Colonoileoscopy
1.5.5.1 Preparation and anesthesia
Food should be withheld for at least 24 and preferably 36 hours before the procedure. The colon must be cleaned thoroughly, which can be achieved by use of gastrointestinal lavage solutions (e.
g., Colyte®, Schwarz Pharma, Milwaukee, WI) and /or enemas.8 Enemas are easier and less expensive, but it is crucial to perform several enemas before the procedure. Properly performed enemas consist of administering copious amounts of warm water (no soap) with the enema tube inserted as far into the colon as possible. At least one liter of warm water is administered per enema to dogs weighing more than 10 kg. For large breeds (e.g., >30 kg) 2 liters per enema can be used. Water often starts exiting the anus before the enema is finished, but the full amount should be administered. Three to four such enemas should be given the night before the procedure and 1-2 more the next morning, at least 2-3 hours before the procedure. Administering bisacodyl (5 mg) the night before the procedure also can be useful. The colon in cats is particularly hard to clean with enemas. Also, one must avoid over distension of the colon with the enema, which could result in vomiting. Cats usually receive 50-60 ml of warm water via a soft latex catheter and a syringe.Lavage solutions are more effective for cleaning the colon than enemas alone.4,9 These solutions are especially useful in large patients (i. e., >30 kg) or in patients with rectal pain. A volume of 25-30 ml/kg of the lavage solution is administered twice, at least 2 hours apart, the night before the procedure. Another dose of the solution is usually administered again the morning of the procedure. An enema will then be administered to wash out the lavage solution. Very rarely, gastric dilation and volvulus occurs after administering such large volumes of lavage solution.
Almost any anesthetic regime may be used for colonoscopy. Severely ill patients may only need sedation or manual restraint, unless ileoscopy is also planned. Ileal biopsies typically require anesthesia, and one should avoid drugs like oxymorphone and fentanyl.
1.5.5.2 Technique4
1 Flexible colonoscopy is simple to perform compared to gastroduodenoscopy, and rigid colonoscopy is very easy. A digital rectal examination should always be performed immediately before either endoscopy to detect potential problems (e.g., perineal hernia or a mass) and help straighten out the rectal canal so as to make entry into the colon easier. For rigid colonoscopy, the patient is positioned in right lateral recumbency so that any fluid present in the colon will pool in the ascending and transverse colon.8 The tip of the colonoscope is inserted about 3 cm into the rectum with the obturator in place. Then, the obturator is removed, the glass window closed, and air is insufflated into the colon. As the colonic lumen opens up, the operator can follow the lumen orad until the entire length of the scope is inserted or the descending colon turns and becomes the transverse colon. Rigid colonic biopsy forceps provide tissue samples that are far superior to those that can be obtained by use of flexible biopsy forceps. However, rigid colonoscopy is limited to the descending colon. Fortunately, most, but not all, diffuse colonic lesions involve the descending colon.
If the entire colon is to be examined, flexible colonoscopy is required. The patient is positioned in left lateral recumbency, which prevents other abdominal organs from pushing down on the ileocolic valve area. The endoscope is advanced along the lumen until the ileocolic valve is seen. If the colon will not distend because air is escaping from the rectum, an assistant can hold the rectum tightly against the endoscope, thus trapping the air.
The ileocolic valve region is often not as a clean as the rest of the colon because of ingesta continually exiting the small bowel and entering the colon.
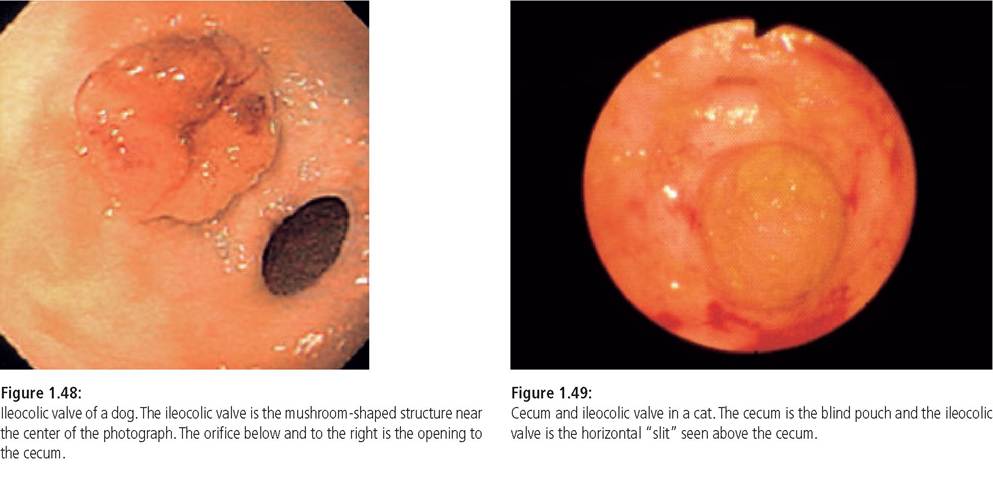
In the dog, it is easy to bypass the ileocolic valve obscured with ingesta and inadvertently pass the endoscope tip into the cecum, thinking that the endoscope is still in the colonic lumen. If the colon appears to be making a spiral curve and the scope cannot be further advanced, the scope should be withdrawn as the operator carefully looks for the ileocolic valve that was previously missed.The ileocolic valve is a dynamic structure in the dog. It can appear as a “mushroom” with a slit in the center (Figure 1.48), it can retract and look like an opening in the colonic wall, or it can appear anywhere in between these two extremes.4 The feline ileocolic valve region is different. The cecum is simply a blind sac, and the ileocolic valve is usually a slit opening in the mucosa (Figure 1.49). This region is seen immediately after the tip of the scope negotiates the flexure between the descending colon and the ascending / transverse colon. In some cases, the tip of the scope will pass the ileocolic valve and the scope will have to be partially withdrawn in order to see the valve.
In dogs weighing >7 kg, one can typically enter the ileum with an endoscope that has an outer diameter of a more “gummy” or "jello-pudding"-like texture.
piece of tissue (as opposed to the non-distinct material that characterizes samples primarily composed of villus tips) that can be unfolded and handled (Figure 1.51), and c) it fills the cup of the biopsy instrument.14 Pushing the biopsy forceps into the mucosa at as near to a 90° angle as possible (as opposed to a more acute angle) is desirable.13 One technique, known as the “turn and suction” technique involves inserting the biopsy instrument until the jaws extend several millime-

Figure 1.52:
Biopsy site.
Endoscopic view of a site where a biopsy has been taken. Note the white submucosal tissue showing that a full thickness section of mucosa was obtained.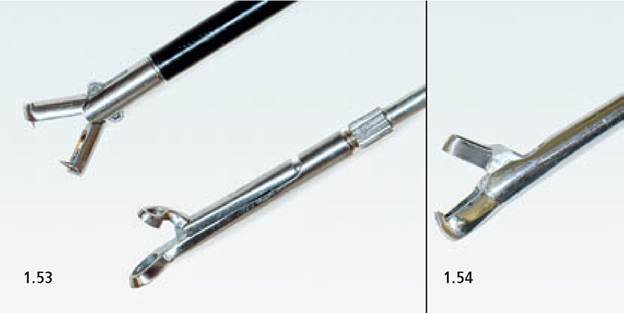
Figure 1.53:
Biopsy forceps. The top one is a “double spoon” forceps, which is preferred for laparoscopic liver biopsies. The lower one has a smaller punch that fits into the lower cup much like a pair of scissors, which is preferred for biopsy of colonic mucosa.
Figure 1.54:
Biopsy forceps. Heavy duty rigid forceps that will be able to cut through very dense, infiltrative lesions.
ters in front of the scope tip.10 Then the biopsy instrument jaws are opened and the forceps are gently withdrawn until the opened jaws are resting against the tip of the scope. Now, the tip of the scope is maximally deflected up or down, whichever makes the tip of the scope as near perpendicular to the mucosa as possible. This will produce a “red out” (i. e., the scope tip rests against the mucosa causing the endoscopist to see a red blur). Next, suction is applied and then the biopsy instrument is advanced into the mucosa for 2-4 mm. The biopsy instrument is closed when there is substantial resistance to advancing the tip. The scope is straightened in order to avoid damaging the biopsy channel, and the forceps are withdrawn. Sometimes one may look at the mucosa after performing an excellent biopsy and see obvious, whitish submucosa, which indicates that a full-thickness mucosal biopsy was obtained (Figure 1.52). Another technique is the “push-off” technique, which is, however, not described here.10 If the duodenum cannot be entered, one may blindly pass the biopsy forceps through the pylorus to biopsy duodenal mucosa. However, such biopsies typically yield non-diagnostic, artifact-riddled tissue samples. At least eight excellent tissue samples from the duodenum, should be collected in the hope that one or two of them will be oriented in an optimal fashion for evaluation by the pathologist.15
For flexible endoscopic biopsy of the colon and ileum, the same technique is employed.
If a rigid scope is used, one can obtain a tissue sample superior to anything that a flexible scopecan provide. A fold of colonic mucosa is created by gently moving the endoscope back and forth a little, and then the edge of this fold is cut off using rigid forceps.8 The best biopsy forceps for collecting colonic mucosal biopsies are those where the small upper punch fits into a larger lower cup and cuts the tissue much like a pair of scissors rather than the “double spoon” type (Figure 1.53).
For rectal lesions with a dense submucosal infiltrate (e.g., scirrhous carcinomas), it is imperative to biopsy the underlying submucosa and not just the overlying mucosa. In order to collect these tissue samples, heavy, rigid forceps with the shearing action described above are necessary (Figure 1.54). It can be very difficult to sample a densely infiltrated submucosa and it sometimes works best if the scope is removed from the anus, and a gloved finger guides the forceps to the thickest part of the lesion. The opened jaws of the forceps are carefully placed over the thickest part, pushed firmly into the lesion, and forcefully closed. This often results in an audible “crack” as the dense underlying tissue is cut.8 The tissue must be inspected after removal from the forceps. If the presence of submucosa is not obvious the biopsy must be repeated.

Figure 1.55:
Biopsy handling. Example of how tissue samples should be placed on a sponge or other media prior to fixation. Note how the biopsies have been gently unfolded after they were taken from the biopsy forceps.
1.5.7.2 Mounting and handling tissue samples
It is critical that the clinician consults with the pathologist to establish how the samples are to be submitted, and how the lab will process the samples. In particular, duodenal samples are very difficult to get embedded correctly, but are often the samples most likely to provide valuable information.
The author places tissue samples on a non-absorbent, plastic sponge that fits into the histopath cassette.14,15 Duodenal and ileal samples are oriented such that the submucosal side of the sample is on the sponge and the villi are pointing away from the sponge (Figure 1.55). It is crucial to not allow the tissue samples to dry out. The sponges with the attached tissue samples are placed upside down in formalin and submitted to the laboratory. The laboratory embeds these samples in paraffin by turning them 90 degrees so that they will be sectioned longitudinally. This should enable the pathologist to see a well-oriented section of mucosa from the villus tips to the junction of the mucosa and muscularis mucosa (Figure 1.56). For gastric and colonic mucosal samples, it does not matter which side is against the sponge. However, care must be taken not to stretch colonic or gastric mucosa when placing it on the sponge.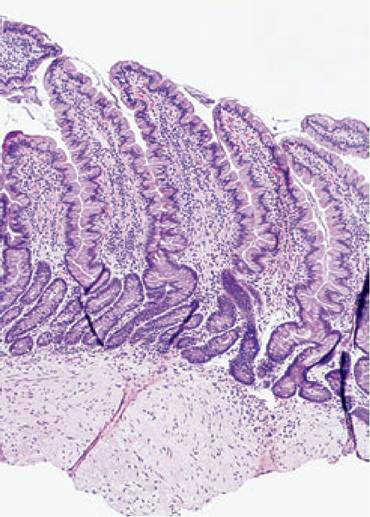
Figure 1.56:
Duodenal mucosa. A photomicrograph of a good-quality, well-oriented section of duodenal mucosa. Note that the entire thickness of the mucosa can be seen and that some submucosa is included. Not all endoscopic biopsies are as high-quality as the one shown, but it should be the aim of the clinician and pathologist that at least some samples from every case are oriented this well.

Figure 1.57:
Duodenal papilla. Endoscopic view of a duodenum showing the duodenal papilla at the 9-o'clock position. (From: Fossum T (ed.) Small Animal Surgery, 2nd ed. 2002, page 113; used with permission.)

Figure 1.58:
Lymphoid follicle. Endoscopic view of a duodenum showing a crater-like depression at the 5-o'clock position, which represents a normal lymphoid follicle.

Figure 1.59:
Submucosal leiomyoma in a dog. (From: Nelson R, Couto G (eds.), Small Animal Internal Medicine, 3rd ed. 2003, page 416; used with permission.)
1.5.6