» Superficial Structures
Other organs that are visible or palpable in life may be identified with the assistance of Fig. 25.2. Relatively little of the skull lies directly below the skin, but large areas have thin coverings of fascia and cutaneous muscle, making it easy to palpate the broad forehead, dorsum of the nose, temporal line, zygomatic arch, facial tuberosity, nasoincisive notch, and ventral border.
The supraorbital, infraorbital, and mental foramina can also be identified (Figs. 25.1, 25.2, and 25.7).Few specific features of the mimetic musculature are important. It is supplied by the facial nerve (VII), which divides into its principal terminal branches under cover of the parotid gland. The auriculopalpebral nerve supplies muscles of the external ear and eyelids. It reaches these by crossing the zygomatic arch directly in front of the temporomandibular joint, where its superficial position makes it vulnerable (Fig. 25.6/3). Damage to the nerve may be evidenced by drooping of the ear and sagging of the eyelids, particularly the lower one. Paralysis of the orbicularis makes it impossible to close the eye. It is therefore clear that it may be advantageous to block the nerve to eliminate the blink reflex when examining the eye. It is most easily palpated where it passes over the zygomatic arch.
The dorsal buccal branch continues the parent trunk, crossing the masseter muscle in an exposed position that carries considerable risk of injury. The effects of such injury include loss of innervation to the muscles of the nose and upper lip and to the buccinator. The first loss leads to slight distortion of the face, which is drawn toward the unaffected side; the second allows food to collect in a wad within the oral vestibule. The ventral buccal branch takes a more protected course caudomedial to the ramus of the mandible and reaches the face in company with the facial artery and vein.
It has a limited distribution, and the visible effects of injury are minimal (Fig. 25.2/5 and 6).The distribution of the cutaneous nerves is shown in Fig. 25.8. Specific "blocks" of certain of these nerves are occasionally attempted. The large infraorbital nerve can be palpated where it leaves the infraorbital foramen, about 3 cm dorsal to the first cheek tooth. The mental nerve is found where it leaves the mental foramen of the mandible, about 3 to 4 cm caudal to the lateral incisor tooth (Table 25.1).
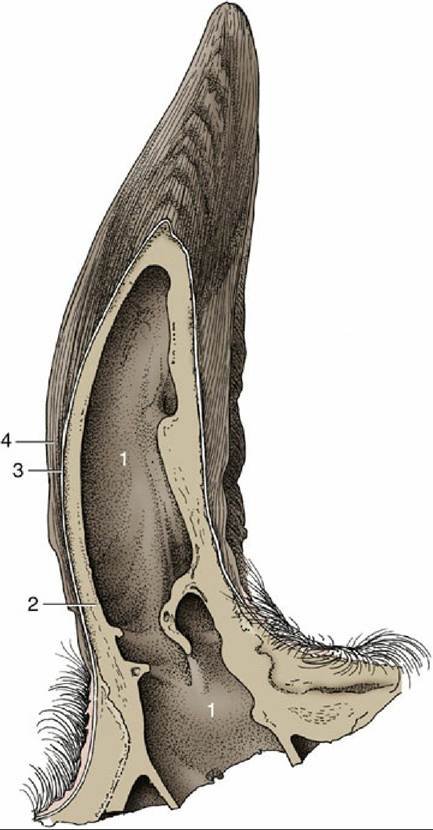
FIG. 25.4 Longitudinal section of a bovine horn. 1, Cornual diverticulum of frontal sinus; 2, cornual process; 3, periosteum, dermis, and epidermis; 4, horn tubules.
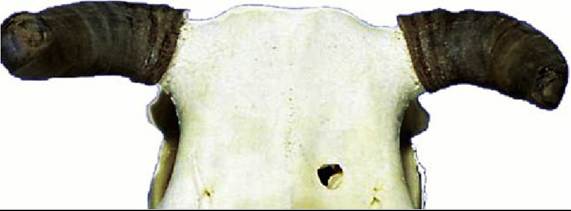
FIG. 25.5 Horn rings resulting from variation in horn production and wear in cattle.
The facial artery and vein are the most important superficial vessels. They cross the ventral margin of the mandible in front of the masseter muscle and are distributed to the lips, cheeks, muzzle, and periocular structures. The pulse may be examined where the artery lies on the side of the bone; it is less easily located in the notch of the ventral border.
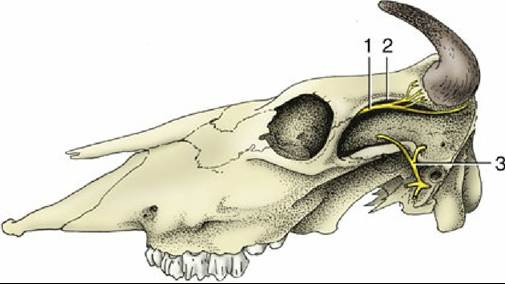
FIG. 25.6 Cornual nerve (1) follows the temporal line (2) on bovine skull. The auriculopalpebral nerve (3) is palpable where it crosses the zygomatic arch.
The position of the frontal vein should also be noted because this fair-sized vessel is at some risk in trephination of the caudal frontal sinus. The vein takes a caudorostral course in a palpable groove over the frontal bone to enter the supraorbital foramen; it then traverses a canal in the lateral part of the sinus. The foramen is located about 2 cm medial to the temporal line and about 2 cm caudal to the lateral angle of the eye (see Fig.
25.12/4). A system of veins on the external surface of the pinna becomes engorged and prominent when a tourniquet is applied around the base of the ear. The central member of the set is sometimes used as an alternative to the jugular vein for the placement of an indwelling catheter. Neither site is free from problems.The ventral end of the mandibular gland forms a conspicuous swelling in the intermandibular space. When palpated, this gland is often mistaken for the adjacent mandibular lymph node (Fig. 25.2/20) but is identified based on its larger size, softer consistency, and more medial and more rostral extent. The lymph node can be separately identified on the medial aspect of the sternomandibularis tendon. Normally the parotid lymph node is also palpable rostroventral to the temporomandibular joint.
In the last part of its course along the rostral margin of the masseter, the parotid duct accompanies the facial vessels and ventral buccal nerve. The duct penetrates the cheek opposite the fifth upper cheek tooth.