The Lung Continuously Produces Lymph as a Result of the Net Fluid Movement from the Pulmonary Microvasculature into the Pulmonary Interstitium
In the lung, as in other organs, there is continual movement of water and solutes from the capillary bed into the lung interstitium. The hydrostatic and osmotic forces governing fluid movement are the same as those in other organs, but because the lung vasculature operates at low pressure, the magnitude of the forces is different.
About 60% of fluid filtration takes place from alveolar capillaries, 15% from extra-alveolar small arteries, and 20% from extra-alveolar veins.Figure 50-4 represents a capillary in the alveolar septum. Fluid filtration normally occurs between the capillary and the interstitial tissue on the thick side of the alveolar septum, where a layer of interstitium is interposed between the
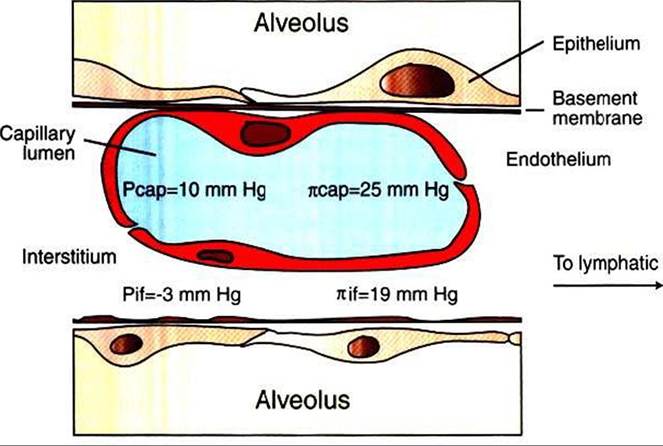
FIGURE 50-4 Diagrammatic representation of a capillary in the alveolar septum. Top, Capillary endothelium and alveolar epithelium share a basement membrane. Bottom, Endothelium and epithelium are separated by a layer of interstitial tissue. Values for capillary and interstitial fluid hydrostatic pressures (Pcap and Pif) and oncotic pressures (neap and πif) are shown.
endothelium and the epithelial basement membrane. On the thin side of the septum, interstitial tissue is absent because the capillary endothelium shares a basement membrane with the alveolar epithelium. Fluid movement out of the capillary is thought to occur between endothelial cells, but these gaps are too small to allow passage of macromolecules. The latter probably pass through endothelial cells in vesicles, which may fuse to form Iransendothelial channels. Another possibility is that these large molecules pass through gaps between cells that appear when the endothelia contract and become more permeable under the influence of mediators such as histamine.
The alveolar epithelium is less permeable than the capillary endothelium, and therefore fluid does not leak into the alveoli unless the epithelium is damaged or unless there is considerable fluid accumulation in the interstitium.Forces described in Starling’s equation govern the movement of fluid across the endothelium:

where Qfis the amount of fluid flowing per minute; Kfis the capillary filtration coefficient; Pcap is capillary hydrostatic pressure; Pif is interstitial fluid hydrostatic pressure; πcaρ and πif are capillary and interstitial colloid osmotic (oncotic) pressures, respectively; and σ is the colloid reflection coefficient (see Chapter 23). Figure 50-4 shows average values for vascular and interstitial pressures.
When values shown in Figure 50-4 are inserted into Starlings equation, the net force is positive and favors Iluid filtration from the capillaries to the interstitium of the lung. The fluid that is continuously filtered from capillaries moves through the interstitium toward the perivascular and peribronchial tissues, where lymphatic vessels are located. Fluid transport out of the lung along lymphatic vessels is aided by lymphatic vasomotion, valves, and the pumping action of the lungs during breathing.
The movement of fluid between the capillaries and the interstitium varies with changes in vascular permeability and with hydrostatic and oncotic pressures. Increases in capillary hydrostatic pressure occur during exercise and in animals with left-sided heart failure. These elevated pressures result in an increase in fluid filtration from the capillaries into the interstitium. The lymphatic vessels remove this filtered fluid and can accommodate large increases in fluid flux. Excess fluid accumulates around the bronchi and large blood vessels. The compliant peribronchial and perivascular spaces provide these intrapulmonary repositories for fluid accumulation.
Fluid does not accumulate in the alveoli and cause clinically evident pulmonary edema unless there is a large increase in the amount of fluid being filtered from the capillaries. Alveolar flooding occurs once the peribronchial capacity is exceeded. The fluid probably enters the air spaces across the alveolar epithelial cells or at the level of the bronchioles. The foaming fluid typical of clinical pulmonary edema results from the mixing of air, edema fluid, and surfactant within the airways.Increased fluid filtration and pulmonary edema can also result from a decrease in plasma oncotic pressure, which is a result of hypoproteinemia. Hypoproteinemia can be caused either by starvation or by the Overvigorous administration of intravenous fluids that dilute the plasma proteins. Increased vascular permeability occurs in many inflammatory lung diseases, such as pneumonia. This results from the effects of neutrophil products, probably oxygen radicals, on the endothelium. Protein-rich fluid leaks into the interstitium, elevating interstitial fluid oncotic pressure and causing osmotic attraction of water into the interstitium from the vasculature.