There Are at Least Three Distinct Mechanisms of Sodium Absorption
The first pathway of sodium absorption is through sodium co-transport proteins, as previously discussed. This secondary active transport pathway is not only the mechanism for glucose and amino acid absorption (Figure 30-17, A), but also a major means of sodium absorption.
The second sodium absorption mechanism is through the Na7H+ exchanger (Figure 30-17, B), mentioned previously as an example of an ion exchanger, or antiport. Through this mechanism, intracellular Hi is exchanged for luminal Na+ across the apical membrane. The H’ for this exchange is formed by the action of carbonic anhydrase, which generates HCO3 as well as H+. As H+ is exchanged for Na*, HCO3" concentrations build up in the cell. The resulting transcellular HCO3' gradient drives the action of the C17HCO3" exchanger, which results in the exchange of intracellular HCO3' for luminal Cl". Because of the close connection between Na’ and Cl' absorption by these pathways, this transport mechanism is often called coupled sodium chloride transport, as illustrated in Figure 30-17, B. One must appreciate, however, that it is only the intracellular balance of H" and HCO3" that couples the two exchange pathways. 'Γhere are instances in which the intracellular pH is such that Na7H* exchange occurs without C17HCO√ exchange, and vice versa.
Coupled sodium chloride absorption is usually most active in the ileum and colon, where the sodium concentration in the gut is usually relatively low compared with that in the
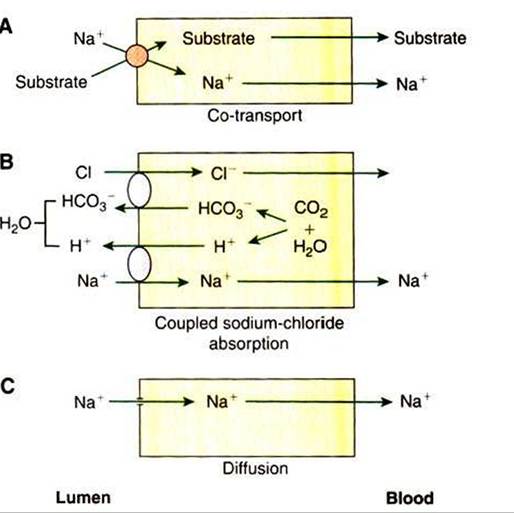
FIGURE 30-17 Three mechanisms of sodium (Na*) absorption. A, Sodium co-transport with organic molecules is a major means of sodium uptake during active digestion and absorption.
B, Chloride-coupled sodium absorption is also an important means of sodium absorption and requires the action of carbonic anhydrase and the existence on the apical membrane of bicarbonate-chloride (HCO37CΓ) and sodium-hydrogen (Na7H*) exchange mechanisms. C, Simple diffusion of sodium across the apical membrane may occur because of the large, favorable concentration gradient, but it is a relatively minor means of sodium absorption. H2O, Water; CO2, carbon dioxide.
duodenum and jejunum. As usual, sodium entering the enterocytes is transported across the Basolateral membrane to the lateral spaces by the action of the Na+,K+-ATPase pump. Chloride, however, remains in the enterocyte until its concentration is high enough to promote the diffusion of chloride through special channels, or gates, in the basolaleral membranes. The rate of absorption of sodium and chloride by the coupled mechanism appears to depend on the permeability of the chloride channels; when the permeability is high, chloride passes rapidly out of the enterocyte, allowing continued chloride absorption. Conversely, when chloride channels are relatively closed, the intracellular chloride concentration rises, diminishing chloride absorption by the creation of an unfavorable concentration gradient across the apical membrane.
The third mechanism of sodium absorption is by simple diffusion through ion channels in the apical membrane (Figure 30-17, C). The large electrochemical gradient that can exist for sodium across the enterocyte apical membrane allows direct, uncoupled movement of sodium across the membrane when the ion channels are open. Although some sodium absorption probably occurs by this mechanism, its overall importance in body sodium homeostasis is probably not great.
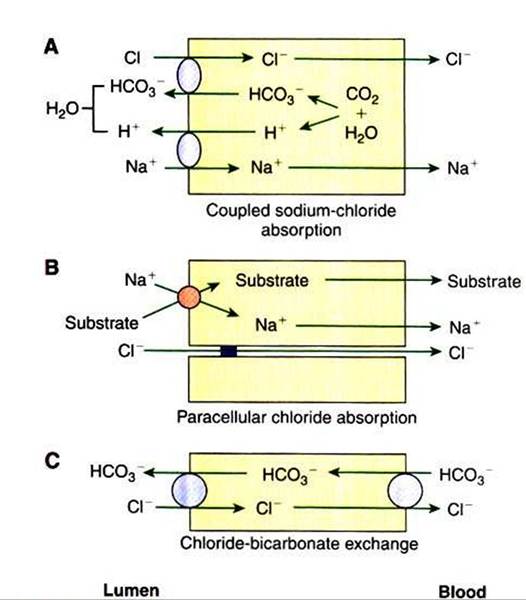
FIGURE 30-18 ∙ Three mechanisms of chloride (CΓ) absorption. A, Chloride-coupled sodium absorption is directly related to sodium (Na*) uptake. B, Paracellular chloride absorption is indirectly related to sodium absorption that occurs during co-transport. C, Chloridebicarbonate (Ct∕HCO3~) exchange occurs especially in areas where bicarbonate secretion into the intestinal lumen is important.