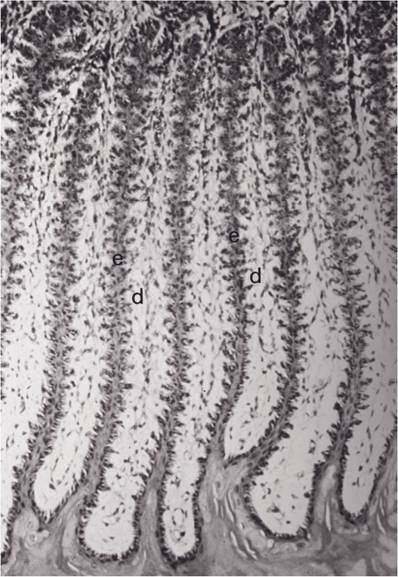
Figure 14-8. Photomicrograph of a cross-section of equine fetal hoof in the region of the laminae. e, Epidermal laminae; d, interdigitate with dermal laminae. (Reprinted with permission of Wiley-Blackwell from Stashak T.S. Adams’ Lameness in Horses. 5th ed. Baltimore: Lippincott Williams & Wilkins, 2002.)
commonly seen in horses used at speed (e.g., racehorses; see also Fig. 7-9).
Ligaments
The ligaments of the foot include the medial and lateral collateral ligaments of fetlock, pastern, and coffin joints. These are typical collateral ligaments as found in any ginglymus joint. In addition, a specialized structure, the suspensory ligament, runs parallel to the cannon bone on its palmar/plantar aspect. In animals with more than one digit, this structure usually has a considerable amount of muscle; in such animals, it lies between adjacent meta- carpals or metatarsals and is therefore called the interosseous muscle. The suspensory ligament of foals often has significant muscle tissue that is subsequently replaced with connective tissue during maturation.
The equine suspensory ligament is found between the cannon bone and the deep digital flexor tendon. It attaches proximally to the proximal end of the cannon bone and to the distal row of carpal or tarsal bones. It passes down between the splint bones on the palmar/plantar surface of the cannon bone in the horse (Fig. 14-10).
upon reaching the fetlock, the suspensory ligament divides into several branches. The main continuation of the suspensory ligament attaches to the proximal sesamoid bones and to the ligaments that bind these two bones together. In addition, medial and lateral bands (extensor slips or extensor branches) extend to the dorsal side of the fetlock to attach to the tendon of the common digital extensor muscle. The suspensory ligament acts as a strong supportive mechanism for the fetlock, discussed later with the stay apparatus.
The proximal sesamoid bones form a critical physical connection between the suspensory ligament and three sets of sesamoidean ligaments that connect the proximal sesamoid bones with the middle and proximal phalanges. Taken together, this set of structures provides a relatively inelastic band that supports the fetlock (discussed later in the section on the stay apparatus). The proximal sesamoids are also linked together by a broad ligament, the palmar (plantar) ligament. This ligament forms a smooth depression between the sesamoid bones, covered by synovial membrane for frictionless movement of overlying flexor tendons. The proximal sesamoids are further stabilized by medial and lateral collateral sesamoidean ligaments to the distal end of the cannon bone and proximal end of the proximal phalanx and by two short sesamoidean ligaments attaching them to the proximal phalanx.
The sesamoidean ligaments that connect the proximal sesamoids to more distal structures include, from superficial to deep, a straight sesamoidean ligament, two oblique sesamoid- ean ligaments, and a pair of cruciate sesamoid- ean ligaments (Fig 14-11). Their names describe
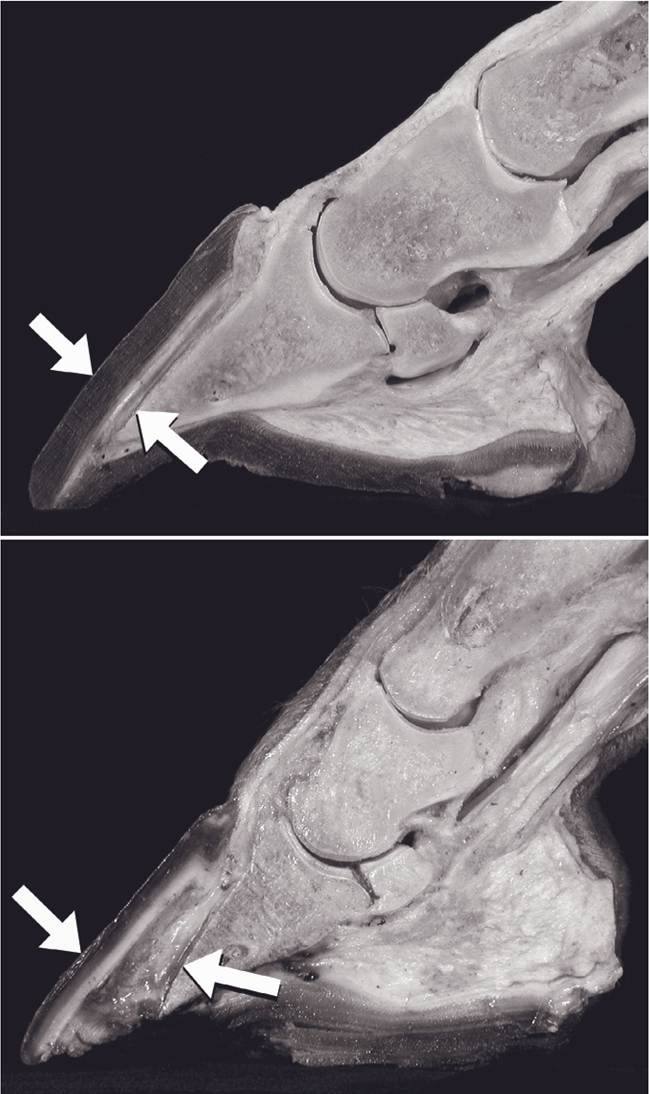
Figure 14-9. Chronic Iaminitis (founder) is characterized by loss of congruity between epidermal and dermal laminae. The distal phalanx is rotated away from the hoof wall by the distractive force of the deep digital flexor tendon. Top) Normal hoof in sagittal section. Arrows emphasize the parallel surfaces of the hoof wall and distal phalanx. Bottom) Hoof with chronic laminitis and rotation of the distal phalanx. (Photo supplied by A. Fails. Colorado State University, Fort Collins, CO)
Figure 14-10. Palmar view of the equine foot, illustrating the elements of the suspensory ligament and proximal sesamoids. The suspensory ligament and the ligaments of the proximal sesamoids form a continuous ligamentous band that passes from the carpus and proximal metacarpus to the proximal and middle phalanges. This part of the stay apparatus is the most important support for the fetlock joint.
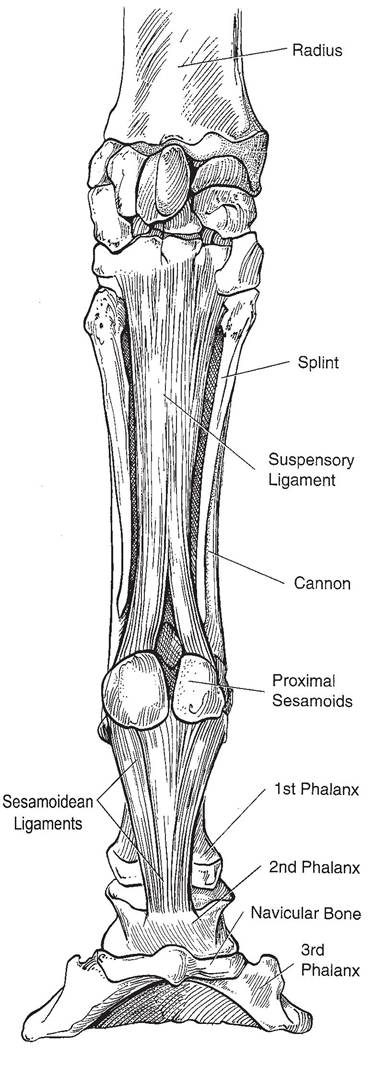
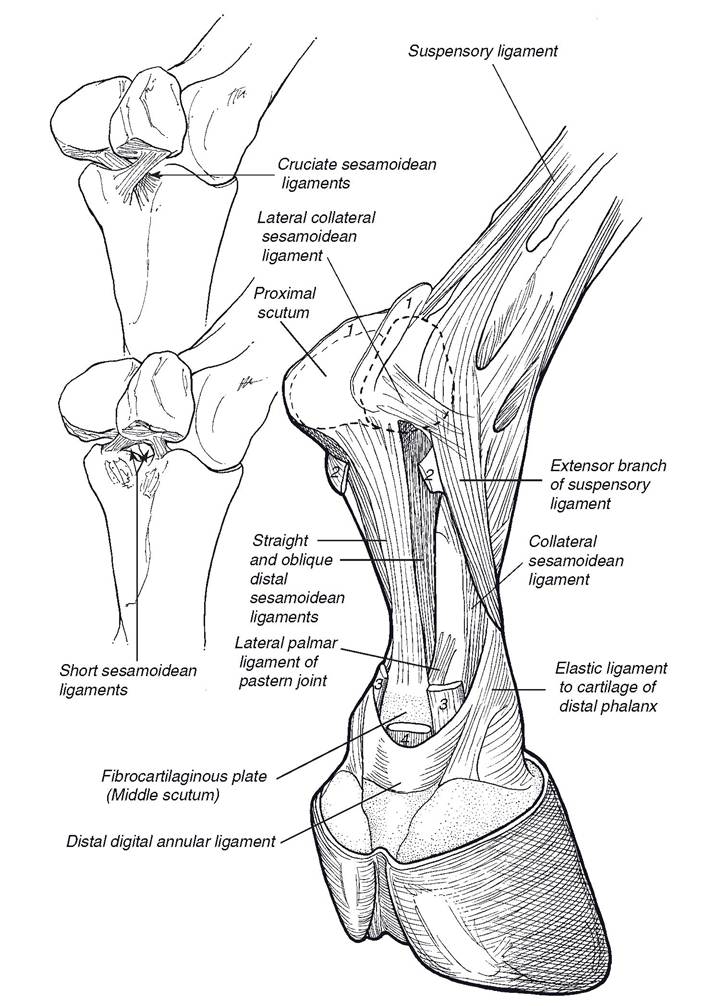
Figure 14-11. Sesamoidean ligaments. Broken lines indicate the positions of the proximal sesamoid bones. Numbers indicate the cut stumps of the (1) palmar annular ligament of the fetlock, (2) proximal digital annular ligament, (3) superficial digital flexor tendon, and (4) deep digital flexor tendon. (Reprinted with permission of Wiley-Blackwell from Stashak T.S. Adams’ Lameness in Horses. 5th ed. Baltimore: Lippincott Williams & Wilkins, 2002.)
their gross appearance; the straight ligament attaches to the middle phalanx, and the others to the proximal phalanx. As a group, these ligaments are often called the distal sesamoidean ligaments, but as this name sounds as though they are associated with the distal sesamoid (navicular) bone, it is probably best avoided.
The distal sesamoid bone (navicular bone) has a number of ligaments associated with it. Medial and lateral collateral ligaments attach the navicular to the distal phalanx, and an additional unpaired ligament (impar ligament) extends from the distal sesamoid to the solar surface of the distal phalanx. The proximal face of the navicular bone is connected to the middle phalanx and the deep digital flexor tendon by the T ligament (Fig. 14-2).
The many ligaments and tendons of the equine digit are bound together with a number of encircling annular ligaments. These are reasonably discrete thickenings of the local deep fascia. The palmar/plantar annular ligament arises from the proximal sesamoids and wraps around the palmar/plantar aspect of the fetlock, where its collagenous fibers blend with the flexor tendon sheath. The proximal digital annular ligament is more distal, forming a supportive sleeve on the palmar/plantar aspect of the pastern. Finally, the distal digital annular ligament forms a sling around the deep digital flexor tendon near the insertion of the superficial digital flexor tendon, holding the deep digital flexor tendon close to the pastern (Fig. 14-11).
Synovial Structures
The tendons of the superficial and deep digital flexor muscles share a synovial sheath that has its most proximal extent some 5 to 8 cm above the fetlock and that extends distad to the middle of the middle phalanx. The navicular bursa lies between the navicular bone and the deep digital flexor tendon. inflammation of this bursa is one component of navicular disease.
Navicular disease is a common cause of forelimb lameness in Quarter Horses and Thoroughbreds. A variety of pathologies are described with navicular disease, and not every affected horse shows all of them. These include erosion of the articular cartilages of the navicular bone, bursitis of the navicular bursa, adhesions between the deep digital flexor tendon and navicular bone, and erosions or necrosis of the navicular bone. There is a hereditary component to the disease, probably related to a certain conformational type, often described as a heavy horse on small feet with upright pasterns, which exposes the navicular bone and associated structures to excessive concus- sive forces. Improper trimming of the hoof, so that the toe is left too long and/or heels overshortened, increases the stress on the deep digital flexor tendon and may aggravate a predisposition to navicular disease.
The structure of the synovial joints between the phalanges and between the cannon and proximal phalanx is typical (see Chapter 6). The joint cavity of the fetlock is especially voluminous to accommodate the wide range of motion in this ginglymus joint. part of the joint cavity extends proximad between the cannon bone and suspensory ligament. Accumulation of excess synovial fluid within this palmar (plantar) recess may be associated with the trauma of hard training. This produces a visible distension of the recess called wind puffs or wind galls.