DELAYED GASTRIC EMPTYING AND GASTRIC MOTILITY DISORDERS
Delayed gastric emptying can be caused by mechanical obstruction of gastric outflow, by functional gastric motility disorders, or by a combination of both. Causes of mechanical outflow obstruction include gastric foreign bodies, pyloric mucosal hyperplasia or muscular hypertrophy, antral polyps, neoplasia, eosinophilic granuloma, or fungal granuloma.
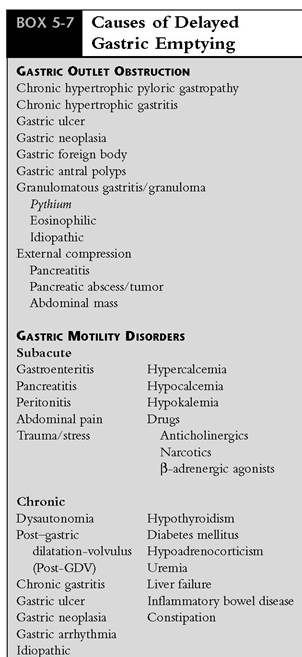
Duodenal neoplasia and pancreatic inflammation or abscess also impair gastric emptying, as will external compression on the pylorus from intraabdominal tumors.Functional gastric motility disorders occur secondary to inflammatory, infiltrative, or ulcerative disease of the upper GI tract, electrolyte imbalances (hypokalemia), metabolic diseases (hypoadrenocorticism, diabetes mellitus, uremia, hypergastrinemia), drugs (anticholinergics, β-adrenergic agonists, opiates), and peritonitis. Gastric hypomotility often occurs postoperatively, particularly following GDV or spinal injury. If delayed gastric emptying is observed in a patient with chronic vomiting and an underlying cause such as mechanical or metabolic disease is not found, a functional motility disorder should be considered as the cause of the clinical signs. Several types of motility disorders occur in the dog, including retrograde transit (duodenogastric reflux), delayed gastric emptying, and accelerated gastric emptying that infrequently occurs secondary to gastroduodenal surgery. Similar functional motility disorders have not been described in cats. Delayed gastric emptying and retrograde transit are probably caused by a functional abnormality of the gastric myenteric plexus or gastric smooth muscle and are referred to as primary or idiopathic delayed gastric emptying. Specific causes of delayed gastric emptying are listed in Box 5-7.
Clinical signs of mechanical gastric-outlet obstruction and functional gastric motility disorders are similar but vary according to the underlying cause.
Onset of signs is usually gradual, with intermittent vomiting of large amounts of partially digested food and fluid occurring several hours after eating. Vomiting progresses to a more predictable postprandial vomiting, especially if partial obstruction is present. Abrupt vomiting of nondigested food without retching will sometimes be described by the owner and incorrectly interpreted by the clinician to be regurgitation rather than vomiting. Gastric foreign bodies are an exception, usually causing acute and persistent vomiting. Postprandial abdominal distention and discomfort that are relieved by vomiting might be observed, particularly in dogs with chronic hypertrophic pyloric gastropathy. Between episodes of vomiting, most dogs will appear to be normal, with no physical or predictable laboratory abnormalities occurring unless metabolic complications such as electrolyte imbalance or dehydration occur. With time, moderate weight loss and abdominal distention may occur. If an inflammatory or neoplastic disease is the underlying cause, signs such as anorexia, weight loss, hematemesis, and melena might be observed.Diagnosis of delayed gastric emptying is made on the basis of history, physical examination, exclusion of metabolic diseases that cause chronic vomiting, and radiographic studies (Table 5-7). In general, laboratory changes caused by delayed gastric emptying are minimal and nonspecific. Anemia, often with iron deficiency, may occur with ulcerative malignancy such as gastric carcinoma. Electrolyte and acid-base imbalances are uncommon unless significant obstruction to gastric outflow has occurred, in
which instance hypochloremic alkalosis might develop. Hypokalemia can result from chronic vomiting; however,it can also be a cause of gastric hypomotility.
Survey abdominal radiographs can be normal or might reveal an enlarged stomach, depending on the cause, duration, and severity of delayed emptying.
Survey abdominal radiographs are usually normal with functional gastric motility disorders, whereas obstructive lesions often cause a fluid-filled and distended stomach. Contrast radiographs using barium sulfate liquid can be used to outline the lumen of the stomach and to subjectively evaluate gastric emptying (see Figure 5-3). Food mixed with bar-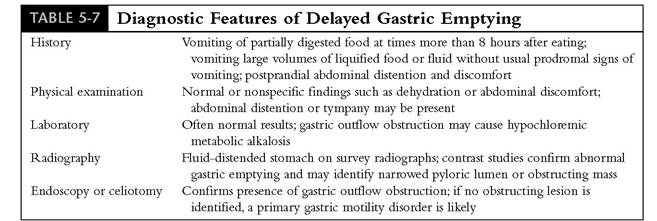
ium more accurately estimates gastric emptying time of solids. Interpretation of both types of contrast studies is subjective, and results of both can vary significantly in normal animals. Fluoroscopic examination improves accuracy of interpretation by allowing visualization of sequential changes in the shape of the stomach and pylorus and of movement of contrast through the pylorus. Liquid barium should begin to enter the duodenum within 15 minutes after administration, and gastric emptying of liquid should be complete within 1 to 4 hours. Complete gastric emptying of a barium meal should occur within 8 hours but might not be complete in some normal dogs until 15 hours after feeding. If most of the liquid barium is retained in the stomach after 4 hours, if liquid barium is present in the stomach longer than 12 hours, or if a large amount of a barium meal is retained longer than 8 to 10 hours, delayed gastric emptying is present.
An alternative method to barium studies for evaluation of gastric emptying is the use of radiopaque BIPS. BIPS are given with a canned- food meal consisting of approximately 25% of the daily caloric intake. Abdominal radiographs should then be taken at 4- to 6-hour intervals over the next 12 to 24 hours. The percentage of BIPS that have left the patient's stomach is compared with a standard curve for normal gastric emptying that is provided by the manufacturer. When radiographic gastric-emptying studies are done, it is important to remember that fear and anxiety from physical restraint often cause a transient delay of gastric emptying.
More importantly, potent anticholinergic drugs such as aminopentamide (Centrine) can delay gastric emptying for several hours. Because aminopentamide can cause profound and prolonged gastric stasis and ileus, which sometimes worsens the emesis and diarrhea that it was intended to resolve, it is not recommended for antiemetic therapy.More accurate techniques to evaluate gastric motility are limited to hospitals with nuclear medicine and GI motility laboratory facilities. Scintigraphic studies using radioactive tracers mixed with food is the method of choice for measuring gastric emptying time. Electrogastro- grams can also be done and are useful to detect abnormal patterns of gastric motility such as tachygastria and bradygastria.
Functional gastric motility disorders are characterized by delayed gastric emptying in the absence of morphologic lesions. Partial obstruction caused by restrictive or infiltrating mural diseases of the pylorus, such as muscular hypertrophy, neoplasia, or granulomatous diseases, produces annular narrowing of the pyloric canal. Barium may only fill the narrow entrance to the pylorus, resulting in a thin stream of barium often referred to as having a “beaklike” appearance (see Figure 5-3, C); this is a common finding with antral pyloric hypertrophy. Polyplike filling defects can be caused by mucosal hypertrophy, inflammatory granuloma, neoplasia, or foreign body.
Once delayed gastric emptying has been confirmed, additional diagnostic procedures such as ultrasonography, endoscopy, or exploratory surgery are necessary to determine if an obstructive lesion is present. Ultrasonography is useful to detect foreign bodies, mural thickening, and masses not detected by radiographs. Endoscopy and mucosal biopsies are useful in diagnosing chronic gastritis, IBD, neoplasia, or foreign body. Surgical examination and biopsy should be considered if the cause of delayed gastric emptying is uncertain. Full-thickness gastric biopsy allows examination of muscle and nerve plexuses not included in endoscopic pinch biopsy specimens that usually extend only into the submucosa.
Surgery provides an opportunity for resection of masses and for procedures to relieve gastric outlet obstruction.Specific Syndromes of Delayed Gastric Emptying
Antral pyloric hypertrophy syndrome, also referred to as pyloric stenosis and chronic hypertrophic pyloric gastropathy (CHPG), occurs either as a congenital condition or more frequently as an acquired disorder (Table 5-8).Young to middleage male brachycephalic breeds, particularly boxers, Boston terriers, Lhasa apsos, and Maltese, Pekingese, and shih tzu dogs, are most commonly affected. Clinical and radiographic signs of delayed gastric emptying with intermittent gastric dilatation and episodes of projectile vomiting are often observed. Physical examination and laboratory findings are usually normal. Contrast radiographs often reveal a distended stomach with delayed gastric emptying of contrast material and an abrupt narrowing of the pyloric canal with only a narrow stream of barium passing through (see Figure 5-3, C). Endoscopic examination usually reveals a thickened pyloric mucosa that sometimes appears as a protuberant mass, often with mucosal erosions (see Figure 5-3, D). Histologically the mucosa is thickened with edema and hyperplasia, and the muscu- laris is usually hypertrophied.
Treatment requires pyloroplasty with submucosal resection to remove thickened mucosal folds to reestablish gastric outflow. Y-U antral advancement flap pyloroplasty is the most effective method of reestablishing gastric outflow while preserving normal pyloric function. Prognosis is generally good following pyloroplasty, although some patients require a feeding schedule of small frequent meals and treatment with metoclopramide to enhance gastric emptying.
Primary Gastric Motility Disorders
Delayed gastric emptying can be caused by abnormally slow gastric contraction (bradygastria), rapid rhythm (tachygastria), or irregular rhythm (dysrhythmia), conditions thought to be caused by abnormal gastric pacemaker activity.
Brady- gastria causes infrequent gastric contraction, whereas tachygastria can cause reversed propagation of motor activity, which prevents normal emptying. Gastric dysrhythmias have been observed to occur normally in healthy dogs during fasting, whereas feeding will abolish the dysrhythmia. Animals symptomatic for gastric dysrhythmias are presented for signs of post prandial abdominal discomfort, bloating, or chronic vomiting. Diagnosis requires documentation of gastric retention and elimination of obstructive and metabolic causes of delayed gastric emptying (Figure 5-8; see color plate). Measurement of gastric electrical activity is diagnostic but is limited to referral institutions.Treatment relies on a combination of dietary changes and prokinetic drugs to improve gastric emptying (Box 5-8). Surgical procedures are generally not successful to improve gastric emptying for patients with primary functional gastric motility disorders. Liquified or blenderized diets are useful to try because liquids empty from the stomach more rapidly than solids. Because fats and proteins delay gastric emptying, diets low in fat and protein and high in carbohydrates should be tried
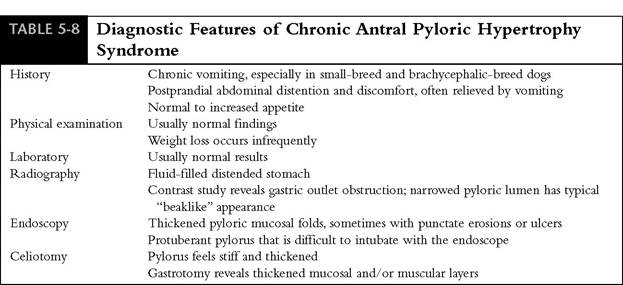

Figure 5-8 Gastric retention of food particles and bile-colored fluid in a 12-year-old miniature poodle with clinical signs of intermittent vomiting, regurgitation, inappetence, and bloating. The dog had no food or water for 14 hours before endoscopy. Results of gastric mucosal biopsies were normal, and the dog was diagnosed with primary (idiopathic) gastric motility disorder. Clinical signs improved, but did not resolve, when the dog was treated with cisapride and dietary management (small meals, fat- restricted food). (See color plate.)
initially for patients with suspected functionally delayed gastric emptying. If dietary changes are unsuccessful, gastric prokinetic drugs should be added to the therapeutic plan.
Different prokinetic drugs have different modes of action and therefore have different effects on gastric, pyloric, and duodenal contractions. For that reason, whether a particular drug is effective in improving motility depends on both the specific effects of that drug and how the underlying abnormality is affecting gastric motility. In general, cisapride has been considered to be the most effective prokinetic drug because it accelerates gastric emptying in dogs by stimulating both pyloric and duodenal motor activity, by improving coordination among antral, pyloric, and duodenal contractions, and by increasing propagation distance of duodenal contractions. The result is a predictable promotility effect, particularly in the upper GI tract, with no significant adverse effects being reported in dogs or cats. Because of the uncertain availability of cisapride, other drugs, including metoclopramide, erythromycin, and ranitidine, are alternatives to consider for treatment of delayed gastric emptying. Metoclopramide is not as effective as cisapride in accelerating gastric emptying. However, it does enhance coordination of gastro- pyloroduodenal contractions to improve gastric emptying of liquids and to prevent gastric stasis and enterogastric reflux. Metoclopramide also inhibits dopaminergic D2 receptors in the CRTZ to diminish central stimulation of nausea and vomiting that can occur from delayed gastric emptying. Another alternative is erythromycin, which at low dosages will induce antral contractions and accelerate gastric emptying of solids. The contractions stimulated by erythromycin are similar to those that normally occur in the fasting state to empty the stomach of nondigestible solids. As a result, treatment with erythromycin might result in larger than normal and less-digested food particles being expelled into the duodenum, which could possibly cause worsening of the GI signs. The H2-receptor antagonists ranitidine and nizatidine are
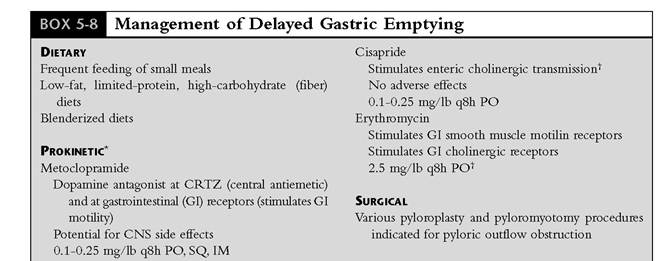
CRTZ, Chemoreceptor trigger zone; CNS, central nervous system; PO, orally; SQ, subcutaneously; IM, intramuscularly.
[*]Contraindicated in gastric outlet obstruction.
1"May be more effective than metoclopramide to enhance gastric emptying of solids.
used primarily to inhibit gastric acid secretion. These drugs also stimulate GI motility by inhibiting acetylcholinesterase activity, thereby increasing the amount of acetylcholine available to bind to smooth muscle muscarinic receptors. The result is primarily stimulation of gastric emptying, with some increase in small intestinal and colonic motility.
The choice of which prokinetic drug to use first depends in part on whether an underlying cause has been identified. For example, ranitidine and nizatidine are useful in the treatment of gastric motility disorders associated with gastric ulcerative or inflammatory diseases where both acid suppression and stimulation of gastric emptying are beneficial. Metabolic causes of delayed gastric emptying such as uremia or diabetic ketoacidosis, where central stimulation of vomiting might also occur, and gastric hypomotility following surgery for GDV tend to respond well to treatment with metoclopramide. If an underlying abnormality cannot be identified, the choice of treatment is trial and error. In general, cisapride (if available) should be tried initially, with erythromycin being a second choice. Metoclopramide and ranitidine or nizatidine are considered if inadequate response is achieved with the initial treatment.
Clinical experience indicates that several days of treatment are often required before a clinical response is observed. Some patients with functional dysrhythmias that respond to prokinetic drugs may require treatment indefinitely, perhaps at lower or less frequent dosing than the standard recommendations, whereas other patients might eventually be weaned off therapy. To determine if a lower drug dose is adequate requires individualized treatment for each patient. A suggested protocol is to first decrease the frequency of dosing (e.g., if a drug is being given three times a day, decrease to two times a day; if being given two times a day, decrease to every day). If clinical signs are adequately controlled for several days, alternate-day treatment can then be tried. If signs are still controlled, discontinuing the drug should be considered. If the signs reoccur, treatment must be resumed, and the lowest possible effective dose is used on a longer-term basis.