THE NERVES OF THE HINDLIMB
The formation and ramification of the lumbosacral plexus and the distribution of its peripheral branches follow the common pattern in broad outline; important
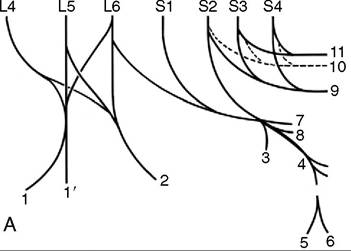
Figure 24-18 The nerves of the hindlimb.
A, The lumbosacral plexus, schematic. B, The principal nerves, medial view. 1, Femoral n.; 1', saphenous n.; 2, obturator n.; 3, cranial gluteal n.; 4, sciatic n.; 5, common peroneal n.; 5', lateral cutaneous sural n.; 5", 5,", superficial and deep peroneal nn.; 6, tibial n.; 6', caudal cutaneous sural n.; 6", 6'", medial and lateral plantar nn. (the lateral nerve gives rise to the plantar metatarsal nn.); 7, caudal gluteal n.; 8, caudal cutaneous femoral n.; 9, pudendal n.; 10, pelvic n.; 11, caudal rectal n.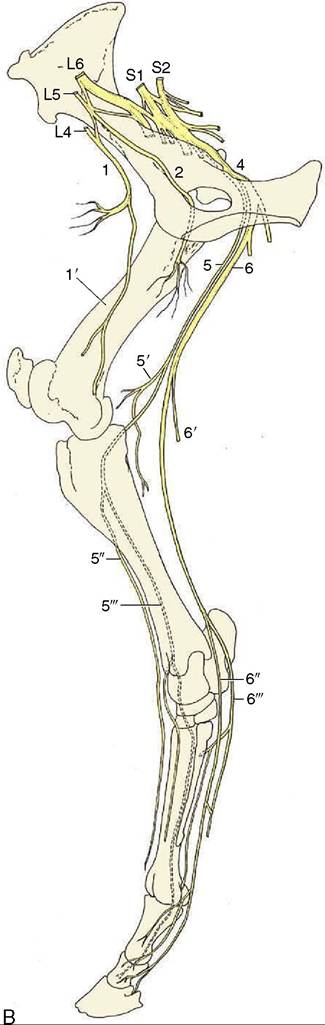
species differences are confined to the innervation of the foot.
The cranial and caudal gluteal nerves attend to the innervation of the lateral muscles of the croup, including the vertebral heads of the hamstring muscles; the details have been given.
The distributions of the femoral, obturator, and sciatic nerves have greater clinical relevance. The femoral nerve (L4-L6) (Figure 24—18/7) passes through and also supplies the sublumbar muscles before entering the thigh by way of the vascular lacuna. It then splits into several branches, most of which at once enter the quadriceps. The one branch of more extended course, the saphenous nerve (Figure 24—18/7'), continues within the femoral triangle before penetrating the medial femoral fascia to obtain a more superficial position. It continues through the thigh, leg, and upper cannon, supplying skin over the medial aspect of the limb from thigh to fetlock.
It also supplies the sartorius. Extensive damage to the femoral nerve is uncommon, but when it does occur, the consequences are severe; paralysis of the quadriceps removes the ability to fix the stifle and therefore the ability to support weight on the affected limb. In addition, skin sensibility is lost over a considerable area.The obturator nerve (L4-L6) (Figure 24-18/2) leaves the pelvis by way of the obturator foramen and innervates the adductor muscles (pectineus, gracilis, adductor, and obturator externus). Injury, which generally follows foaling or a pelvic fracture, results in partial or complete inability to adduct the limb. The severity of the dysfunction is rather unpredictable; it appears to depend on the weight of the animal, the nature of the terrain, and the extent of the lesion.
The sciatic nerve (L6-S2) (Figure 24-18∕√) leaves the pelvis by the greater sciatic foramen and after a short course over the sacrosciatic ligament turns distally caudal to the hip joint to enter the thigh under cover of the biceps. It divides about the level of the joint into tibial and peroneal nerves that initially run together. They part company a little above the stifle, when the peroneal nerve moves laterally to pass between the biceps and the lateral head of the gastrocnemius; the tibial nerve holds its course and runs between the two heads of the gastrocnemius. Both divisions detach cutaneous branches while still within the thigh. That from the peroneal (lateral cutaneous sural nerve; Figure 24-18∕5') becomes subcutaneous by piercing the biceps and then spreads to supply skin over the lateral aspect of the leg. The corresponding tibial branch (caudal cutaneous sural nerve; Figure 24-18∕d') descends in the fascial plate between the calcanean tendon and deep flexor, following the lateral saphenous vein for part of its course. It supplies branches to the skin over the plantarolateral aspect of the hock and cannon, reaching to the fetlock.
The peroneal nerve divides caudal to the lateral collateral ligament of the stifle into deep and superficial branches.
The superficial branch (Figure 24-18/5") continues down the leg, slightly sunken within the groove between the long and lateral extensors, where it can be palpated below the middle of the leg. It supplies the lateral extensor, the skin over the lateral aspect of the leg, and more distal segments of the limb. The deep branch takes a parallel course after sinking deeply between the same two muscles to follow the cranial face of the intervening septum (Figure 24-18Z5'" and Figure 24-7Z6'). It supplies branches to the remaining muscles of the dorsolateral group and then continues under cover of the long extensor tendon as a purely sensory nerve that splits into medial and lateral branches over the hock. These, the medial and lateral dorsal metatarsal nerves, edge toward the grooves between the cannon and splint bones (Figure 24-19Z5,5'). The lateral nerve follows the palpable dorsal metatarsal artery (Figure 24-20Zwhere it is easily palpated (Figure 24-7Z12). When level with the calcaneus, it divides into medial and lateral plantar nerves that pass over the sustentaculum tali beside the deep flexor tendon. The lateral nerve diverges laterally, and just distal to the hock, it detaches the common trunk of the medial and lateral plantar metatarsal nerves (Figure 24-19Z2'). These supply the interosseous muscle and associated structures and the plantar pouch of the fetlock joint (Figure 24-19Z√,√'). The medial plantar nerve follows the line of the parent trunk. Although the plantar nerves generally resemble the palmar nerves of the forelimb, the communicating branch is relatively slight or even absent; when present, it can usually be palpated as it slopes in a laterodistal direction over the superficial aspect of the flexor tendons (Figure 24-19Z1).There is one other difference. The dorsal and plantar metatarsal nerves play a larger role in the sensory innervation of the hoof contents than do the corresponding forelimb trunks—the dorsal branch of the ulnar nerve and the palmar metacarpal nerves—which commonly fail to reach the coronet.
Tibial paralysis is manifested by a slight sagging of the hock when weight is borne on the affected limb. Despite the inability to flex the distal joints, the gait is not seriously disturbed. The sensory deficit is very considerable.
Lesions that affect the sciatic trunk involve the hamstring as well as the leg muscles. Despite this, the consequences are less disastrous than might well be supposed. Retention of activity by the quadriceps enables the animal to fix the stifle and, through the reciprocal apparatus, the hock. It is thus able to support weight on the limb. Cutaneous and deep sensations are lost below the stifle, except in the province of the saphenous nerve.
The tibial nerve may be blocked on the lateral side of the limb approximately 10 cm above the point of the hock.

Both superficial and deep branches of the peroneal nerve can be blocked by injecting, subcutaneously and then deeply from the same point of entry, between the long and lateral extensors a handbreadth or so proximal to the tarsocrural joint (Figure 24-7Z6,6'). Apart from this, the local anesthetic techniques for surgical and diagnostic purposes generally resemble those prescribed for the forelimb; the one distinction of relevance is the distal extension of the dorsal metatarsal nerves. It is possible to block the undivided tibial nerve (level with the point of the hock) as an alternative to the plantar nerves (Figure 24-7Z12).