Clostridial Vaccines
Francisco A. Uzal and J. Glenn Songer
Clostridial infections cause mostly acute and frequently fatal disease in cattle. The pathogenesis of most clostridial diseases is mediated by powerful toxins,1,2 and prevention is therefore based on immunoprophylactic amelioration of the effects of these molecules.
Unfortunately, the ready availability of mostly inexpensive and efficacious bacterins, toxoids, and bacterin-toxoids has not eliminated clostridial infections, mainly because these immunoprophylactic products are sometimes used poorly or not at all. Duration of immunity is poor in some cases, and frequent revaccination is required if adequate immunity is to be achieved. Accurate diagnosis remains an important component in management of clostridial diseases as it provides vital information on type of vaccines to use in a given area or herd.3-5 Immunization of cattle against clostridial diseases can be complicated by the development of site reactions, leading to trimming at slaughter.6 These problems are exacerbated with some of the multivalent modern clostridial vaccines and have stimulated the biologics industry to seek a new paradigm for preparation and delivery of vaccines. Approaches have included concentration of the antigen into smaller doses and use of alternate adjuvants. Recombinant proteins delivered by conventional means, application of slow-release media, in vivo expression from attenuated bacterial delivery systems, and production in vivo by replicon particles from alpha viruses will likely be a major focus of effort.Clostridium chauvoei (Blackleg) Bacterins
Blackleg occurs frequently despite long-term availability of generally effective bacterins.10 The most common route of exposure in cattle is likely ingestion, and dormant spores seeded within macrophages in the skeletal or cardiac muscle germinate when muscle damage provides appropriate conditions of lack of oxygen.
Signs in affected animals, when observed, include fever, anorexia, depression, and lameness. Sudden death is common. Lesions are characterized by extensive, dry, and emphysematous to edematous, hemorrhagic, and necrotic myositis with or without subcutaneous edema. In diagnosis, differentiation between blackleg and gas gangrene edema is important as both clinical signs and lesions may overlap.7Vaccination against blackleg is universally advocated, especially in cattle younger than 2 years. Dogma holds that protection arises from the immune response to a heat-labile soluble antigen, but C. chauvoei produces alpha toxin and several other toxic factors that may be equally important targets.8-11 Recommendations for immunization are summarized in Table 48.12.
Gas Gangrene Bacterins
Gas gangrene, historically called malignant edema, is a wound infection most frequently caused by C. septicum,i2,ri although other microorganisms, including Clostridium novyi type A, Clostridium chauvoei, Clostridium sordellii, and more rarely C. perfringens type A can also be involved. The infection usually follows direct contamination of a wound, including accidental trauma, iatrogenic injuries, and genital tract lacerations during delivery. Infection spreads mostly along fascial planes, and lesions that are initially warm and pitting become crepitant and cold. The clinical signs and lesions are similar to those of blackleg, except that subcutaneous and interstitial tissue is more frequently involved than muscle.13 “Braxy” or “Bradsot” is a form of C. septicum alimentary infection characterized by necrotizing abomasitis, which occurs most commonly in calves and lambs.14 Cattle are protected by two initial doses of the corresponding bacterin, 4 to 6 weeks apart, followed by an annual booster. Vaccination is recommended in areas with a substantial incidence of the disease13 (see Table 48.9). Vaccines elicit antibody responses to both somatic and toxin antigens, and research findings suggest a central role for C.
septicum alpha toxin.11,15,16 Several bacterins contain immunogens to most or all the components of the gas gangrene complex.Clostridium haemolyticum (formerly called Clostridium novyi type D) (Bacillary Hemoglobinuria) and Clostridium novyi type B (infectious necrotic hepatitis or black disease) Bacterins
Bacillary hemoglobinuria, also called redwater, is caused by Clostridium haemolyticum and it occurs mostly in cattle, although
■ TABLE 48.12
General Considerations for Use of Clostridial Seven-Way and Eight-Way Bacterin-Toxoidsa
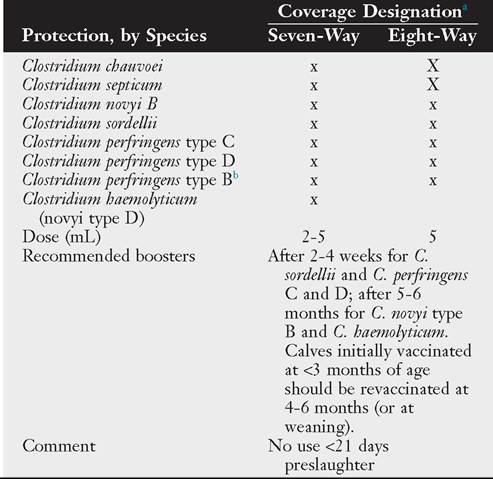
aNote that many combinations are available commercially, including some that also contain immunogens against nonclostridial diseases. Some of these combinations also include tetanus toxoid.
bNo currently licensed product is produced by use of cultures of C. perfringens type B, but protection against type B infection is implied by the inclusion of toxoid prepared against type C (beta toxin) and type D (epsilon toxin) strains.
occasional cases in sheep have been reported. C. novyi type B causes infectious necrotic hepatitis (black disease) of sheep, with occasional cases being reported in cattle.17,18
The hallmark lesion of both diseases is acute focal or multifocal liver necrosis. Dormant spores in Kupffer cells germinate when liver injury provides appropriate anaerobic conditions, most frequently associated with migration of larvae of Fasciola hepatica through the liver parenchyma, although cases of both diseases may occur in animals free of this parasite.17,18
Beta toxin, a homolog of C. perfringens alpha toxin (CPA), mediates the pathogenesis of bacillary hemoglobinuria, and C. novyi alpha toxin seems to be the main virulence factor involved in the pathogenesis of infectious necrotic hepatitis. Both diseases usually occur in well-nourished animals, with bacillary hemoglobinuria occurring mostly in animals 1 year of age or older,17,18 and infectious necrotic hepatitis affecting mainly adult animals.19 Tissue damage caused by migrating liver fluke larvae or other less understood factors allows germination of dormant spores in Kupffer cells.
Vegetative growth yields focal or multifocal hepatic necrosis with local production of a large amount of toxins. In cattle with bacillary hemoglobinuria, systemic dissemination of beta toxin via the bloodstream results in intravascular hemolysis, hemorrhage, and hemoglobinuria.17 When urine takes on the color of port wine, about 50% of the red cells have lysed and death ultimately results from anoxia. Because the pathogenesis of infectious necrotic hepatitis is thought to be mediated mostly by C. novyi alpha toxin with much less involvement of beta toxin, jaundice and hemoglobinuria are not usually observed in animals with this disease.19A vaccination program is essential for herds pastured in endemic areas. When heavy exposure to fluke metacercariae is expected, an initial double dose, 4 to 6 weeks apart, of
bacterin-toxoid should be administered to all cattle older than age 6 months, before they are pastured in the spring. This should be followed by a single annual booster a few weeks before the season when heavy exposure to flukes is expected. Liver fluke control also helps prevent cases of both bacillary hemoglobinuria and infectious necrotic hepatitis.
Clostridium botulinum (Botulism) and Clostridium tetani (Tetanus) Toxoids
Botulism is caused by C. botulinum neurotoxins, which block acetylcholine release from cholinergic nerve endings.20 Cattle in the United States are most commonly affected by type C, and this is commonly associated with an infected animal carcass in the feed. Clinical signs include incoordination, flaccid paralysis, and difficulty in swallowing; respiratory paralysis causes eventual death.20,21
Toxoids of botulinum toxins can be employed for immunoprophylaxis, but vaccination is usually practiced only in populations at immediate risk, such as beef cattle grazed on phosphorus-deficient range land, where cattle tend to chew on bones of carcasses left in the field, increasing the risk of contamination.22 Feeding of poultry litter poses a similar problem, in that it may contain animal remains, but this practice has now been suspended in the United States.
Spores of C. tetani are found in soil, and animal hosts are usually infected in association with some traumatic event. Spores introduced to tissue under proper conditions of anaerobiosis germinate and produce tetanus neurotoxin.23 Tetanus can develop after several different interventions in cattle including, but not limited to, calves after castration by the elastrator method.24,25 Cases may also occur in postparturient dairy cows.23 Toxin moves retrograde, binding to presynaptic axonal terminals and resulting in muscular tremor and increased stimulus response; continued motor neuron hyperactivity causes sustained tetanic spasms in the innervated muscles and then permanent rigidity. Death is due to respiratory failure.23
Acquired resistance to tetanus is based on circulating antitoxin, and widespread vaccination with toxoid in populations at risk has dramatically lessened the impact of tetanus on animal production. Neonatal passive immunity acquired from the dam is followed by active immunization with toxoid at 2 to 3 months of age followed by a booster 4 to 6 weeks later. Single annual boosters are commonly recommended at 1- to 5-year intervals. Passive immunotherapy is intended to neutralize preformed toxin, although it is much more effective when used prophylacti- cally than therapeutically. Vaccination is recommended in endemic areas, but universal vaccination is not usually recommended as a cost-effective means for control of tetanus.
Clostridium perfringens Toxoids
C. perfringens causes various diseases in domestic animals, and those of greatest importance affect the gastrointestinal tract4 (Table 48.13) (see ruminant section of Chapter 32). This organism has been historically classified into 5 types (A, B, C, D, and E) on the basis of the production of one or more of the following toxins: alpha, beta, epsilon, and iota. Two additional types (i.e., F and G), have been recently added on the basis of the production of enterotoxin and and necrotic B-like toxins (see Table 48.13).26
C.
perfringens type A is present in the intestine of most clinically healthy animals. Although this microorganism has been associated with gastroenteric syndromes in many mammals including, among others, cattle, final proof of involvement of C. perfringens type A in these syndromes is lacking and there are currently no accepted criteria to establish a diagnosis of C. perfringens type A enteritis in cattle.4Type B disease is a rare disease that affects mostly sheep, and it has not been diagnosed in the United States. Pathogenesis is thought to be mediated by beta and epsilon toxins.27 Type C strains affect several mammalian species including cattle. Because beta toxin, the main virulence factor of C. perfringens type C, is exquisitely sensitive to trypsin and other intestinal proteases, type C disease occurs mostly in neonatal animals in which trypsin is naturally inhibited by colostrum present in the intestine. In the absence of trypsin activity, beta toxin accumulates and produces local hemorrhage and necrosis, as well as systemic effects.28,29 Type D produces enterotoxemia in sheep and goats and rarely in cattle. Epsilon toxin is the main virulence factor of type D strains; this toxin facilitates its own absorption through the intestinal wall and, in circulation, damages the central nervous system and other systems distant from the gut.30 C. perfringens type E has been associated, albeit infrequently, with cases of enterotoxemia in lambs, calves, and rabbits. However, the few diagnoses of this condition reported so far were based on isolation of C. perfringens type E from the intestinal content of sick animals, which is not considered a diagnostic criterion for C. perfringens intestinal diseases because this organism is found in most healthy animals.4
C. perfringens types F and G are not involved in diseases of cattle.26
Although a few commercial vaccines including type A toxoid are currently available, because type A disease has not been definitely proved to occur in cattle, the use of such vaccines has not been fully evaluated.
Vaccination against type C enterotoxemia is recommended only in herds where the disease has been documented. Because the disease affects mostly neonates, vaccination of all dams before calving is required, and immunity is provided to calves via immune colostrum. Initial immunization should be followed by a booster after 3 to 4 weeks, with the second dose (and subsequent boosters precalving) administered approximately 2 to 3 weeks before parturition.
Type D enterotoxemia occurs sufficiently infrequently in cattle that vaccination may not be cost-effective. No commercial products are licensed in the United States for use against infections by strains of type E. Although production of autogenous toxoids or bacterin-toxoids have been used, these have not been scientifically evaluated and information about their efficacy is lacking.
■ TABLE 48.13
Classification Schedule of Clostridium perfringens Based on Production of 6 Toxin
C. perfringens
| Toxin Type | alpha | beta | epsilon | iota | enterotoxin | NetB |
| + | + | |||||