The Paranasal Sinuses
The extensive sinus system possesses considerable clinical interest because it is susceptible to infection that may spread from the nose or from an alveolar abscess. It also provides a means of access to the unerupted portions of the caudal cheek teeth (Fig.
18.13).» TABLE 18.1
Superficial Nerves of the Face of the Horse
Nerve Areas Supplied
| Facial | Auriculopalpebral branch | Muscles of eyelid and external ear |
| Dorsal and ventral buccal branch | Muscles of lip, cheek, and nose | |
| Trigeminal | Supraorbital nerve | Upper eyelid and the adjacent skin on forehead |
| Infraorbital nerve | Skin of the upper lip, nostril, and nose extending caudal to the foramen | |
| Mental nerve | Skin of the lower lip and chin |
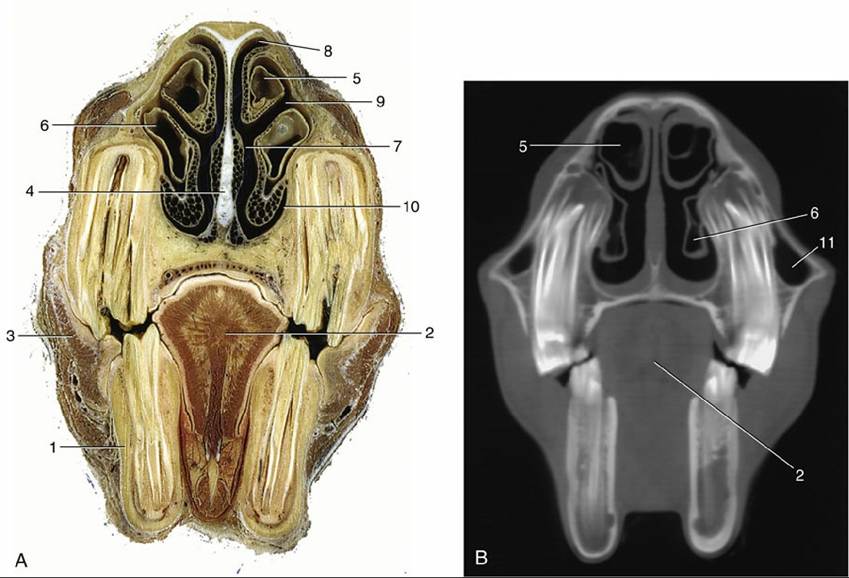
FIG. 18.10 (A) Transverse section of the head at the level of the rostral maxillary sinus. (B) Computed tomographic scan (bone window) at about the same level. 1, P4; 2, tongue; 3, buccinator; 4, nasal septum; 5, dorsal nasal concha; 6, ventral nasal concha; 7, common nasal meatus; 8, dorsal nasal meatus; 9, middle nasal meatus; 10, ventral nasal meatus; 11, rostral maxillary sinus.
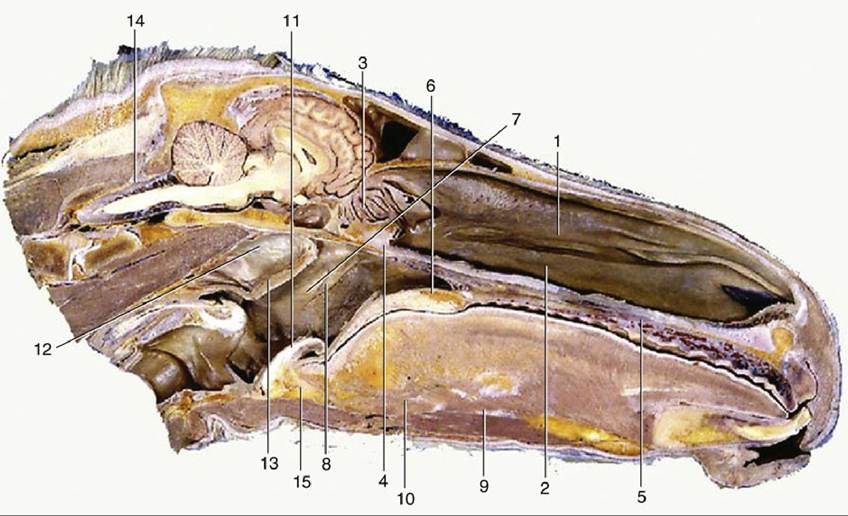
FIG. 18.11 Median section of the head; most of the nasal septum has been removed. 1, Dorsal nasal concha; 2, ventral nasal concha; 3, ethmoidal conchae; 4, right choana; 5, hard palate with prominent ridges (rugae); 6, soft palate; 7, nasopharynx; 8, pharyngeal opening of auditory tube; 9, geniohyoideus;
10, genioglossus; 11, epiglottis; 12, medial wall of guttural pouch; 13, pharyngeal muscles; 14, cerebellomedullary cistern; 15, basihyoid.
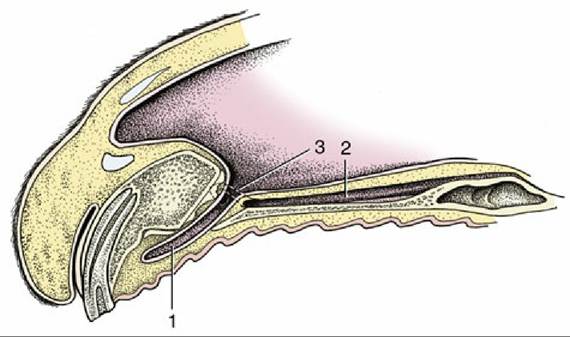
FIG. 18.12 Paramedian section of the rostral end of the nose. 1, Incisive duct; 2, vomeronasal organ; 3, opening of the incisive duct into the nasal cavity and opening of the vomeronasal organ into the incisive duct.
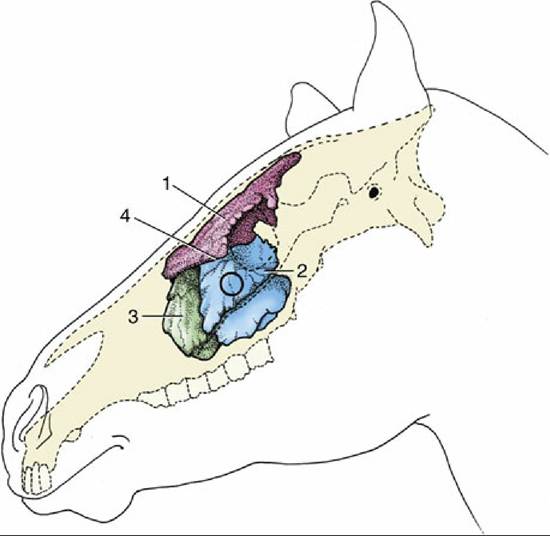
FIG. 18.13 Topography of the conchofrontal and maxillary sinuses, which are filled with casting material. The circle indicates where the caudal maxillary sinus can be trephined. 1, Conchofrontal sinus; 2, caudal maxillary sinus; 3, rostral maxillary sinus; 4, position of frontomaxillary opening between 1 and 2.
On each side there are frontal, caudal maxillary, and rostral maxillary sinuses of importance and sphenopalatine and ethmoidal spaces of less account. The layout is complicated and, in one important respect, unique (among domestic species): the frontal sinus communicates with the nasal cavity indirectly via the caudal maxillary sinus.
The frontal sinus occupies the dorsal part of the skull medial to the orbit. It overlaps both cranial and nasal cavities, and because it also occupies the closed part of the dorsal concha, it is more correctly known as the conchofrontal sinus. Its extent is shown in Fig. 18.14/1 and 1'. From this it will be seen that the interior of the frontal part is incompletely divided by several bony lamellae. The floor of this part is molded over the ethmoidal labyrinth, and rostrolateral to these areas of unevenness, it displays the large oval communication (frontomaxillary opening) with the caudal maxillary sinus. The opening normally allows easy natural drainage.
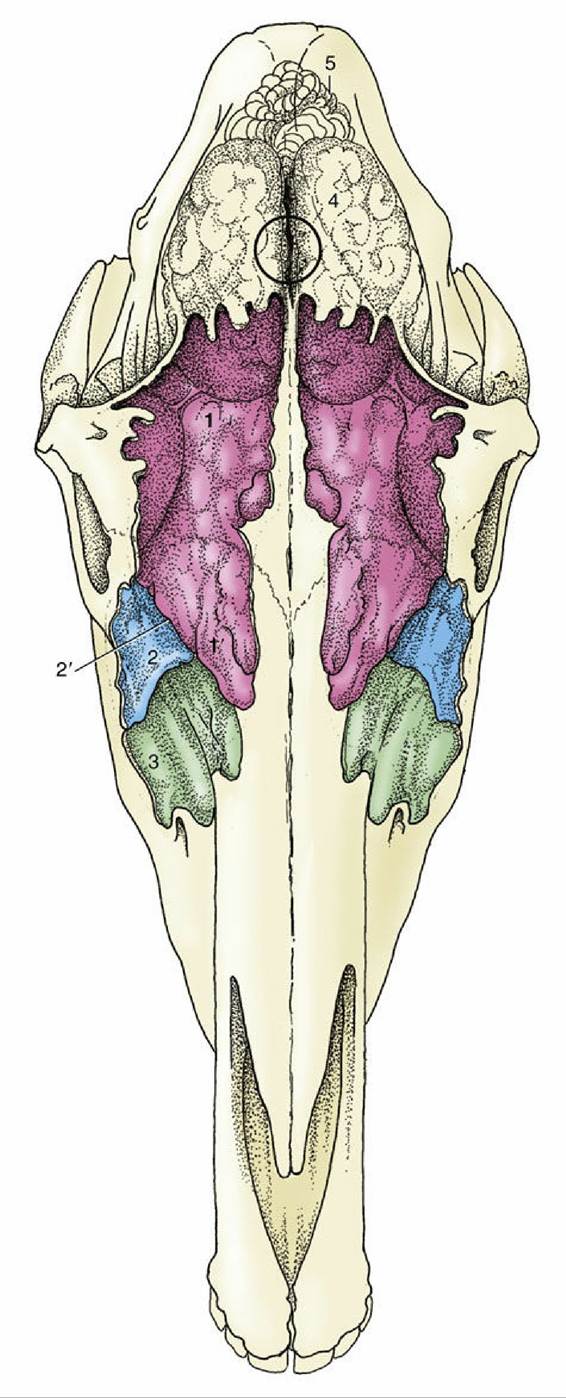
FIG. 18.14 Projection of the brain and frontal and maxillary sinuses on the dorsal surface of the skull. The sinuses are filled with casting material. The frontal sinus extends caudally over the rostral part of the brain and rostrally beyond the level of the orbit.
The circle indicates the center of the brain and the location where a horse may be shot. 1 and 1', Conchofrontal sinus: frontal part (1) and dorsal conchal part (1); 2, caudal maxillary sinus; 2', position of frontomaxillary opening; 3, rostral maxillary sinus; 4, cerebrum; 5, cerebellum.Trephining: A window may be opened, usually by trephination, in the roof of the frontal sinus to allow for irrigation or for removal of a molar by repulsion, when a punch introduced through the frontomaxillary opening is brought to bear on the appropriate alveolus. Such a window also allows introduction of a fiberoptic endoscope to inspect the interior of this large sinus.
The two maxillary sinuses together occupy a large part of the upper jaw, where they have a critically important relationship to the embedded portions of the caudal cheek teeth. They share a slitlike communication (nasomaxillary opening) with the middle meatus of the nasal cavity but are otherwise completely divided by an oblique septum. This is variable in position but most commonly located about 5 cm caudal to the rostral end of the facial crest. The ventral part of each sinus is also divided into medial and lateral spaces by an upright longitudinal plate supporting the infraorbital canal and fused in young animals to the alveoli containing the roots and unerupted portions of the cheek teeth. The medial part of the caudal sinus continues into the irregular sphenopalatine sinus. The corresponding part of the rostral sinus extends into the ventral concha.
It is impossible to define the exact extent and projections of the maxillary sinuses, which enlarge considerably after birth as the teeth are extruded (Fig. 18.15). Their relationship to the teeth is also affected by the forward migration of the teeth as they develop and come into wear. As Fig. 18.15 shows, the relationship is confined to the last premolar and first molar tooth in the newborn foal; it later extends to involve the last four teeth but finally retains contact only with the three molars.
There is much variation, and attention to the varying inclination of the embedded parts of different teeth is required.Entering the Maxillary Sinus: Entry to the sinus may be required either to effect drainage (because the natural route, the nasomaxillary opening, is placed high in the wall) or to give access to certain teeth. Although factors such as the routes followed by the very vulnerable nasolacrimal duct and infraorbital nerve limit the safe surgical area of maxillary sinuses, the potential operating area is defined by the following boundaries: (1) the vertical line tangential to the rostral limit of the orbit; (2) the facial crest; (3) the oblique line joining the rostral limit of the crest to the infraorbital foramen; and (4) the line parallel to the facial crest that intersects the infraorbital foramen.
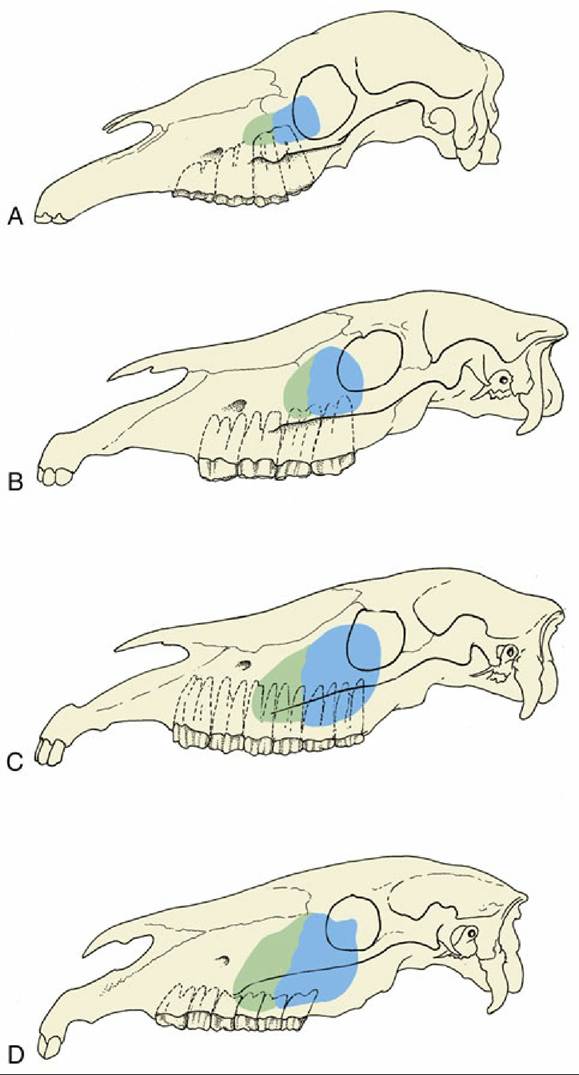
FIG. 18.15 Projection of the maxillary sinuses at various ages. In older horses the cheek teeth are more rostrally placed. (A) 1 month. (B) 1 year. (C) 4 to 6 years. (D) Older than 12 years.
» The Mouth
The small size of the entrance makes it impossible to open the mouth wide; this limitation, coupled with the great depth of the cavity, severely hampers clinical inspection.
The vestibule communicates with the mouth cavity proper only between the incisor and cheek teeth (where the diastema may be interrupted by the canine teeth) and by small gaps behind the last molars. The hard palate is therefore largely bounded by the alveolar processes and teeth. It is almost uniformly broad and is marked by two more or less symmetrical series of ridges (Fig. 18.11/5). The incisive papilla is found directly behind the central incisors; grooves that flank the elevation end blindly and do not communicate with the nasal cavity and vomeronasal organs (Fig. 18.12). The mucosa of the hard palate is thick, particularly in its most rostral part, and incorporates a very generous venous plexus, which may become engorged (lampas) at the time of tooth replacement when it may project above the occlusal surfaces of the neighboring teeth.
The appearance is striking, and laypeople are sometimes alarmed by this purely physiologic phenomenon.The soft palate continues the hard palate beyond the level of the second molar tooth. It is remarkably long and hangs down before the epiglottis; its free margin is closely applied to the tongue. The palatopharyngeal arches extend caudally from the palate, completing a sphincter about the structures that bound the entrance to the larynx, which thus projects some way into the nasopharynx. The application of the palate to the tongue is so firm that an airtight seal is created that closes the oropharynx, which then provides a barrier between the mouth and the pharynx. This ensures that breathing is through the nose, precluding use of the oral route and incidentally resulting in ingesta passing into the nasal passages on the rare occasions when horses vomit. These relationships of the palate are normally maintained except during deglutition.
The obstructions of the upper respiratory tract commonly recognized in horses worked at a fast pace are often due to anomalous position and relations of the soft palate and lead to diminished physical performance. There obstructions are more common at the palatopharyngeal level in younger animals and at the laryngeal level in older animals, and frequently both occur together.
The use of videoendoscopy of the nasopharynx and larynx of affected horses while they were strenuously exercised on a treadmill has helped to identify two abnormal conditions of the soft palate. These apparently occur after admission of air into the oropharynx breaks the seal that normally maintains the parts in close apposition. In the less severe form, there is abnormal movement of the caudal part of the palate, aptly described as "billowing." In the more severe form, of which billowing is probably a precursor, the soft palate is displaced dorsally, losing contact with the ventral side of the epiglottis and narrowing the nasopharyngeal airway.
At endoscopy the epiglottis is no longer visible. Both forms may be accompanied by abnormal respiration sounds.Some of the factors that may break the seal include the following: the extreme negative pressure developed in the rostral nasopharynx at one stage of the respiratory cycle; dysfunction of the palate musculature weakening the contact between tongue and palate; overactivity of those ventral cervical muscles that attach to the larynx and hyoid, drawing the larynx caudally and freeing the palate from entrapment by the epiglottis; and abnormal activity of the hyoepiglottic muscle, tilting the epiglottis caudally with the same effect.
The mucosa on the oral surface of the soft palate is marked by numerous pits where the palatine glands open. It also exhibits a rostral median tonsillar swelling.
The tongue is long, conforming to the shape of the cavity, and is spatulate at its apex, which is incompletely restrained by a narrow frenulum. Its upper surface is thickly strewn with delicate filiform papillae that confer a velvet-like texture; the larger papillae with gustatory function are less widely spread (Fig. 18.16/9-H). A scattering of lymphoid tissue over the root constitutes a diffuse lingual tonsil. Each of two low mucosal folds beneath the apex of the tongue carries a fleshy sublingual caruncle where the mandibular duct opens.
» The Dentition and Masticatory Apparatus
The Dentition
The dentition of the horse is admirably suited to a diet of grass, a surprisingly abrasive material. The masticatory area is increased by the enlargement of the premolars and their assimilation to the molars, with which they present a continuous grinding surface. Both cheek teeth and incisors have high crowns, which ensure a long working life, despite the considerable attrition that takes place at the occlusal surfaces. Delayed formation of the roots also allows the cheek teeth to grow for some years after they come into wear. Attrition wastes the cheek tooth by 2 to 3 mm each year; to allow for this the greater part of the crown is initially embedded within the jaw and only gradually extruded to compensate for this loss. The enamel casing of the incisor and cheek teeth is also folded, although in different ways in the incisor, upper cheek, and lower cheek teeth series. The folding increases the area of the durable enamel presented at the working surface, where it stands proud of the neighboring dentine; the alternation of harder and softer tissues provides efficient grinding instruments (see Fig. 18.19).
The formula of the temporary dentition is

The incisor teeth are ranked together to form a continuous arch in each jaw and are so implanted that their roots converge (Fig. 18.17). Each is curved lengthwise, presenting a labial convexity. When in occlusion, the upper and lower incisors of the young animal form a continuous arch when viewed in profile. Later, as they wear, the upper and lower teeth meet at an increasingly pronounced angle. The occlusal surface recently brought into use is a broad transverse oval (Fig. 18.18B) and presents an outer enamel casing and an inner enamel ring lining the infolding known as the infundibulum; this is partially filled with cement, leaving a small cavity, the cup (Fig. 18.18/1). Because the enamel lining is more resistant, it projects above the surrounding dentine. Changes in the appearance of the occlusal surface provide the information principally used in aging older horses. The points to note are the depth of the infundibulum and its overlap with the dental cavity. Although it may appear that wear would eventually expose the pulp, this is prevented by the timely formation of secondary dentine, distinguishable from primary dentine by its darker color; this secondary dentine provides the feature known as the dental star (Fig. 18.18/3).
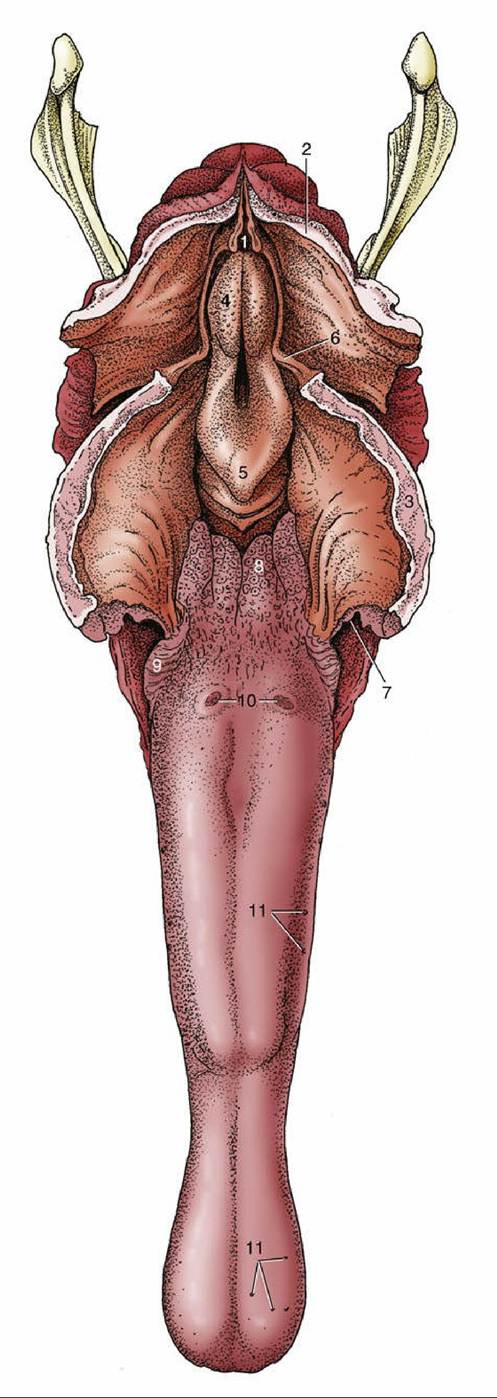
FIG. 18.16 The tongue and pharynx; the latter has been opened dorsally to expose the entrance to the larynx. 1, Entrance into esophagus; 2, dorsal wall of nasopharynx (split in median plane); 3, soft palate (split in median plane); 4, corniculate process of arytenoid cartilage; 5, epiglottis; 6, free border of soft palate, continued caudally by palatopharyngeal arch; 7, palatoglossal arch; 8, lingual tonsil; 9, foliate papillae; 10, vallate papillae; 11, examples of fungiform papillae.
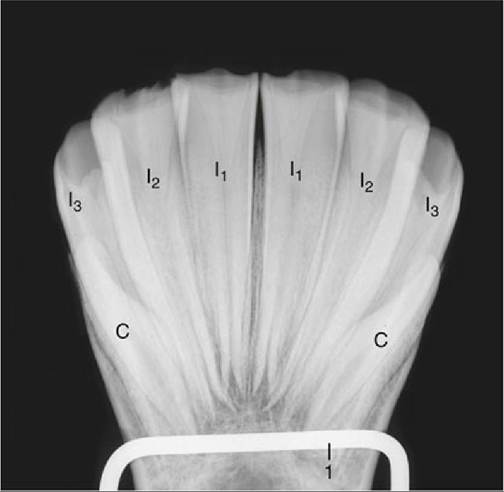
FIG. 18.17 Root convergence of permanent lower incisors; radiograph of a bone specimen from a 5- year-old (estimated) horse. Note the funnel-shaped infundibulum visible in each of the first and second incisors. I1,12, and I3, Lower first, second, and third incisors; C, lower canine tooth, present only in the male; 1, mounting wire of specimen.
Although canine teeth generally form in both sexes, they are rudimentary and commonly fail to erupt in mares. In male animals they are low, laterally compressed cones placed within the diastemas rather closer to the corner incisors than to the cheek teeth. The embedded portions are disproportionately large in relation to the exposed crowns.
The first premolar ("wolf" tooth) often fails to develop, and when present, it is vestigial and almost invariably confined to the upper jaw. Although it is without functional significance, it does have a potential nuisance value because it may shift under the pressure of the bit and so irritate the gum. It is easily extracted.
The remaining premolars (P2-P4) form a continuous row with the molars. The first and last of the six cheek teeth are somewhat triangular in section and the others rectangular; nonetheless, each is so like its neighbors that only an expert may distinguish isolated teeth (see Fig. 18.21). There are, however, important differences between the upper and lower sets; the upper teeth are much wider and exhibit a more complicated enamel folding, which creates two infundibula that fill with cement before eruption. The enamel of the lower teeth is also much folded but forms no infundibula (Fig. 18.19B). Most teeth occlude with two members of the opposing set along a relatively narrow area of contact that follows the lingual edge of the upper teeth and buccal edge of the lower teeth. The occlusal plane slopes ventrobuccally (Fig. 18.10). Irregular or incomplete chewing movements may cause the buccal edge of the upper cheek teeth and the lingual edge of the lower cheek teeth to escape wear (sharp teeth); the resulting protrusions must be filed down (floated) to prevent injury to cheeks and tongue.
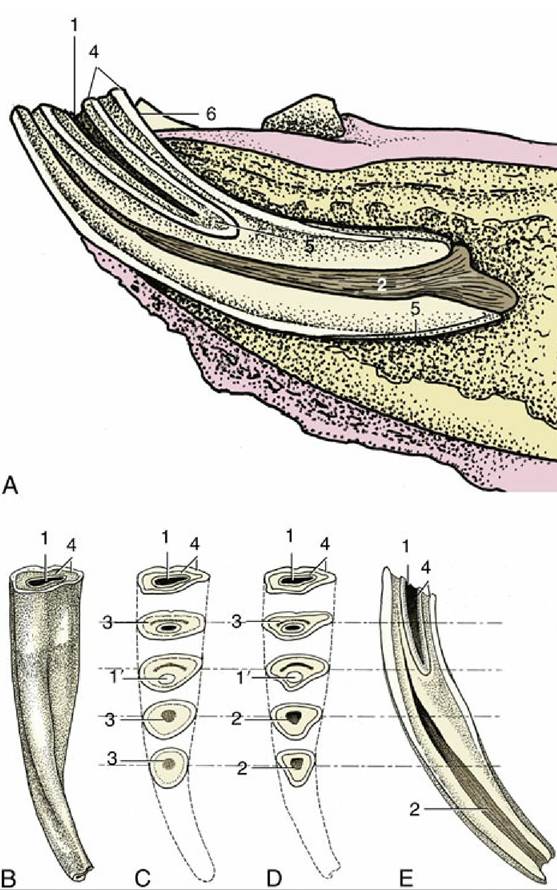
FIG. 18.18 Structure of a lower incisor. (A) In situ, sectioned longitudinally; the clinical crown is short in relation to the embedded part of the tooth. (B) Caudal view; the junction between the clinical crown and the rest of the tooth is not marked. (C) As a result of wear the occlusal surface changes; the cup gets smaller and disappears, leaving, for a time, the enamel spot; the dental star appears and changes from a line to a large round spot. (D) These are sawn sections of a young tooth for comparison. (E) Longitudinal section of incisor, showing the relationship between the infundibulum and dental cavity; the latter is rostral.
1, Cup, black cavity in center of infundibulum; 1', enamel spot, proximal end of infundibulum; 2, dental cavity; 3, dental star, changing in shape from a linear to a rounded form; 4, outer and inner enamel rings;
5, cement; 6, lingual surface.
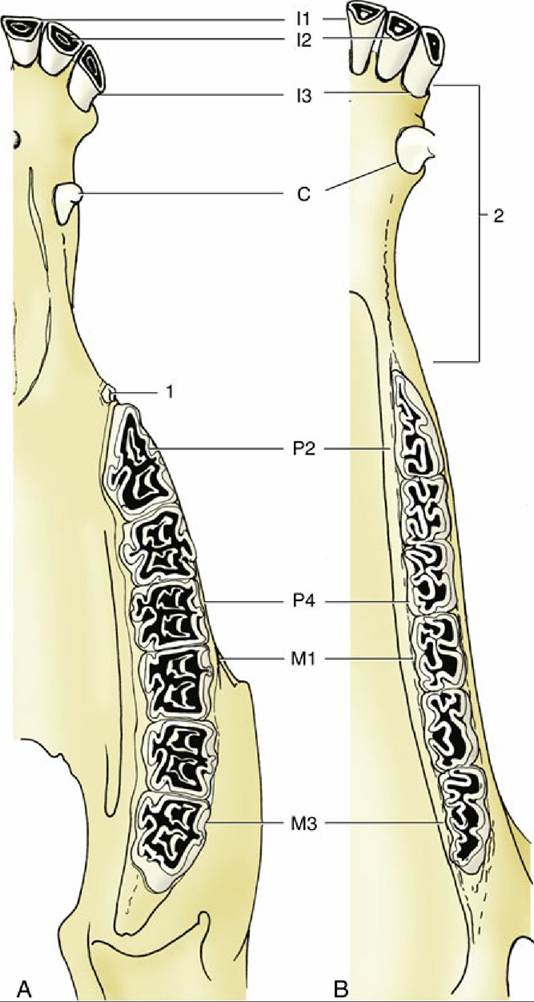
FIG. 18.19 The permanent teeth of the (A) upper and (B) lower jaws. 1, “Wolf” tooth (P1); 2, diastema.
The structure of the cheek teeth is shown in Fig. 18.20. The upper teeth are anchored by three or four roots and are so implanted that the reserve portions slope caudally at varying angles (Fig. 18.21). The relationship to the maxillary sinuses and other features of the skull is very helpfully revealed in radiographs. Only a thin plate of alveolar bone separates the molars from the sinus; in consequence, infection may easily spread to the sinus from tooth or alveolar abscesses. The relationship changes with age, partly because gradual extrusion lowers the alveolar floor, enlarging the sinus, and partly because the teeth migrate rostrally (Fig. 18.15).
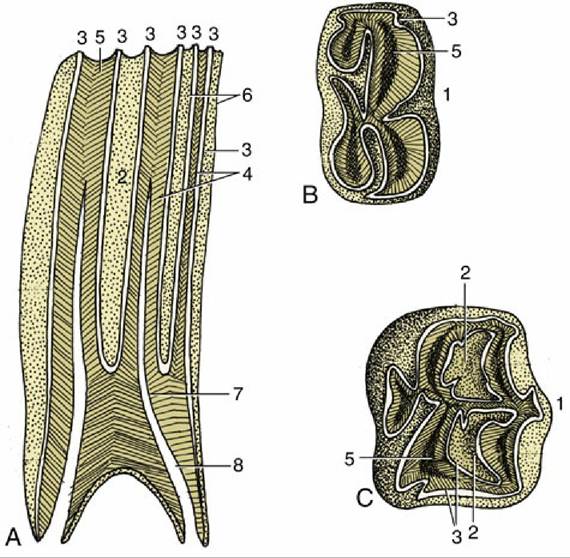
FIG. 18.20 Structure of the cheek teeth shown in sagittal section (A) and by views of the occlusal surface of lower (B) and upper (C) molars. 1, Buccal (labial) surface; 2, infundibulum; 3, enamel; 4, dentine; 5, secondary dentine; 6, cement; 7, dental cavity; 8, root canal.
The transitory swellings occasionally seen on the ventral margin of the mandible of 2- to 4-year- old horses are produced by modeling of the mandible to accommodate the formation of the roots of permanent teeth, which are prevented from rising within the jaw by remnants (caps) of deciduous predecessors blocking the way (Fig. 18.22). When the remnants are shed, their successors can move into place. Further modeling of the mandibular border erases the swellings.
Simple extraction of cheek teeth is more or less impossible. Their length, curvature, and close fit would hamper any effort to draw one out past its neighbor(s), even were the attempt permitted by the small size of the opening between the lips and the depth of the oral cavity (Fig. 18.23). Instead, they must be removed by expulsion, that is, by means of a punch brought to bear over the root in an operation of some severity and difficulty involving the opening of a window through bone. Accurate determination of the position of the root of the tooth involved is essential, and for this it is necessary to be mindful of how the dispositions of the teeth change with age. The approach to a caudal member of the upper cheek teeth series is made via the caudal maxillary sinus or the frontal and caudal maxillary sinuses when M3 is involved.
The deciduous teeth generally resemble the permanent teeth but are much smaller and significantly shorter in relation to their breadth. The deciduous incisors are constricted at the neck and are much whiter than their replacements because the porcelain-like enamel is unobscured by the cement encrustation that gives permanent teeth a slightly yellow and porous appearance. Some longitudinal striation is apparent on the temporary incisor crown.
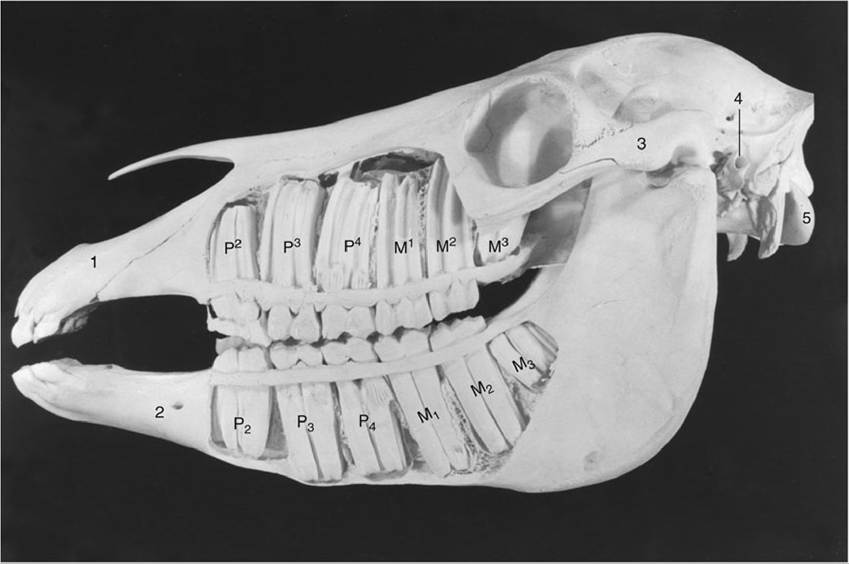
FIG. 18.21 Exposed cheek teeth of a horse 2½ years old (estimated). Upper Jaw: The deciduous premolars are still present, p2 in the form of a cap; M3 has not yet erupted. LowerJaw: The deciduous premolars 3 and 4 are still present in the form of caps; M3 has not yet erupted. 1, Incisive bone; 2, mental foramen; 3, zygomatic arch; 4, external acoustic meatus; 5, occipital condyle.