WATER BALANCE
18.15.1 Water Gain
Water gains occur by ingestion of water along with food and also from metabolic water. Metabolic water is derived from the chemical reactions of cellular metabolism in the mitochondria.
The metabolism of proteins, carbohydrates, and fats requires different amounts of cofactors, with the greatest amounts required for fats. Accordingly, the yield of metabolic water is greater for a certain amount of fat than for an equal amount of protein or carbohydrate. For example, the metabolic water yield from each of 100 g of carbohydrate, protein, and fat is 60 ml, 40 ml, and 110 ml respectively.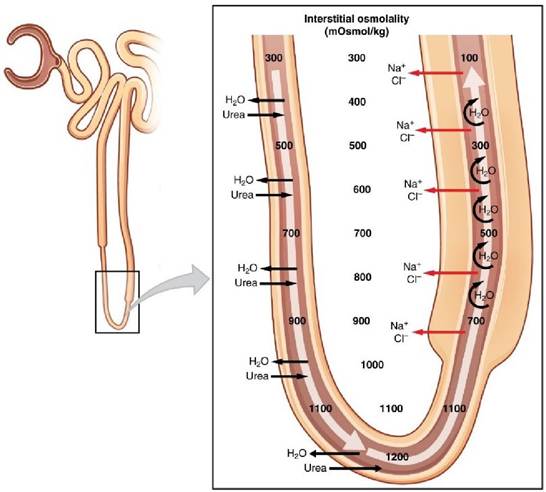
FIGURE 18.7 Countercurrent multiplier in loop of Henle.
18.15.2 Water Loss
Water loss from the body is classified as either an insensible loss or a sensible loss. Insensible losses are associated with vapor losses and occur constantly by evaporation from the skin and by loss of water vapor in exhaled air. Inhaled air becomes saturated with water vapor in the respiratory passages and lungs, but there is no body mechanism to remove moisture from the respiratory gases before exhalation. Sensible losses are the visible losses in the form of urine, feces, and body secretions that leave the body. Sensible losses can become excessive in certain conditions, such as diarrhea, and threaten body stores of water.
18.15.3 Regulation of Acid-Base Balance
The regulation of acid-base balance actually means regulation of [H+] in the body fluids. The [H+] is usually expressed in terms of pH, which is the negative log of the hydrogen ion concentration. pH = log 1 /[H+ ] = -log[H+]. The pH of the extracellular fluid (ECF) is generally 7.4. Relatively small pH changes are associated with correspondingly large changes in H+ concentration.
Enzymatic reactions and metabolic processes in the cells of the body operate optimally within a very narrow range of pH (7.35 to 7.45). Therefore, if any deviations occur from this pH value, mechanisms are present in the body to make corrections for the deviations. Most of the acids and bases in the extracellular fluid that are involved in normal acid-base regulation are weak acids and weak bases. The normal range of blood pH may be assumed to be 7.35 to 7.45. To resist acid-base disturbances, the body uses three basic mechanisms1. 1. Chemical buffering - immediately combining with acid or base to prevent excessive changes in H+ concentration.
2. Respiratory adjustment of blood CO2 concentration - regulates the removal of CO2 (and therefore, H2CO3) from the extracellular fluid.
3. Excretion of H+ or HCO3- ions by the Kidneys - can excrete either acid or alkaline urine, thereby readjusting the extracellular fluid H+ concentration toward normal during acidosis or alkalosis.
A chemical buffer system consists of a mixture of a weak acid and its conjugate base, example is a solution of carbonic acid and bicarbonate ion. The Henderson-Hasselbalch equation describes the relationship between pH and the mixture of a weak acid and its conjugate base as pH= pKa log [Base]∕[Acid]. Ka is the dissociation constant of the weak acid and Pka is the negative logarithm of Ka. pKa is defined as the pH at which the acid and base of the buffer system are in equal concentration. Thus, pH = pKa when base and acid are equal.
When an acid is added to the buffer system, a shift of pH is resisted, but the ratio of base to acid decreases and pH is somewhat depressed. If further acid will be added, buffers system will be exhausted and acidemia will result. The restoration requires the formation and secretion of H+ ions by the kidney tubules. If instead strong base were added to the body fluids, it would react with the acid of the buffer and thus form more buffer base.
This ultimately must be corrected by renal excretion of base and retention of hydrogen ions. The principal buffer systems of the blood are the bicarbonate, protein, phosphate and Haemoglobin.18.15.4 Bicarbonate Buffer System
The bicarbonate buffer system is the principal buffer of the blood and the ECF. The weak acid component of the bicarbonate buffer system is H2CO3 and the conjugate base is HCO3-. pH = pK + log [HCO3-]/ [H2CO3]. Bicarbonate is formed in the body by the reaction of carbon dioxide with water.
When a strong acid (Hcl) is added to the bicarbonate buffer solution, the increased H+ from the acid is buffered by HCO3-. As a result, more H2CO3 is formed, causing higher production of CO2 & H2O. The excess CO2 greatly stimulate respiration which eliminate the CO2 from the ECF. Opposite reaction takes place when strong base, NaOH is added to bicarbonate system. Here concentration of H2CO3 decreases, and net result is decreased concentration of blood CO2 level. This inhibits respiration and decreases the rate of CO2 expiration. For bicarbonate buffer system, pK is 6.1
18.15.5 Phosphate Buffer System
It plays a major role in buffering renal tubular fluid and intracellular fluids (ICF). The main component is H2PO4 and HPO4- so when strong acid (Hcl) is added.

Here strong acid, Hcl is replaced by weak acid NaH2PO4 and the decrease in pH is minimized. When a strong base, NaOH is added, the OH- is buffered by the H2PO4 to form additional amount of HPO4- & H2O. Phosphate buffer system has pK of 6.8 which is very near to the normal pH of 7.4. The phosphate buffer is especially important in tubular fluid of kidney for two reasons. Phosphate usually becomes highly concentrated in the tubules, hence increasing the buffer power of the phosphate system.
Tubular fluid usually has lower pH than the ECF, hence it brings the operating range of buffer closer to the pK (6.8) of the system. The phosphate buffer system is important in buffering ICF for two reasons: The concentration of phosphate is many times higher in ICF than ECF. Also, the pH of ICF is lower than that of ECF and therefore it is closer to the pK of the phosphate buffer system compared with the ECF.18.15.6 Protein Buffer System
Proteins are among the most plentiful buffers in the body because of their high concentration intracellularly. Approximately 60-70% of the total chemical buffering of the body fluid is inside the cells, and most of this results from the intracellular proteins. In addition to the high concentration of proteins in the cells, another factor that contributes to their buffering power is the fact that the pK of many of the proteins system are very close to intracellular pH.
18.15.7 Excretion and Osmoregulation
The maintenance of fluid balance is critical for maintaining many bodily functions, including metabolic and biochemical reactions, transport of nutrients and maintenance of temperature. The average adult animal has roughly 60% fluid volume. These body fluids may again be subcategorized into intracellular and extracellular fluid compartments.
Intracellular fluid is all the fluid contained within cells. The intracellular fluid makes up roughly two-thirds of the total body volume.
The remaining one-third of fluid volume in the body is constituted by extracellular fluid and may further divide into its interstitial, intravascular and transcellular compartments.
The maintenance of fluid homeostasis in each of these compartments is mainly dependent on the concentration of electrolytes and this electrolyte is responsible for generation of osmotic pressure. This process regulation of osmotic pressure is known as osmoregulation.
To maintain homeostasis, it is essential that the excretion of water and electrolytes match an individual’s intake.
The kidneys play a very essential role in osmoregulation by controlling the quantity of fluid reabsorbed from the glomerular filtrate. This fluid is reabsorbed in the renal tubes and may be modulated by the hormones like antidiuretic hormone (ADH), aldosterone, and angiotensin II. The kidney has large capacity to alter fluid excretion, as well as electrolyte excretion.The glomerular filtration rate value in an average human being is 180L∕day. The advantage of this high filtration rate in terms of osmoregulation is that it allows the kidneys to rapidly and precisely regulate the volume and composition of body fluids.
At the hypothalamus level, osmoreceptor response to extracellular fluid hypertonicity, and facilitate ADH release from axons down to the posterior pituitary into the circulation. ADH serves a primary function to increase solute-free water reabsorption in the nephrons to bring down body fluid hypertonicity.
18.15.8 Pathophysiology of Electrolyte Imbalance
Due to excessive release of ADH one important disease occurs named as Syndrome of inappropriate ADH secretion (SIADH). This excessive ADH release may results from hypothalamic hyperactivity, or other sources like small-cell carcinoma. Increased ADH promotes free-water reabsorption from the filtrate, leading to an inappropriately elevated urine osmolality compared to blood plasma and by consequence, hyponatremia may develop.
In both, chronic or acute kidney disease glomerular function affected so heavily, thereby reducing the production of the filtrate. Typically, this leads to increased water retention, increased potassium retention and dilution of plasma sodium concentrations due to reduced water excretion.
Oedema is one of the consequences of kidney dysfunction. Oedema is the presence of excess fluid in either the intracellular or the extracellular fluid compartment. Extracellular oedema, may occur clinically due to acute or chronic kidney failure, mineralocorticoid excess, decreased plasma proteins or decreased hepatic synthesis of proteins.