The Pathological Consequences of Cardiac Defects Are Direct Results of the Abnormal PressuresfVoIumes, and Workloads Created in the Cardiac Chambers
Figure 21-10 summarizes the pathological consequences associated with some common cardiac defects. First, consider mitral regurgitation. With each contraction of the left ventricle, a normal volume of blood is ejected into the aorta, and an additional volume of blood is ejected backward (through the regurgitant valve) into the left atrium.
As a result, there is an increase in the volume work performed by the left ventricle. Therefore, mild to moderate left ventricular hypertrophy develops. Also, in a heart with mitral regurgitation, the left atrium becomes distended, and left atrial pressure increases, as does pulmonary venous pressure. Elevated pressure in the pulmonary blood vessels forces water and electrolytes out of the bloodstream and into the pulmonary interstitial spaces, causing pulmonary edema. When left atrial pressures exceed about 20 mm Hg, pulmonary edema becomes so severe that the lungs’ ability to transfer oxygen into the bloodstream is substantially reduced. The result is respiratory distress.The consequences of mitral regurgitation are usually more noticeable during exercise than during rest. One reason is that despite the regurgitation, the left ventricle can usually adapt
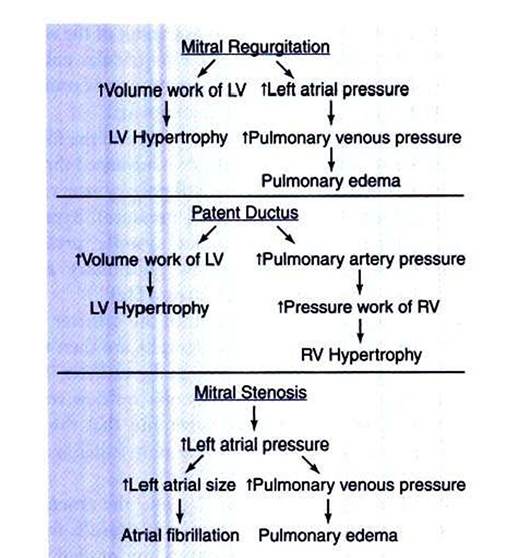
FIGURE 21-10 Pathological consequences of several common cardiac defects. LV, Left ventricle; RV, right ventricle.
enough through hypertrophy and an increase in heart rate to maintain a normal cardiac output into the aorta (and therefore into the systemic circulation) at rest. Also» despite some pulmonary edema, the oxygenation of the blood is sufficient to meet the animals needs during rest. During exercise, however, the output of the left ventricle into the systemic circulation must increase several-fold to supply adequate blood to exercising skeletal muscle.
Also, the delivery of oxygen into the blood must increase several-fold. Despite the hypertrophy, the left ventricle may not be able to deliver adequate blood flow to the systemic circulation during exercise if mitral regurgitation is serious. Also, pulmonary edema may prevent delivery of enough oxygen into the blood to support the metabolism of the exercising animal.Consider next the abnormalities associated with aortic stenosis (not shown in Figure 21-10). To eject a normal volume of blood with each beat through a stenotic aortic valve, the left ventricle must develop an abnormally high systolic pressure. This increases the pressure work of the left ventricle, which leads to a marked left ventricular hypertrophy. I he hypertrophy has the desirable effect of increasing the contractility of the left ventricular muscle so that it can generate the increased pressure required to maintain normal cardiac output. As hypertrophy progresses, however, the ventricular muscle begins to impinge on the aortic outflow pathway, which further hampers the ability of the ventricle to eject blood. In a sense, the hypertrophic ventricular muscle “gets in its own way” or becomes muscle bound. The resulting limitation in aortic outflow is much more likely to be a problem during exercise than at rest. A patient with aortic stenosis may be able to function normally at rest but characteristically exhibits exercise intolerance.
Patent ductus arteriosus (PDA) is a defect that typically results in both left and right ventricular hypertrophy (Figure 21-10). In a typical patient with a PDA, the left ventricle pumps a near-normal volume of blood per minute to the systemic circulation and also pumps two to three times that volume of blood per minute through the PDA. As a result, the volume work done by the left ventricle greatly exceeds normal amounts, which leads to left ventricular hypertrophy. The blood flowing through the PDA enters the pulmonary artery, and thus pulmonary arterial pressure exceeds normal levels.
This in turn increases the pressure work that must be done by the right ventricle. The right ventricle receives a near-normal volume of blood back from the systemic circulation each minute, and the right ventricle must generate an elevated systolic pressure to eject this blood into the high-pressure pulmonary artery. The increased pressure work for the right ventricle is a powerful stimulus for hypertrophy, and pronounced right ventricular hypertrophy develops.As a patient with PDA grows, exercise intolerance becomes evident. Despite hypertrophy, the left ventricle cannot supply the increased blood flow needed by growing, exercising skeletal muscles, in addition to the blood that flows through the PDA. In patients with PDA the pulmonary artery and the pulmonary blood vessels must carry not only the blood that is pumped by the right ventricle (as in a normal animal), but also the blood that is pumped through the PDA. In a severe case, pulmonary blood flow can be more than four times greater than normal. The resulting increases in pulmonary vascular pressure can lead to pulmonary edema. Surgical repair of a PDA in a young animal leads to a rapid reversal of all these pathological changes.
An understanding of the preceding examples should make it easy to predict the pathological consequences of a ventricular septal defect. These consequences include increased volume work of the left ventricle, moderate left ventricular hypertrophy, increased volume and pressure work of the right ventricle, pronounced right ventricular hypertrophy, increased blood flow through the lungs, possible pulmonary edema, and probable exercise intolerance. It should also be clear why pulmonic stenosis leads to increased pressure work for the right ventricle and pronounced right ventricular hypertrophy (see Clinical Correlations).
Figure 21 -10 also summarizes the pathological consequences associated with the diastolic murmur of mitral stenosis. The left atrial pressure must exceed normal levels to force a normal volume of blood through the stenotic mitral valve and into the left ventricle during each ventricular diastole.
The elevated left atrial pressure distends the left atrium. There may be some hypertrophy of the atrial muscle. The atrium continues to function, however, mainly as a reservoir to collect and hold blood during ventricular systole, rather than as a pumping chamber to force blood into the ventricle during its diastole. One problem is that atrial action potentials tend to become discoordinated in a distended atrium, and atrial fibrillation is a common consequence. Also, the increase in the left atrial pressure causes blood to back up and accumulate in the pulmonary blood vessels, so pulmonary edema is likely. It might seem that the backup of blood in the pulmonary vessels would eventually also increase the pressure in the pulmonary artery and thereby increase the pressure work of the right ventricle. In other words, mitral stenosis might be predicted to lead to right ventricular hypertrophy. This prediction is logical, but in practice, animals with greatly elevated left atrial pressures usually die from the effects of pulmonary edema before right ventricular pressures have had a chance to become high enough to induce right ventricular hypertrophy. Therefore, mitral stenosis does not generally lead to hypertrophy of either ventricle.The defect of aortic regurgitation leads to left ventricular hypertrophy. With each systole, the left ventricle must eject an abnormally large volume of blood into the aorta. Of this, a normal volume of blood goes on into the systemic circuit; the rest is simply regurgitated back from the aorta into the left ventricle during diastole. Thus the volume work of the left ventricle is increased to above-normal levels, and left ventricular pressures may rise as well. Both these factors stimulate left ventricular hypertrophy. In severe cases of aortic regurgitation, diastolic ventricular pressure becomes elevated (because during diastole the left ventricle receives blood from both the left atrium and the aorta). This leads to increases in left atrial pressure, and pulmonary edema may develop.
Consideration of the abnormalities associated with cardiac defects is important for two reasons. First, these defects and their consequences are often encountered in veterinary medicine. Second, this discussion illustrates how the clinical signs and consequences of disease states can be understood and predicted in a rational way, on the basis of an understanding of basic principles of cardiac physiology.