Urine Acidification
Intercalated cells in the walls of collecting ducts are capable of the active transport of hydrogen ions into the tubular lumen to acidify the urine. This system can generate a difference between blood and urine of about 3 pH units, so if blood pH is 7.4, urine with a pH of 4.4 can be formed.
The hydrogen ions to be secreted are generated in intercalated cells by the hydration of carbon dioxide under the influence of carbonic anhydrase. A bicarbonate ion is also generated during this process, and these are secreted into the extracellular fluids at the base of the cell, from where the bicarbonate can diffuse into the plasma (Fig. 23-13).The secretion of hydrogen ions by intercalated cells is regulated in part by the concentrations of carbon dioxide and bicarbonate ions in the plasma and other extracellular fluids. if carbon dioxide concentration increases or if bicarbonate ion concentration decreases, the rate of hydrogen ion secretion accelerates, and urine becomes more acidic. The importance and relevance of this regulation by carbon
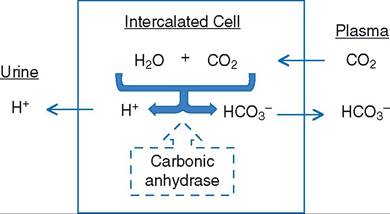
Figure 23-13. Formation and secretion of hydrogen and bicarbonate ions by intercalated cells. Formation of hydrogen and bicarbonate from water and carbon dioxide in the cell is promoted by the action of intracellular carbonic anhydrase.
dioxide or bicarbonate to the regulation of overall acid-base balance is discussed in a later section of this chapter.
some of the secreted hydrogen ions combine with HPO4-2 ions in the tubular fluid to form H2PO4-. In this manner, HPO4-2 acts as an intratubular buffer to reduce the concentration of free hydrogen ions and prevent the urine pH from dropping too low. The phosphate ions originally entered the tubular fluid as part of the glomerular filtrate.
Ammonia may also serve as an intratubular buffer (forming ammonium ions), and it is secreted into the tubular fluid by the collecting duct.Regulation of Acid-Base Balance
The pH of blood plasma and other extracellular fluids is maintained relatively constant within a narrow range (about 7.35 to 7.45). It is important to maintain this constancy because enzyme activity and metabolic processes require close control of pH for optimal function. Three major mechanisms function together to prevent the development of an abnormal pH. These are (1) extracellular and intracellular chemical buffers, (2) ventilatory control of plasma carbon dioxide, and (3) urinary excretion of bicarbonate or an acid urine as needed.
Extracellular and Intracellular Buffers
A chemical buffer system acts to maintain a constant pH by either donating or removing free hydrogen ions in a solution (see Chapter 2).
The bicarbonate buffer system is quantitatively the most important chemical buffer in blood plasma and other extracellular fluids. Bicarbonate is the base in this system, and the acid is carbonic acid. However, because carbonic acid is difficult to measure and in body fluids it is in equilibrium with carbon dioxide, the levels of carbon dioxide are routinely used as indicators of carbonic acid levels.
The bicarbonate buffer system is the most important body buffer system from a physiologic standpoint, because the concentrations of the components of the system can be rapidly adjusted by changes in either renal excretion of bicarbonate or pulmonary ventilation to remove carbon dioxide. Bicarbonate is avidly reabsorbed by renal tubules, but a renal threshold value permits rapid excretion of excess bicarbonate. Also, plasma carbon dioxide levels are normally the primary regulator of ventilation, so these levels are also under constant control.
Figure 23-14 summarizes the roles of the urinary and respiratory systems in maintaining the concentrations of the components of the bicarbonate buffer system.
Note that free hydrogen ions and bicarbonate ions can be excreted in the urine, while carbon dioxide is excreted via the respiratory system. Because carbon dioxide is a potential acid (it is in equilibrium with carbonic acid) and can be excreted in expired air, it is termed a volatile acid. The respiratory system is responsible for excreting this potential volatile acid produced by cellular metabolism. Other acids in body fluids, such as lactic acid, are not volatile, and the kidneys are responsible for excreting these non-volatile acids. The A- shown in Figure 23-14 represents the anion of non-volatile acids (e.g., lactate) that may be produced by cellular metabolism or absorbed from the gastrointestinal tract.Both intracellular and extracellular proteins function as buffers; that is, these proteins are capable of accepting excess hydrogen ions or donating free hydrogen ions to assist in the maintenance of a stable pH. Because of the large quantity of intracellular proteins in organs such as skeletal muscle, intracellular proteins account for a large percentage of the total buffering capacity in the body. However, intracellular buffers cannot be as easily regulated as the bicarbonate buffer system in the extracellular fluid, and hydrogen ions from the extracellular fluid must enter cells to be buffered by the intracellular proteins (Fig. 23-14). Hemoglobin proteins in erythrocytes are a major contributor to the total buffering capacity of whole blood.
Acids and bases are produced by normal cellular metabolism and are constantly being added to the ECF (Figure 23-14). Acids and bases are also added to the ECF by gastrointestinal absorption. Normally, these additions are balanced by the actions of the urinary and respiratory systems so that extracellular fluid pH (Fig. 23-14) and the status of body buffer systems, including intracellular proteins, remain stable. However, the ability of these mechanisms to maintain a normal pH can be overwhelmed during metabolic disturbances or after the absorption of large amounts of acids or bases from the gastrointestinal tract.
Ruminal or lactic acidosis is seen in ruminants that ingest large amounts of carbohydrates, usually grain, over a short period.
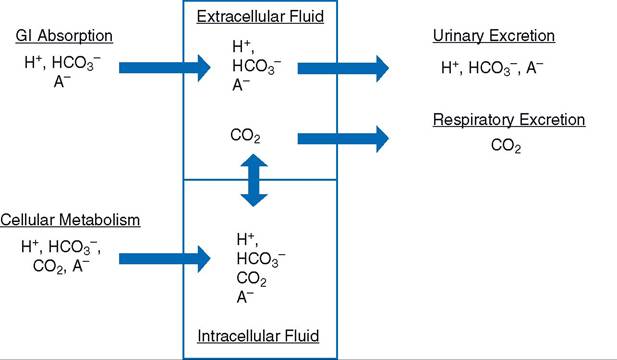
Figure 23-14. Primary factors affecting extracellular fluid pH. The A- refers to a variety of anions such as lactate. The arrow between intracellular and the extracellular fluids indicates that exchanges can occur in either direction, but this exchange is limited by the abilities of the different ions to cross cell membranes.
The sudden ingestion of the concentrated carbohydrates alters the microbial population in the rumen, favoring the rapid growth of organisms that produce lactic acid. The rapid increase in lactic acid absorption into the blood overwhelms the ability of the pH regulatory systems, and systemic acidosis develops.
Classification of Alkalosis and Acidosis and Compensation
Alkalosis is a condition in which the pH of body fluids (including blood) is abnormally high, and acidosis is a condition in which the pH is abnormally low. Acidosis or alkalosis can be classified as being either metabolic or respiratory, to indicate the cause of the pH imbalance. The term respiratory refers to acid-base imbalances that come about as a result of primary or initial changes in carbon dioxide levels. The term metabolic refers to all other causes of acid-base imbalances.
When an acid-base imbalance arises and the buffering capacities of the extracellular and intracellular chemical buffers are overwhelmed, the body systems primarily responsible for acid-base balance (respiratory and urinary) should respond. This response may lead to a state of compensation, so that the acid-base imbalance is less severe than if the compensation (or response) had not occurred. For example, chronic lung diseases may result in an accumulation of carbon dioxide and a respiratory acidosis. The kidneys compensate for the respiratory acidosis by producing a more acidic urine and retaining base (bicarbonate).
An increase in blood bicarbonate concentration is an indicator of renal compensation for the primary respiratory acidosis.Because of its importance as the major extracellular buffer system and because the components of the system can be readily determined in clinical laboratories, the status of the bicarbonate buffer system is used to evaluate overall acid-base balance. The primary cause of acidosis or alkalosis is routinely diagnosed by evaluation of the bicarbonate buffer system.
Metabolic alkalosis is a primary increase in bicarbonate ions. Causes include excessive ingestion of alkaline salts or gastric vomiting, during which hydrochloric acid is lost from the body fluids. The body compensates for metabolic alkalosis by hypoventilation to retain carbon dioxide and by increasing urinary bicarbonate excretion.
Metabolic acidosis is a primary decrease in bicarbonate ions. Causes include (1) excessive loss of bicarbonate via diarrhea (e.g., calf scours); (2) excessive formation of metabolic acids as a result of metabolic disturbances (e.g., diabetes mellitus, starvation, and lactic acidosis during shock); (3) inability of the kidneys to excrete acid (e.g., renal failure); and (4) absorption of excess acid from the gastrointestinal tract (e.g., ruminal acidosis). The body compensates for metabolic acidosis by hyperventilation and excretion of a more acid urine if possible.
Respiratory alkalosis is a primary deficit in carbon dioxide (hypocapnia is low blood carbon dioxide). Causes include (1) exposure to high altitudes, where low oxygen tension causes hyperventilation; (2) a high fever, which may produce hyperventilation; and (3) inflammation or diseases of the brain, which stimulate the respiratory centers. The kidneys compensate for respiratory alkalosis by increasing excretion of bicarbonate ions in the urine.
Respiratory acidosis is a primary excess of carbon dioxide (hypercapnia is elevated blood carbon dioxide). Causes include pneumonia, pulmonary fibrosis, pulmonary edema, airway obstructions, and breathing air that is high in carbon dioxide. The kidneys compensate for the primary respiratory problem by excreting a more acid urine and secreting additional bicarbonate into the blood. Note in Figure 23-13 that a bicarbonate ion is also produced when intercalated cells generate a hydrogen ion for urine acidification, and that the bicarbonate ion can be secreted into the blood. Plasma levels of bicarbonate may increase as the compensatory response continues.