Azoles
Overall, the azoles are the most widely used class of antifungal drugs in humans (Lass-Florl 2011) and in animals for the treatment and prophylaxis against deep fungal infections.
Azoles are cyclic organic molecules characterized by a core five- member azole ring, which can be divided into two groups based on the number of nitrogen atoms in the azole ring. These are the imidazoles and triazoles, which contain two and three nitrogen atoms, respectively, within the azole ring (Maertens 2004).Ketoconazole belongs to the imidazoles (Maertens 2004), whereas fluconazole, itraconazole, voriconazole, posaconazole, and isavuconazole are prominent triazoles. The chemical structures of azoles used for systemic antifungal therapy are shown in Fig. 16.4. The azoles inhibit the synthesis of ergosterol from lanosterol in the fungal cell membrane by binding of the free nitrogen atom of the azole ring to the iron atom of the heme group of a fungal enzyme (Groll et al. 2003; Mohr et al. 2008). Their target enzyme is the cytochrome P450 CYP-dependent 14-α-demethylase (CYP51 or Erg11p), which catalyzes the targeted synthetic reaction. The inhibition depletes ergosterol, and methylated sterols accumulate in the cell
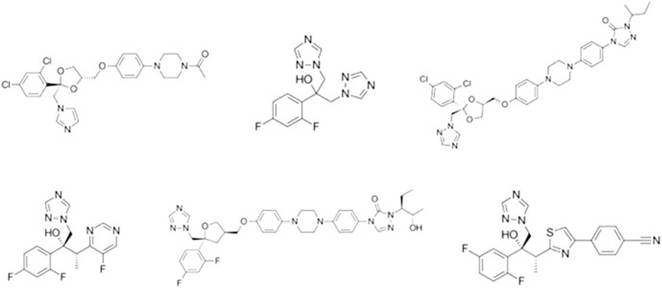
Fig. 16.4 Chemical structures of ketoconazole (top-left), fluconazole (top-middle), itraconazole (top-right), voriconazole (bottom-left), posaconazole (bottom-middle), and isavuconazole (bottomright)
membrane, which either inhibits growth or induces death of the fungal cells, depending on the species and antifungal compound involved. Of note, the triazoles have different affinities for the CYP-dependent 14-α-demethylase, which results in variable susceptibilities of different fungi, side effects, and drug-drug interactions (Warrilow et al.
2010).16.2.2.1 Imidazoles
Ketoconazole
Ketoconazole is a member of the class of imidazole antifungals and is structurally similar to clotrimazole and miconazole. Released in the early 1980s, it was the first broad-spectrum oral antifungal treatment for systemic and superficial fungal infections (Maertens 2004). Prior to the introduction of the triazoles, ketoconazole was regarded as the standard and only available oral agent for the treatment of chronic mucocutaneous candidiasis for over a decade, and an effective alternative to amphotericin B in less severe (non-immunocompromised) cases of blastomycosis, histoplasmosis, paracoccidioidomycosis, and coccidioidomycosis in humans (Maertens 2004; Gupta and Lyons 2015). However, within the first few years of its approval, numerous clinically relevant shortcomings of this compound became evident such as hepatotoxicity, several drug interactions, considerable interindividual variation influenced by gastric pH, and poor penetration of the blood-brain barrier, which rendered it ineffective and unsuitable for the treatment of fungal meningitis. In addition, ketoconazole is largely fungistatic and has been proved to be less effective in immunocompromised patients (Maertens 2004; Gupta and Lyons 2015). Due to its significant side effects, the use of ketoconazole in humans is now largely reserved for topical administration for fungal and seborrheic dermatitis. However, systemic ketoconazole may be indicated for the treatment of endemic mycoses (blastomycosis, coccidioidomycosis, histoplasmosis, chromomycosis, and paracoccidioidomycosis) where alternatives are not available or feasible (Gupta and Lyons 2015).
Ketoconazole is licensed for dogs only in some European countries. In dogs and cats, ketoconazole has been used successfully to treat systemic mycoses, including blastomycosis (Arceneaux et al. 1998), histoplasmosis (Clinkenbeard et al. 1988), cryptococcosis (O'Brien et al. 2006), dermatophytosis (De Keyser and Van den Brande 1983), systemic coccidioidomycosis (Hinsch 1988), and sporotrichosis (Nakamura and Saato 1995) and Malassezia dermatitis (Godfrey 1998; Foy and Trepanier 2010).
However, its successful response rate is lower than itraconazole and fluconazole (Hodges et al. 1994; Legendre et al. 1996). As in humans, the topical ketoconazole formulations (shampoo, cream, ointment) can be used for treatment of dermatophytosis and Malassezia infection in animals. A review indicated that ketoconazole was effective to treat Malassezia dermatitis at both 5 and 10 mg/kg per day for 3 weeks (Negre et al. 2009). Ketoconazole use is contraindicated in pregnant animals (Frymus et al. 2013). Topical ketoconazole formulations are also used in cats (Willard et al. 1986). However, most of the dermatophytosis cases in cats require a systemic treatment (Rochette et al. 2003).Parconazole
Parconazole is another systemic fungicide belonging to the imidazole group, with a broad spectrum against yeasts dermatophytes, and other filamentous fungi. It is a registered veterinary drug in poultry and birds breeding in many countries. Parconazole is used in veterinary medicine as an oral fungicide against candidiasis in guinea fowls. As a medicated feed, it is recommended at a concentration of 30 mg/ kg for prophylaxis and 60 mg/kg as a therapeutic dose for 7-10 days (EMA 1998).
16.2.2.2 Triazoles
The poor response rates and frequent recurrences of major fungal infections as well as the toxicity associated with ketoconazole therapy led to the development of a second group of azole derivatives, namely, the triazoles (Maertens 2004). In humans, five triazole compounds (fluconazole, itraconazole, voriconazole, posaconazole, and isavuconazole) have been clinically approved and are currently widely used for the prevention and treatment of several life-threatening fungal diseases (EMA 2012a, b). The triazoles have different affinities for the CYP-dependent 14-α-demethylase, which in turn results in variability on the susceptibilities of fungi, side effects, and drug-drug interactions (Warrilow et al. 2010).
Fluconazole
Fluconazole exhibits antifungal activity against most common clinical isolates of Candida and Cryptococcus spp.
and the endemic dimorphic fungi B. dermatitidis, Coccidioides spp., H. capsulatum, and P. brasiliensis. However, fluconazole lacks efficacy against molds such as Aspergillus spp., and, therefore, it is not suitable for targeted prophylaxis or treatment of aspergillosis (EMA 2012c). Typically, Candida glabrata, Microsporum, and Malassezia species are inherently less susceptible to fluconazole, while C. krusei is considered to be intrinsically resistant to this triazole (Odds et al. 1986).Fluconazole is available both in oral and intravenous formulations, with excellent bioavailability following oral administration (~90%) in humans (Brammer et al. 1990). It is also reported to be completely absorbed following administration to dogs (Humphrey et al. 1985). Fluconazole is cleared primarily by the kidneys, with greater than 70% of the dose eliminated unchanged in the urine in humans and various animal species (Humphrey et al. 1985; Diflucan 2013). The pharmacokinetics of fluconazole is similar in dogs and cats, and this triazole penetrates well into various fluids, including cerebrospinal fluid, aqueous humor, and bronchial epithelial fluid (Humphrey et al. 1985; Vaden et al. 1997; Diflucan 2013). Overall, fluconazole is very well-tolerated with few significant adverse effects, such as nausea, vomiting, and headache (Diflucan 2013). Increases in hepatic enzymes can occur with administration, but this is a class effect of the azoles, and hepatic failure is rare. Drug interactions can also occur with fluconazole due to its potent inhibition of CYP2C9 and moderate inhibition of CYP3A4 (Diflucan 2013).
In humans, fluconazole is approved for the treatment of vaginal, oropharyngeal, and esophageal candidiasis, as well as systemic Candida infections, fungal infections of the urinary tract, peritonitis, cryptococcal meningitis, and prophylaxis of patients undergoing bone marrow transplantation (Diaz et al. 1992; Pappas et al. 1995). Previous studies have shown that high doses of fluconazole (≥4-8 mg/kg per week) applied for long durations (12-16 weeks) are required for treating tinea capitis regardless of the fungus causing the infection (Shemer et al.
2013).Fluconazole shows a predictable pharmacokinetics in animals and does not require therapeutic drug monitoring (Latimer et al. 2001). However, due to its teratogenic potential, fluconazole should be avoided during gestation (Pursley et al. 1996). Fluconazole has been recommended for veterinary patients with systemic mycoses affecting the central nervous system or eyes. Fluconazole pharmacokinetics following intravenous and oral administration suggests that a dosage of 5-10 mg/kg per day in dogs and a dosage of 50 mg per cat per day exceed minimum inhibitory concentrations for most pathogenic fungi (Vaden et al. 1997). It has been used successfully in dogs and cats with cryptococcosis (Malik et al. 1992; O'Brien et al. 2006) and blastomycosis (Arceneaux et al. 1998). Fluconazole at oral doses of 2.5-5 mg/kg appears to be effective for treatment of canine nasal aspergillosis; however the success outcome was much lower compared with topical enilconazole (Sharpetal. 1991).
Itraconazole
Itraconazole is another first-generation triazole antifungal. It is a strongly hydrophobic and water-insoluble compound with a high molecular weight, is highly proteinbound (>99%), and is structurally similar to ketoconazole (Fig. 16.4). The spectrum of activity of itraconazole is increased compared to that of fluconazole, in that it does have activity against certain molds, including Aspergillus species and some members of the order Mucorales, as well as B. Bermatitidis, Coccidioides spp., and H. capsulatum. Itraconazole is also active against Sporothrix species, although this may be variable (Kohler et al. 2004). Variable activity has also been reported against some species within the order Mucorales. Resistance may develop in Candida species, which has also been documented in Aspergillus species, including A. fumigatus (Seyedmousavi et al. 2014a; Verweij et al. 2016).
In the USA, itraconazole is only available in formulations for oral administration. In humans, this includes capsules and an oral solution.
Unfortunately, the bioavailability following administration of these formulations can be variable in both humans and animals (Van Cauteren et al. 1987; Boothe et al. 1997), with various factors influencing the amount that is absorbed. For the capsule, the use of medications that increase the gastric pH, such as antacids, H2 antagonists, and proton pump inhibitors, may significantly reduce the bioavailability due to the need for an acidic pH for solubility (Denning et al. 1994; Glasmacher et al. 1998; Kageyama et al. 1999). Although less affected by gastric pH since itraconazole is already dissolved, the oral solution is associated with significant gastrointestinal adverse effects, including nausea, vomiting, and diarrhea. The osmotic diarrhea that occurs with the oral solution is due to the cyclodextrin component, which is used to keep itraconazole in solution but is not absorbed following oral administration (Sporanox 2017). Compounded formulations of itraconazole have been used in animals but showed variable pharmacokinetics compared to the clinically available capsule and oral solution formulations (Smith et al. 2010). Following administration, itraconazole is eliminated by hepatic metabolism. In humans and in some animals, including dogs, it is metabolized to hydroxy-itraconazole, a bioactive metabolite with in vitro activity similar to that of the parent drug (Odds and Bossche 2000). However, not all animals metabolize itraconazole to hydroxy-itraconazole. Because it accumulates in various tissues, including the stratum corneum, and has a relatively long half-life, alternative dosing strategies have been utilized in cats for the treatment of cutaneous infections (Pinchbeck et al. 2002). However, the half-life may differ considerably between different animal species (Van Cauteren et al. 1987; Reidarson et al. 1998; Pinchbeck et al. 2002; Manire et al. 2003). As with all azoles, increases in hepatic enzymes may be observed with itraconazole use. Interestingly, itraconazole may have a negative inotropic effect. Because of the potential to result in congestive heart failure in patients with impaired ventricular function, itraconazole carries this as a black box warning in humans (Sporanox 2017). Itraconazole is also associated with significant drug interactions due to inhibition of CYP3A4 as well as p-glycoprotein (Sporanox 2017).Itraconazole was the first extended spectrum triazole to become available for clinical use in humans. It is commonly used for the treatment of chronic and allergic fungal infection and for the empiric therapy of patients with febrile neutropenia who have suspected fungal infections (Lass-Florl 2011). In addition, it is used for the treatment of pulmonary and extrapulmonary blastomycosis, chronic cavitary pulmonary and disseminated non-meningeal histoplasmosis, and pulmonary and extrapulmonary aspergillosis in patients who are intolerant or refractory to amphotericin B therapy (Lass-Florl 2011). Itraconazole also remains the preferred azole for use in human patients to treat non-life-threatening systemic mycoses that do not involve the central nervous system (Lass-Florl 2011). Itraconazole is effective against both Microsporum and Trichophyton species and offers an alternative to griseofulvin for the treatment of kerion and noninflammatory tinea capitis (Schauder 2002).
Though relatively expensive for veterinary use, itraconazole has been used extensively in different animals with systemic fungal infections (Boothe et al. 1997; Miller et al. 2002; Pinchbeck et al. 2002; Manire et al. 2003; Bunting et al. 2009). In dogs, itraconazole is effective against blastomycosis, histoplasmosis, cryptococcosis, and coccidioidomycosis (Hodges et al. 1994; Legendre et al. 1996; Jacobs et al. 1997; Arceneaux et al. 1998; Graupmann-Kuzma et al. 2008). Oral itraconazole is also effective for treatment of dermatophytosis, sporotrichosis, Malassezia dermatitis, and otitis in dogs (Sykes et al. 2001; Pinchbeck et al. 2002).
Itraconazole is currently the preferred drug in feline dermatophytosis and is licensed for this indication in many countries. It is comparable (or superior) in efficacy to ketoconazole or griseofulvin and is much better tolerated by cats (Frymus et al. 2013). In horses, long-term treatment with itraconazole appears to be effective in the treatment of nasal aspergillosis (Korenek et al. 1994) and coccidioidomycosis (Foley and Legendre 1992). Itraconazole has been also used in a variety of raptors, psittacines, and waterfowl as first choice for treatment of aspergillosis, and no toxicity has been reported in birds (Orosz and Frazier 1995).
Voriconazole
Voriconazole is a low molecular weight water-soluble triazole, which is structurally similar to fluconazole. Because of its potent in vitro and in vivo efficacy against Aspergillus species (EMA 2012a), voriconazole is considered the drug of choice for the treatment of invasive aspergillosis in humans, and it is also used for this purpose in animals, including dogs, cats, penguins, falcons, and marine mammals, which may be highly susceptible to Aspergillus infections (Herbrecht et al. 2002; Di Somma et al. 2007; Taylor et al. 2014; Hyatt et al. 2015; Patterson et al. 2016). Voriconazole also has potent in vitro activity against yeasts, including C. krusei, Cryptococcus species, endemic fungi (B. dermatitidis, Coccidioides species, H. capsulatum), as well as different molds, including some Scedosporium (e.g., S. apiospermum and S. boydii) and Fusarium species (Lackner et al. 2012). However, voriconazole lacks activity against the Mucorales (Lewis et al. 2011; Sun and Singh 2011) and has reduced to no activity against certain species of Scedosporium (e.g., S. aurantiacum, Lomentospora (formerly Scedosporium) prolificans) and Fusarium (e.g., F. solani) (Alastruey-Izquierdo et al. 2008; Tortorano et al. 2008; Lackner et al. 2012, 2014).
Both oral and intravenous formulations are available for administration, and in humans oral dosing is recommended to be done on an empty stomach, which is not always feasible when administering to different animal species. Once administered, voriconazole is primarily eliminated via hepatic metabolism by the cytochrome P450 isoenzymes 2C19, 2C9, and 3A4. In human adults, the metabolism may be saturable resulting in disproportional increases in concentrations with small increases in the dose due to nonlinear pharmacokinetics (Lazarus et al. 2002; Walsh et al. 2004). In rodents, voriconazole may induce its own metabolism resulting in low or undetectable concentrations (Roffey et al. 2003), and this may also occur in some bird species (Flammer et al. 2008; Beernaert et al. 2009b). The variability in voriconazole concentrations may be due to numerous factors, including drug-drug interactions, drug-disease interactions (e.g., vomiting, diarrhea, mucositis), as well as CYP2C19 polymorphisms (Matsumoto et al. 2009). Because of this, therapeutic drug monitoring is often performed. The therapeutic window for voriconazole is narrow, with trough levels of at least 1 mg/L needed for efficacy (Smith et al. 2006; Pascual et al. 2008), while higher concentrations (≥ 5.5 mg/L) may result in concentrationdependent toxicities, which have been reported in humans and animals (Imhof et al. 2006; Pascual et al. 2008; Troke et al. 2011; Pascual et al. 2012; Hyatt et al. 2015).
Increases in hepatic enzymes can also occur with voriconazole. There is some debate as to whether increases in hepatic enzymes may or may not be concentrationdependent (Denning et al. 2002; Tan et al. 2006). However, it has been shown in humans and some animal species that central nervous system toxicities, including encephalopathy, are indeed concentration-dependent (Imhof et al. 2006; Pascual et al. 2008; Hyatt et al. 2015). Other toxicities that have been reported with voriconazole include visual abnormalities, alopecia, phototoxicity, and periostitis (Malani et al. 2014; Moon et al. 2014; Williams et al. 2014). Voriconazole is also associated with significant drug interactions, as it is a substrate and inhibitor of CYP 2C19, 2C9, and 3A4.
Clinical reports of voriconazole use in animals are sparse and limited primarily to cases with systemic aspergillosis and other difficult-to-treat fungal infections. In dogs, voriconazole undergoes extensive metabolism; it also induces its own metabolism over time (Roffey et al. 2003). Voriconazole is recommended drug of choice for invasive aspergillosis in dogs and cats because of its fungicidal activity and its safety as compared with amphotericin B. Voriconazole also has been used in birds to control aspergillosis. In some species of wild and captive-held falcons and quails, it appears to be effective and safe for the treatment of aspergillosis (Di Somma et al. 2007; Tell et al. 2010; Gentry et al. 2014). Voriconazole has also been used with success to treat disseminated scedosporiosis in dogs (Taylor et al. 2014).
Topical administration of voriconazole can be used successfully to treat dematiaceous fungal keratitis in dogs (Pucket et al. 2012). Treatment with topical 1% voriconazole solution was successful in resolving Aspergillus flavus keratomycosis (Labelle et al. 2009). Intracorneal administration of 5% voriconazole solution also resulted in resolution of clinical disease, specifically stromal abscessation and secondary uveitis (Smith et al. 2014).
Posaconazole
Posaconazole is a lipophilic triazole, which is structurally similar to itraconazole. Posaconazole is distinguished from the other azoles by its potent in vitro activity against the Mucorales, which show reduced susceptibility to other triazoles, and improved activity against Aspergillus spp. compared to itraconazole (Manavathu et al. 2000).
Posaconazole is currently available in oral and intravenous formulations for humans. The oral formulations include a suspension and a tablet. The oral suspension should be administered with a high-fat meal and multiple times per day due to saturable absorption. The bioavailability of this formulation is limited by several factors, including the concomitant use of agents affecting gastric pH and gastric motility, as well as vomiting, diarrhea, and mucositis (Krishna et al. 2009). Due to significant variability in bioavailability with the oral suspension and a higher percentage of patients having low or undetectable concentrations, a delayed-release tablet was developed that prevents the release of the drug in the low pH environment of the stomach but allows its release in the small intestine where absorption is maximized (Krishna et al. 2012; Kersemaekers et al. 2015). Unfortunately, the delayed-release tablet cannot be crushed so that the dose can be adjusted, and there is limited experience with the use of this formulation in animals.
Posaconazole appears to be well-tolerated in humans, although there are some reports of adverse effects associated with elevated posaconazole concentrations (Martino et al. 2015; Parkes et al. 2016). In dogs, neuronal phospholipidosis has been observed in the central and peripheral nervous systems, although no neurologic deficiencies were reported (Cartwright et al. 2009).
In humans, posaconazole is approved only for the following groups of patients: those who are aged 18 years or older (EMA 2012b), receiving remission-induction chemotherapy for acute myelogenous leukemia (AML) or myelodysplastic syndromes (MDS) expected to result in prolonged neutropenia, and those at high risk of developing IFIs. It is also indicated for prophylaxis in recipients of hematopoietic stem cell transplants (HSCT) undergoing high-dose immunosuppressive therapy for graft-versus-host disease and who are at high risk for developing IFIs and salvage therapy of invasive aspergillosis in patients with a disease condition that is refractory to amphotericin B or itraconazole and in patients who are intolerant of the other medicinal products (Herbrecht et al. 2002; Cornely et al. 2007; Ullmann et al. 2007; Walsh et al. 2008).
In animals, although there is little experience with its use in different species, there are emerging data that posaconazole may be effective for the treatment of invasive aspergillosis in dogs (Corrigan et al. 2016; Stewart and Bianco 2017). Posaconazole is primarily metabolized by glucuronidation and thus should be used with caution in cats, which lack major UDP-glucuronosyltransferase enzymes (Court 2013). However, there is a case report in which posaconazole was successfully used with minimal adverse effects to treat a cat with invasive aspergillosis caused by an itraconazole-resistant isolate (McLellan et al. 2006). Posaconazole administered at a dosage of 5 mg/kg PO q12 h appears to be safe for prolonged treatment of disseminated Aspergillus infections in dogs. Long-term survival >1 year is possible with prolonged treatment, but relapse is common (Corrigan et al. 2016). Successful treatment with posaconazole has been also reported in two cats with fungal disease in which other antifungal treatment had failed (Mawby et al. 2016). Those cases involved a Mucor subcutis infection of the nose and invasive orbital aspergillosis (McLellan et al. 2006; Wray et al. 2008).
A veterinary product containing orbifloxacin and posaconazole in a mineral oil-based system is available for treatment of otitis externa in dogs associated with susceptible strains of yeast (Malassezia pachydermatis') and bacteria (coagulase positive Staphylococci, Pseudomonas aeruginosa, and Enterococcus faecalis).
Isavuconazole
Isavuconazole is the newest broad-spectrum triazole available for treatment of severe invasive and life-threatening fungal diseases in humans (Seyedmousavi et al. 2015b). The prodrug isavuconazonium sulfate (BAL8557) (Ohwada et al. 2003) is a highly potent water-soluble triazole suitable for both oral and intravenous administration. BAL8557 consists of a triazolium salt linked to an aminocarboxyl (N-[3-acetoxypropyl]-N-methylamino-carboxymethyl) via an ester moiety. After oral and intravenous administration, it rapidly and almost completely (>99%) undergoes enzymatic activation via plasma esterases followed by spontaneous chemical degradation to release the active drug isavuconazole (BAL4815, formerly RO-094815) and an inactive cleaved product, BAL8728 (Odds 2006; Schmitt- Hoffmann et al. 2006a, b).
Isavuconazole has a broad spectrum of in vitro activity and in vivo efficacy against a wide range of yeasts and molds including Aspergillus spp., Fusarium spp., Candida spp., the Mucorales, Cryptococcus spp., melanized and dimorphic fungi, dermatophytes that can reproduce in culture (by unilateral budding), and their filamentous co-spp. (Odds 2006; Warn et al. 2006; Guinea et al. 2008; Martin de la Escalera et al. 2008; Perkhofer et al. 2009; Rudramurthy et al. 2011; Shivaprakash et al. 2011; Espinel-Ingroff et al. 2013; Gregson et al. 2013; Seyedmousavi et al. 2013b).
Isavuconazole is available in oral (capsule) and intravenous formulations. In both formulations, the prodrug, isavuconazonium sulfate, is present and is rapidly converted to the active moiety isavuconazole following administration. The halflife is extensive in humans (~130 h) and very short in mice (~3 h) (Warn et al. 2009). Unfortunately, the pharmacokinetics of isavuconazole in other animal species is unknown.
Isavuconazole is effective for the treatment of invasive aspergillosis and mucormycosis (Seyedmousavi et al. 2015b; Maertens et al. 2016; Marty et al. 2016). To date, no study has been conducted using isavuconazole for the treatment of systemic fungal infections in veterinary patients.
16.2.3