The Hindgut
The hindgut develops into the descending colon and the rectum, parts supplied by the caudal mesenteric artery in the adult. Initially the gut ends blindly against the cloacal plate.
Except in the horse and ruminants, in which the descending colon shows a secondary increase in length, significant changes affect only the terminal part of the hindgut. A bud, the allantois, grows from its ventral aspect toward and through the umbilical opening in the abdominal wall; once outside the embryo it enlarges to form the capacious allantoic sac (see Fig. 5.66). A wedge of tissue (urorectal septum) enlarging in the angle between the gut and this diverticulum thrusts toward the cloacal membrane (Fig. 3.66). When it meets the membrane, the wedge divides the gut into two separate tubes: the dorsal one is continuous with the descending colon, and the ventral one is continuous with the allantois and destined to form the lower urogenital tract. Meanwhile, proliferation of mesoderm beneath the ectoderm around the proctodeum has deepened the pit, which is added to the gut upon breakdown of the dorsal part (anal membrane) of the cloacal membrane. The result is the anal canal leading to the exterior.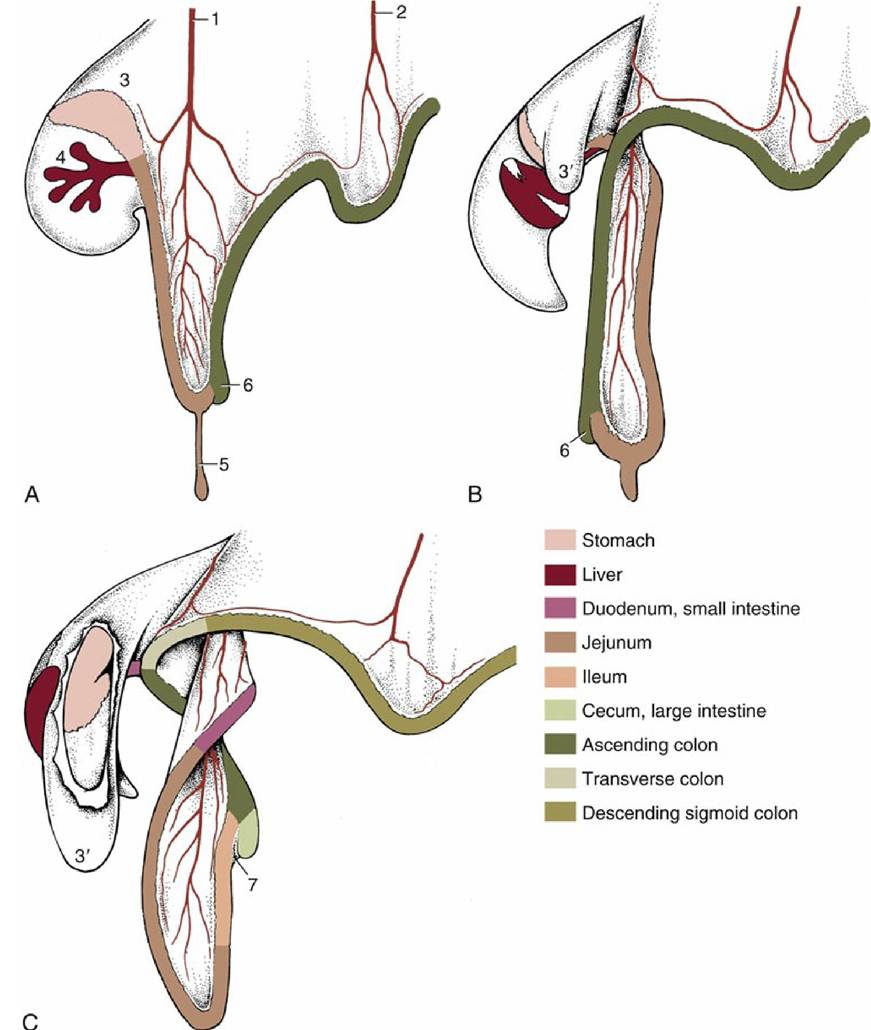
FIG. 3.64 (A to C) Three stages in the growth and rotation of the canine midgut, in left lateral views. 1, Cranial mesenteric artery; 2, caudal mesenteric artery; 3, dorsal mesogastrium; 3', greater omentum, fenestrated in (C) to expose stomach; 4, ventral mesogastrium with developing liver; 5, vitelline duct; 6, cecal primordium; 7, ileocecal fold.
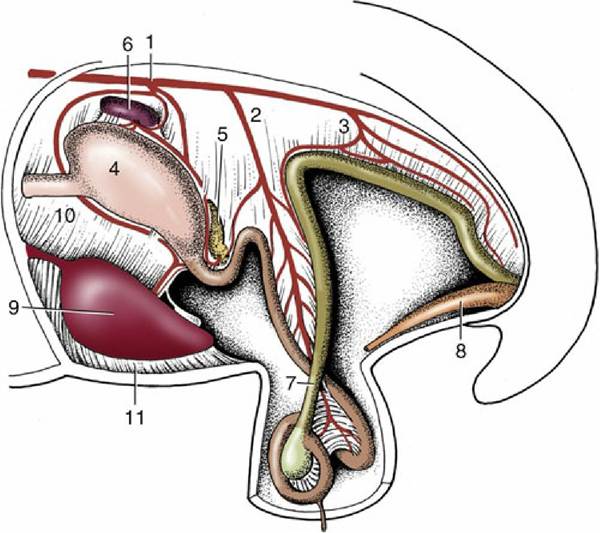
FIG. 3.65 Development of the intestinal tract during the rotation process. The midgut loop is herniated into the extraembryonic celom.
1, Celiac artery; 2, cranial mesenteric artery; 3, caudal mesenteric artery; 4, stomach; 5, pancreas; 6, spleen; 7, loop of midgut; 8, bladder expansion of the urogenital sinus; 9, liver; 10, lesser omentum; 11, falciform ligament.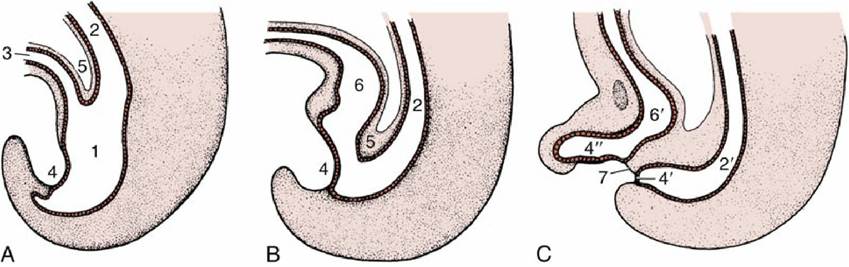
FIG. 3.66 Division of the distal part of the hindgut into the rectum and urogenital sinus. (A) Formation of the allantois and beginning of the caudal extension of the urorectal septum (5). (B) The urorectal septum now approaches the cloacal membrane. (C) Complete division of the urogenital sinus and anorectal canal.
1, Cloaca; 2, hindgut; 2', anorectal canal; 3, allantois; 4, cloacal membrane; 4', anal membrane; 4", urogenital membrane; 5, urorectal septum; 6, primitive urogenital sinus; 6', urogenital sinus; 7, tissue bridge ventral to future anus.
Comprehension Check
Using an embryologic framework, discuss the in vivo arrangement of the digestive tract. Also, demonstrate an understanding of the projections of various digestive organs on the body surface.
>-------------------- <
* The digestive, respiratory, urinary, and male and female reproductive organs constitute a series of systems or apparatuses whose study collectively is known as splanchnology. Most of the component parts are known as viscera (plural of viscus, Latin for organ).
* Terms relating to the teeth—for example, dentin, periodontium, orthodontics, and so forth—are derived from the Latin (dens) or the Greek (odous).
* Most organs contained within the body cavities (divisions of the embryonic celom) are protected by “serous membranes” (serosae). These coverings, which extend to line the walls of the body cavities, consist of a layer of flat mesothelial cells supported by a delicate connective tissue. A small amount of watery (serous) fluid keeps the membranes moist and minimizes friction when opposing surfaces move against each other.
* The alternative term gaster, derived from the Greek, is the root of most clinical terms: for example, gastritis and gastrectomy.
* The Greek word enteron provides the stem for many terms: enteritis, mesentery, and so forth.
* These patches may be initial sites for the accumulation, after ingestion, of the infective agents responsible for the transmissible spongiform encephalopathies (“new variant” Creutzfeldt Jacob disease, bovine spongiform encephalopathy [BSE], scrapie) that have claimed so much attention in recent years.