THE PERICARDIUM AND THE TOPOGRAPHY OF THE HEART
The heart is almost completely invested by the pericardium, which fits snugly about it (Figure 7-5). The pericardium is essentially a closed serous sac that is so deeply invaginated by the heart that its lumen is reduced to a mere capillary cleft (Figure 7-5/4).
The space contains serous fluid, normally just sufficient in amount to allow easy movement of the heart wall against its covering. The visceral and parietal layers of the pericardiumid="Picutre 296" class="lazyload" data-src="/files/uch_group31/uch_pgroup304/uch_uch7232/image/image286.jpg">
Figure 7-2 Left lateral view of the aortic arches and their transformation. A, Dorsal and ventral aortae are connected by the first aortic arches. B, First and second aortic arches are present. C, The first arch begins to disappear, the third is complete, and the fourth and sixth develop. D, The third arch and the cranial part of the dorsal aorta are now transformed into the internal carotid artery, while the sixth gives rise to the pulmonary trunk and ductus arteriosus. 1-4, 6, Aortic arches; 1,-4,, pharyngeal pouches; 7, 7, ventral and dorsal aortae; 8, internal carotid artery; 9, ductus arteriosus; 10, left pulmonary artery; 11, brain vesicle; 12, foregut; 13, lung bud.
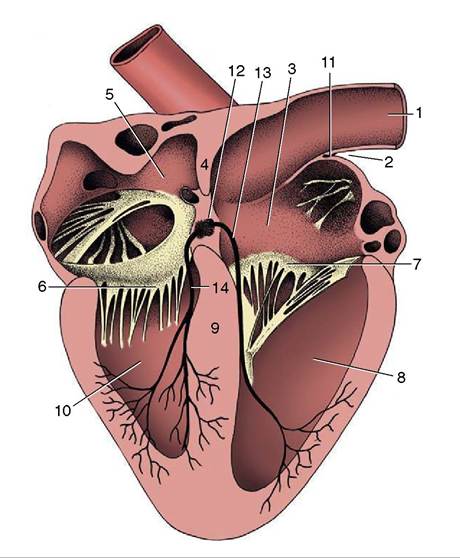
Figure 7-3 Section of the heart exposing the four chambers. 1, Cranial vena cava; 2, terminal sulcus; 3, right atrium; 4, interatrial septum; 5, left atrium; 6, left atrioventricular valve; 7, right atrioventricular valve; 8, right ventricle; 9, interventricular septum; 10, left ventricle; 11, sinuatrial node; 12, atrioventricular node; 13, 14, right and left limbs of atrioventricular bundle.
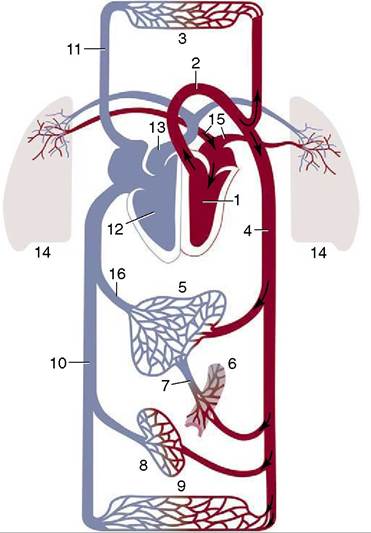
Figure 7-4 Schematic drawing of the systemic and pulmonary circulation.
1, Left ventricle; 2, aorta; 3, capillary bed of head, neck, and forelimb; 4, abdominal aorta; 5, liver; 6, capillary bed of intestines; 7, portal vein; 8, capillary bed of kidneys; 9, capillary bed of caudal part of the body; 10, caudal vena cava; 11, cranial vena cava; 12, right ventricle; 13, pulmonary trunk; 14, capillary bed of lungs; 15, pulmonary vein; 16, hepatic veins.continue into each other at a complicated reflection that runs over the atria and the roots of the great vessels. The visceral layer is so closely adherent to the heart wall that it may be described as a component of this, the epicardium. The parietal layer obtains a thick external fibrous covering (Figure 7-5/6) that blends with the adventitia of the great vessels dorsally and continues into a ligament at the ventral apex of the sac. This usually attaches to the sternum (sternopericardial ligament; Figure 7-5/8) but attaches to the diaphragm (phrenicopericardial ligament) in species in which the heart axis is more oblique. These attachments place a severe restraint on the mobility of the heart, although slight movement does occur with each respiratory excursion.
Although the pericardium distorts to accommodate the changing form of the heart during the cardiac cycle, its fibrous component prevents any significant distention in the short term. It may stretch over longer periods should the heart become enlarged by exercise or disease or should effusion or pus collect within the pericardial cavity.
The heart (within the pericardium) is included within the mediastinum, the partition that separates the right and left pleural cavities (see Figure 4-20, A). It is conical and is placed asymmetrically within the thorax, and the larger part (about 60%) lies to the left of the median plane (see Figures 13-13, B, and 20-8). The base is dorsal and reaches approximately to the horizontal (dorsal) plane that bisects the first rib; in some species (e.g., the dog) it is tilted in varying degree to face craniodorsally.
The apex is placed close to the sternum, opposite the sixth costal cartilage. The long axis that joins the center of the base to the apex thus slopes cau- doventrally, with some deviation to the left imposed by the skewed orientation (Figure 7-6). The projection of the heart on the chest wall extends between the third and sixth ribs (or thereabouts); thus, much of the heart is under cover of the forelimbs, which is a considerable handicap to clinical examination, especially in larger species (see Figures 20-1, 20-2, and 27-2).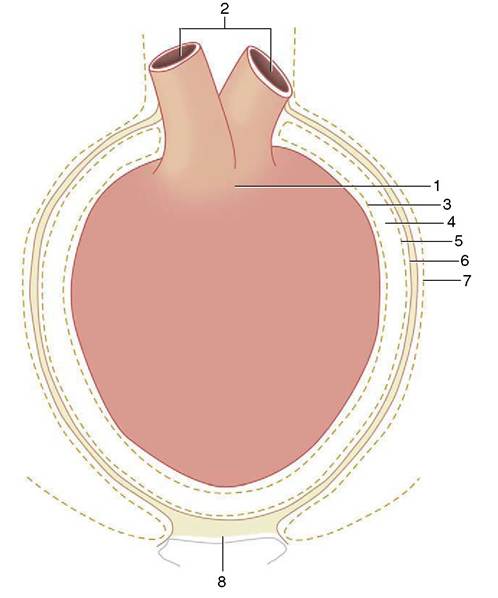
Figure 7-5 Schematic illustration of the pericardium. 1, Heart; 2, great vessels; 3, visceral pericardium (epicardium); 4, pericardial cavity (exaggerated in size); 5, parietal pericardium; 6, connective tissue layer of the parietal pericardium; 7, mediastinal pleura; 8, sternopericardial ligament.
Although generally conical, the heart displays some lateral compression to conform to the similar compression of the thorax of most quadrupeds. This better defines right and left surfaces that face toward the corresponding lungs, which are shaped to fit. The cardiac notch in the ventral border of each lung allows the heart a restricted contact with the chest wall, which is normally greater on the left side because of the asymmetrical position (see Figure 13-5). Each lateral surface is also crossed by the corresponding phrenic nerve. The cranial aspect is extensively related to the thymus (in the young animal), but the caudal surface faces toward the diaphragm and may be indirectly related through this to cranial abdominal organs (see Figure 28-14), which is a point of importance in certain species (p. 687).