GLOMERULAR FILTRATION RATE (GFR)
Glomerular filtration rate (GFR) is defined as the total quantity of filtrate formed by the nephrons in the given time period. Normal GFR is 125 ml/minute or about 180 L/day in human being.
GFR is determined by the balance of hydrostatic and colloid osmotic forces acting across the capillary membrane and the capillary filtration coefficient (Kf). The glomerular capillaries have a much higher rate of filtration because of a high glomerular hydrostatic pressure and a large filtration coefficient. Glomerular hydrostatic pressure is the pressure exerted by the blood in glomerular capillaries. This pressure favors glomerular filtration (60 mmHg). Colloidal osmotic Pressure is the pressure applied by plasma proteins in the glomeruli. It opposes glomerular filtration (32 mmHg). Hydrostatic pressure in Bowman capsule is the pressure exerted by the filtrate in Bowman capsule. It is also called capsular pressure and it also opposes glomerular filtration (18 mmHg)
Factors increasing GFR by vasodilatation: i. Atrial natriuretic peptide (ANP), ii. Brain natriuretic peptide (BNP), iii. Bradykinin, iv. Endothelial derived nitric oxide, v. Prostaglandin (PGE2 & PGI2)
Factors decreasing GFR by vasoconstriction: i. Angiotensin II, ii. Endothelins, iii. Noradrenaline, iv. Platelet derived growth factor (PDGF), v. Prostaglandin (PGF2).
Filtration fraction: The ratio of GFR to RPF is referred to as the filtration fraction (FF) i.e. basically the fraction of the renal plasma flow that is filtered. The FF is the fraction (or percentage) of plasma flowing through the glomerulus that becomes glomerular filtrate. Renal plasma flow (RPF) is that part of the RBF that is plasma. Filtration fraction = GFR / Renal plasma flow x 100. It is expressed in percentage.
18.14.1 Tubular Reabsorption
Tubular reabsorption is the process through which water and other important substances are transported from renal tubules to the blood. Tubular reabsorption is known as selective reabsorption because the tubular cells will reabsorb only those substances that are necessary for the body. Essential substances such as glucose, amino acids and vitamins are completely reabsorbed from renal tubule whereas the metabolic waste products are not reabsorbed and excreted through urine.
18.14.2 Routes of Reabsorption
Water and solutes can be transported either through Transcellular route: In this route the substances move through the cell (through apical or luminal surface of the cell membrane) or Paracellular route: In this route, the substances move through the intercellular space (through the tight junction between the cells) (Figure 18.6).
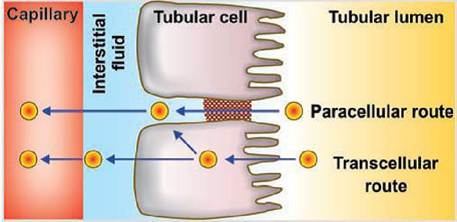
FIGURE 18.6 Route of reabsorption.
18.14.3 Mechanism of Reabsorption
Tubular reabsorption is of two types:
1. Active transport: Active transport is the movement of molecules against the electrochemical (uphill) gradient. This process needs energy which is derived from ATP. Certain substances are reabsorbed actively from the renal tubule like sodium, potassium, calcium, phosphates, bicarbonates, glucose, amino acids, ascorbic acid, uric acid, and ketone bodies.
Active transport is of two types:
Primary active transport: Transport that is coupled directly to an energy source, such as the hydrolysis of ATP. The best example of this type of transport is the sodium-potassium ATPase pump that functions throughout most parts of the renal tubule.
Secondary active transport: Transport that is coupled indirectly to an energy source, such as that due to an ion gradient, is referred to as secondary active transport. Glucose reabsorption by the renal tubule is through secondary active transport.
In secondary active transport, two or more substances interact with a specific membrane protein (carrier molecule) and are transported together across the membrane. As one of the substances diffuses down its electrochemical gradient, the energy released is used to bring another substance against its electrochemical gradient. In this way, secondary active transport does not require energy directly from ATP.2. Passive reabsorption: Passive reabsorption is the movement of molecules along the electrochemical gradient. This process does not need energy. Substances reabsorbed passively are chloride, urea, and water.
18.14.4 Co-Transport and Counter
Transport of Solute
Simultaneous transport of two or more compounds on the same carrier in the same direction (e.g., Na+ plus glucose, or Na+ plus an amino acid) is known as co-transport.
Counter-transport refers to the movement of a compound in one direction, driven by the movement of a second compound in the opposite direction (e.g., Na+-H+ countertransport).
18.14.5 Reabsorption of Important Substances
18.14.5.1 Reabsorption of Sodium
65% of sodium is reabsorbed in the PCT, the remaining 35% continuing beyond the proximal tubules. The energy requirement is derived from the Na+ZK+-ATPase located in the basal and lateral borders of the proximal tubule epithelial cells. The direction of transport is from the nephron proximal tubule to the peritubular capillaries. The reabsorption of Na+ must be accompanied by the reabsorption of anions to maintain electrical neutrality.
18.14.6 Reabsorption of Glucose
Glucose is completely reabsorbed in the proximal convoluted tubule. It is transported through the secondary active transport mechanism. Glucose and sodium bind to a common carrier protein in the luminal membrane of the tubular epithelium and enter the cell. Here the carrier protein is called sodium-dependent glucose cotransporter 2 (SGLT2) which actually helps in the transport of glucose.
From the tubular cell glucose is transported into the medullary interstitium by another carrier protein called glucose transporter 2 (GLUT2).18.14.7 Reabsorption of Amino Acids
Complete reabsorption of amino acids takes place in the proximal convoluted tubule. It is reabsorbed actively by the secondary active transport mechanism along with sodium.
18.14.8 Reabsorption of Bicarbonates
Bicarbonate is reabsorbed actively, mostly in the proximal tubule. Its reabsorption occurs in the form of carbon dioxide. In the filtrate, bicarbonate is mostly occurs in the form of sodium bicarbonate. Sodium bicarbonate dissociates into sodium and bicarbonate ions in the tubular lumen. Sodium diffuses into the tubular cell in exchange for hydrogen. Bicarbonate combines with hydrogen to form carbonic acid. Bicarbonate from the tubular fluid enters the interstitium where it combines with sodium to form sodium bicarbonate.
18.14.9 Reabsorption of Proteins and Peptides
Proteins with a molecular weight of less than 69,000 can become part of the glomerular filtrate. Because they are important nutrients, most of these proteins are reabsorbed in the proximal tubule and are not lost in the urine. However, a small quantity of protein is present in normal urine. Proteins (and polypeptides) are reabsorbed by endo- cytosis and subsequently degraded by cellular lysosomes to their constituent amino acids. The amino acids are expected to move from inside of the cell to the peritubular space by facilitated diffusion.
18.14.10 Transport Maximum (TM)
Tubular transport maximum or TM is defined as the rate at which the maximum amount of a substance is reabsorbed from the renal tubule. When the TM for the substance is exceeded in a nephron, the substance will appear in the urine. In diabetes mellitus, the movement of glucose from plasma into body cells is impaired because of the lack of insulin. Therefore, glucose concentration in the plasma increases, and hence the plasma and tubular loads of glucose increase.
In absence of a carrier molecule glucose reabsorption is hampered and the excess glucose continues its flow through the tubules into the urine. Because of the presence of glucose within the tubules, the effective osmotic pressure of the tubular fluid increases, and water remains in the tubular fluid. Thus, in diabetes mellitus, glucose can be detected in the urine and a greater volume of urine is formed. The affected animal drinks more water to compensate for the loss of urine. Not all of the hundreds of thousands of nephrons have same TM. First appearance of glucose in the urine does not represent the Tm for the kidney but rather the renal threshold. Renal threshold for glucose is defined as the plasma glucose concentration at which glucose first begins to appear in urine. The TM for the kidney is reached when all nephrons are reabsorbing to their maximum ability. In Human renal tubular filtered load is 125 mg/min whereas Tm is 375 mg/min. However renal threshold is 180 mg/dl.18.14.11 Tubular Secretion
It is the process by which the substances are secreted from blood into renal tubules.
18.14.12 Substances Secreted in Different
Segments of Renal Tubules
Potassium (K+) is secreted actively by sodium potassium pump in proximal and distal convoluted tubules and collecting ducts. Renal K+ transport is unique in that it is reabsorbed in some parts of the tubule and secreted in others. When dietary potassium intake is extremely low there is greater reabsorption of K+ in the distal nephron, and when dietary potassium intake is high there is greater K+ secretion. Ammonia is secreted in the proximal convoluted tubule. H+ secretion is primarily in distal nephron which is an active process and occurs in the intercalated cells of the collecting duct. Urea is secreted in loop of Henle.
18.14.13 Glomerulotubular Balance
This property of the proximal tubule to reabsorb a consistent fractional amount of glomerular filtrate is known as glomerulotubular balance.
The amount of filtrate reabsorbed by the proximal tubule is consistently a certain percentage of the filtrate (about 65% for water and NaCl) rather than a constant amount for each unit of time. If the GFR is low, only a fractional amount of filtrate is reabsorbed in the proximal tubule, and the remaining fraction continues to the distal nephron. If the GFR is high, the additional amount of filtrate does not continue to the distal nephron but, rather, only about one-third of it.18.14.14 Concentration of Urine
The mechanism for concentration of the tubular fluid depends on the existence of a very high osmolarity in the interstitial fluid of the renal medulla. The osmolarity increases with the distance from the cortex, reaching a maximum in the innermost aspect of the medulla The magnitude of this value varies with species, as in human it is about 1200 mOsm/L water, Dog (2400 mOsm/L water). Plasma osmolarity is about 300 mOsm/L water. The high osmolarity exists because of the countercurrent mechanism which is established by the activity of the loops of Henle and is maintained by the vasa recta
18.14.15 Countercurrent Mechanism
A countercurrent system is a system of ‘U-shaped tubules where the inflow of fluid runs parallel to, counter (opposite) to, and in close proximity to the outflow. These characteristics are common to the anatomical arrangements of the loops of Henle and the vasa recta. Thus, the countercurrent mechanism in the kidney comprises two countercurrent systems: the countercurrent multiplier (loops of Henle) and the countercurrent exchanger (vasa recta).
18.14.16 Countercurrent Multiplier System
Countercurrent multiplier system is an active process occurring in the loops of Henle, which is responsible for the production of concentrated urine. The loop of Henle uses the countercurrent multiplier system to increase the concentration of solute and ions within the medullary interstitium. These solutes accumulate in the medullary interstitium and increase the osmolarity. Because of increased osmolarity nephrons reabsorb more water and concentrate the urine. Tubular fluid entering the descending limb of loop of Henle from proximal tubule has an osmolarity of 300 mOsm/L, 280 contributed from NaCl and 20 from urea (280,20).
From the descending thin limb water diffuses outward (osmosis) and solute remain within. Tubular fluid at the hairpin turn has an osmolarity of 1200 mOsm (1120, 80). In the ascending thin limb water retained while NaCl diffuses outward and urea diffuses inward. Osmolarity decreases to 500 mOsm (400, 100) when reaches the thick segment. In the thick ascending limb and above, due to continuous outflow of NaCl outward, osmolarity decreases to about 200 mOsm (100, 100) which is hypotonic to plasma. At the end of the distal tubule, and before the fluid enters the cortical collecting duct, the osmolarity is about 150 mOsm (50, 100) (Figure 18.7).
In the cortical collecting duct, outer medullary collecting duct, and the inner medullary duct, Na+ reabsorption is stimulated by aldosterone and water & urea reabsorption is stimulated by ADH. So, at the end of the cortical collecting duct, the osmolarity is 300 mOsm (125, 175), at the end of the outer medulla it is 600 mOsm (200, 400), and before it empties into the renal pelvis it is 1200 mOsm (600, 600).
Here, the sodium and chlorine ions are repeatedly recirculated between the descending limb and ascending limb of Henle's loop through medullary interstitial fluid. In addition to that, there is regular addition of more new sodium and chlorine ions into the descending limb through constant filtration. Because of all these phenomena, there is increase or multiplication of the osmolarity of the medullary interstitial fluid and medullary gradient. Hence, it is called countercurrent multiplier.
18.14.17 Countercurrent Exchanger System
The vasa recta act as countercurrent exchangers. Vasa recta are permeable to solutes and water throughout their length. In the descending limbs, water is drawn out by osmosis from the vasa recta to the hyperosmotic peritubular fluid, and the solutes diffuse in reverse. In the ascending limbs, solutes diffuse back into the peritubular fluid, and water is drawn by osmosis back into the vasa recta. The net result is that the solutes responsible for the vertical medullary gradient are mostly retained in the peritubular fluid of the medulla.
18.14.18 Medullary Washout
An increased rate of medullary blood flow would reduce the time for diffusion of solute from the ascending limb back to the peritubular fluid; therefore, the blood leaving the ascending limb would have a higher concentration of solute. This may result in a gradual loss or washout of the medullary gradient, called medullary washout. To prevent medullary loss of solutes and to maintain the medullary gradient, the blood flow to the vasa recta is reduced and it is often sluggish. If countercurrent blood flow in the vasa recta did not exist, the solute of the renal medulla would be quickly removed instead of being retained.
18.13
More on the topic GLOMERULAR FILTRATION RATE (GFR):
- Diagnosis
- Renal Function and Hyperthyroidism
- Tubular Necrosis
- Acute Renal Failure
- FACTORS THAT INFLUENCE PHARMACOKINETIC PROFILES OF THERAPEUTIC DRUGS
- Blood Urea Nitrogen
- REFERENCES