Miscellaneous Bovine Rickettsial, Bacterial, and Viral Disease Vaccines
Derek A. Mosier
A number of bovine vaccines are available for anaplasmosis, infectious bovine keratoconjunctivitis, staphylococcal mastitis, anthrax, interdigital necrobacillosis (foot rot), papillomatous digital dermatitis (foot warts), rabies, and fibropapillomas.
These are discussed individually next and summarized in Table 48.14.Anaplasmosis
Anaplasmosis is a vectorborne or mechanically transmitted disease caused by the rickettsia Anaplasma marginale.i,2 The disease occurs worldwide and is most prevalent in tropical and semitropical areas. Anaplasmosis is the only major tickborne disease of cattle in North America, being enzootic in the southeastern and some midwestern and western states and sporadic in the northern states and Canada.1-3 In enzootic areas with adequate numbers of arthropod vectors, most adult cattle become naturally immune through repeated exposure. Maternal antibodies protect calves until they also become subclinically infected and develop immunity. Disease is more severe in older cattle than in calves, and nonimmune older cattle are particularly at risk when they are moved into an endemic area.1,4 Susceptibility to disease occurs when there is a lack of arthropod vectors to maintain natural infection and immunity or when a nonim- mune adult is introduced into an enzootic area. In these situations or when vector or environmental conditions suggest an increased risk of disease, vaccination can be beneficial.
No widely marketed commercial vaccines against anaplasmosis were available as of 2012 in North America. A killed vaccine (Anaplasmosis Vaccine, University Products LLC, Baton Rouge, La.) is available in some states, including Arkansas, California, Florida, Indiana, Illinois, Iowa, Kansas, Kentucky, Louisiana, Mississippi, Missouri, Nevada, Oklahoma, Oregon, Tennessee, Texas, and Wisconsin, and in Puerto Rico.
The vaccine consists of an emulsion of concentrated inactivated A. marginale antigens and adjuvant suspended in 10% oil, similar to the last widely available commercial vaccine that was discontinued in 1999 (Plazvax [Schering-Plough Animal Health]). The killed vaccine is not USDA licensed, but it is USDA approved for use as an experimental vaccine. The vaccine has reportedly been used successfully in cows at all stages of pregnancy without an episode of neonatal isoerythrolysis. In endemic areas the vaccine is recommended for use just before the onset of the vector season. Vaccine-induced immunity does not generally occur until 2 weeks after administration of the second dose of an initial series or 2 weeks after a booster dose in previously immunized cattle.5,6 Vaccination does not prevent infection or clinical disease and does not eliminate A. marginale from a herd, but it does reduce the severity and incidence of disease.1,6 Inactivated vaccines could be used in conjunction with oxytetracycline in the face of outbreaks to provide both temporary and more prolonged protection.A sheep-passaged modified live vaccine (Anavac [PHL Associates, Davis, Calif.]) has been used in California and Latin America.7 Because this vaccine causes mild clinical disease, it has limited use for vaccination of mature susceptible cattle.1,7 If the vaccine is administered to cattle older than 2 years of age, anemia, severe clinical disease, and death may occur, especially in bulls and heavily lactating cows.7 The vaccine is recommended for use in healthy cattle between age 1 month and 2 years and is most commonly administered to 7- to 24-month-old cattle in herds in endemic areas. Concurrent use of certain antibiotics or other live or MLV vaccines is contraindicated.
A live vaccine (Frozen Anaplasmosis [Tick-borne gallsickness] vaccine for cattle [Onderstepoort Biological Products, Onderste- poort, South Africa]) composed of A.
marginale subsp. centrale, a less pathogenic species or subspecies of A. marginale, is used in some countries including Africa, Australia, Israel, and Latin America but not in North America.6,8,9 This vaccine consists of standardized and frozen red blood cells from splenectomized cattle that were infected with A. marginale subsp. centrale. The vaccine is recommended for use in 4- to 9-month-old cattle; older cattle have an increased risk of severe vaccine-induced disease. The vaccine produces mild disease but protects against subsequent severe disease caused by A. marginale. Immunity is considered long term or possibly for life if subsequent natural exposure occurs to ensure development of durable immunity.Immunity to A. marginale is proposed to involve humoral responses to a variety of major surface proteins and enhanced macrophage phagocytosis and killing, both mediated by IFN-γ-producing CD4+ T lymphocytes.1,10,11 Inadequate protection from vaccines during field use can result from antigenic variability of the organism, geographic differences in the organism that result in a lack of cross-reactivity between A. marginale strains, and weak immune responses to protective A. marginale antigens.1,4, Purified native, recombinant, and tick culture-derived A. marginale immunogens and DNA vaccines are being investigated for possible commercial use in the future.6,9,12,13,15-17
Infectious Bovine Keratoconjunctivitis
The most common infectious agent associated with infectious bovine keratoconjunctivitis (IBK) is M. bovis.1 Vaccination is most effective when done before fly season in herds with a history of problems. Certain breeds (e.g., Herefords, Hereford crosses) are particularly susceptible and may benefit from vaccination.1,2 Commercial vaccines used to help prevent the disease consist of inactivated cultures of various strains of M. bovis.2 Some products recommend two doses given 3 weeks apart for initial vaccination, beginning as early as 3 weeks of age to no earlier than 5 months of age.
Other products recommend a single dose administered 3 to 6 weeks before the predicted onset of the disease season, with annual vaccination thereafter. M. bovis bacterins are also available in combination with seven-way clostridial bacterin-toxoids.4 Although multivalent M. bovis bacterins can provide some protection in field use, efficacy varies depending on the M. bovis strains present in the bacterin and those responsible for disease.1,5-7 Seven different disease-producing serogroups of M. bovis are recognized on the basis of differences in pili, and there is variable cross-reactivity between serogroups.3 Pilin gene rearrangements and pilin-type switching can allow M. bovis to switch from expression of one type of pilus antigen to another, making it difficult to predict what serogroup(s) may be necessary for protection.2,3,6 Monovalent bacterins are generally ineffective in field use, and multivalent bacterins provide neither consistent nor reliable protection.3,5-7 Vaccines must incorporate pili from all major serogroups or conserved immunogenic portions of all serogroups to provide optimum protection.3,6,7 Experimental recombinant vaccines containing cloned pili of various sero- groups have demonstrated some promise for future vaccines.5,6 Another immunogen considered important for protection isM. bovis β-hemolytic corneotoxic and leukotoxic cytotoxin.1-3 Experimental vaccines containing hemolytic cytotoxin preparations alone or in combination with pilus antigens have shown some efficacy in experimental trials.1,3,8-10 Other potential immunogens include iron-regulated OMPs, proteases, fibrinolysins, and phospholipases.1-3 Vaccine-induced protection is
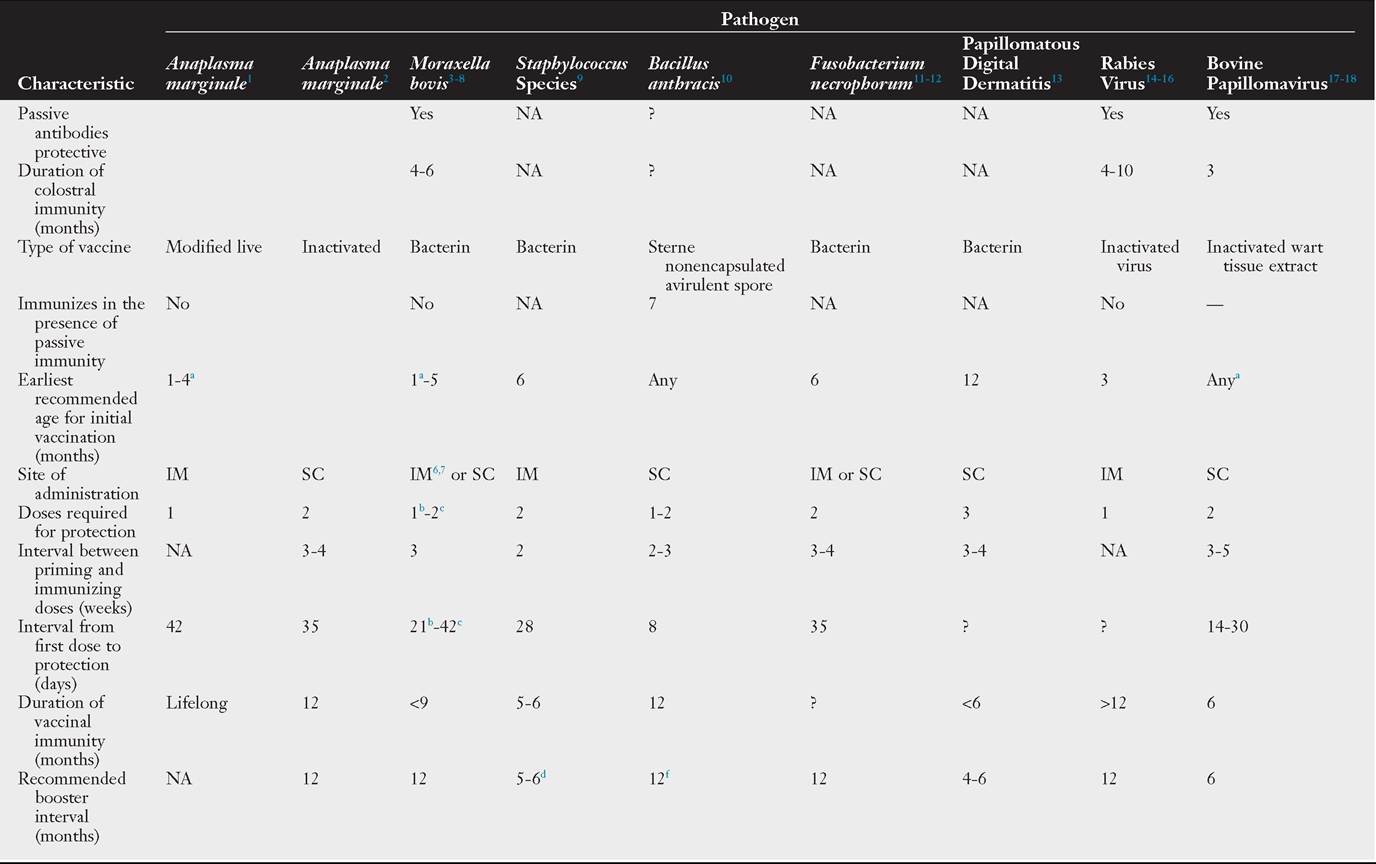
TABLE 48.14
Recommendations for Use of Some Bovine Disease Vaccines: Anαpfαsmα, Moraxeiia1 Staphylococcus, Anthrax, Fusobacterium necrophorum, Papillomatous Digital Dermatitis, Rabies, and Papillomas
Continued
CHAPTER 48 Use of Biologies in the Prevention of Infectious Diseases

O) O)
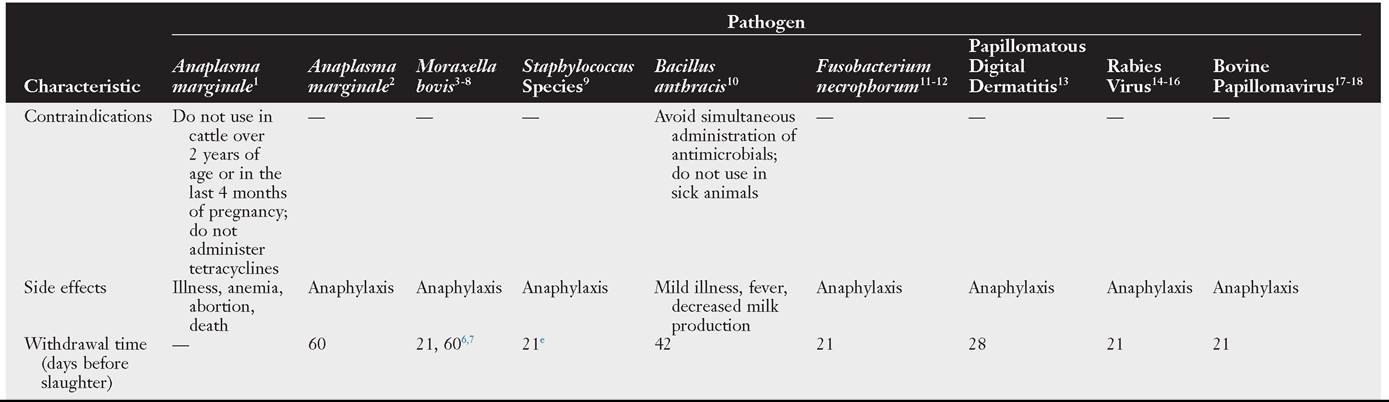
TABLE 48.14
O) O) σ>
Recommendations for Use of Some Bovine Disease Vaccines: Anαpfαsmα, Moraxella1 Staphylococcus, Anthrax, Fusobacterium necrophorum, Papillomatous Digital Dermatitis, Rabies, and Papillomas—cont'd
aCalves vaccinated before the age at which passive immunity no longer exists should be revaccinated on reaching that age.
bOihadjuvant vaccines.cAluminum hydroxide-adjuvant vaccines.
dGive booster 3 to 6 weeks before calving.
eNo milk withdrawal required.
fBooster can be given sooner in heavily contaminated areas.
?, Unknown; IM, intramuscular administration; NA, not applicable; SC, subcutaneous administration.
1Anavac, PHL Associates, DaHs, CA.
2Anaplasmosis Vaccine, University Products LLC, Baton Rouge, LA.
3I-Site, AgriLaboratories, St. Joseph, MO.
4MaxiZGuard Pinkeye bacterin, Addison Biological Laboratoty, Fayette, MO.
5Ocu-Guard MB and Alpha-7 MB, Boehringer Ingelheim, St. Joseph, MO.
6PiHguard Pinkeye-1 Trivalent and Piliguard Pinkeye + 7, Merck Animal Health, Summit, NJ.
7Pinkeye Shield XT4, Novartis Animal Health, Larchwood, IA.
8Vision 7 20/20 with Spur, Intervet Inc., Merck Animal Health, Summit, NJ.
9Lysigin, Boehringer Ingelheim AVtmedica, St. Joseph, MO.
10Anthrax Spore Vaccine, Colorado Serum Co., Denver, CO.
11Volar, Intervet, Millsboro, DE 19966.
12Fusogard, Novartis Animal Vaccines, Larchwood, IA.
13Serpens species bacterin, Hygieia Biological Laboratories, AVoodland, CA.
14Defensor 3, Zoetis, Florham Park, NJ.
15Rabdomun, Schering-Plough Animal Health, Union, NJ.
16Imrab 3 and Imrab Large Animal, Merial, Duluth, GA.
17AVart vaccine, AgriLaboratories, St. Joseph, MO.
18AVart vaccine, Colorado Serum Co., Denver, CO.
correlated predominantly with a suitable lacrimal immune response (predominantly IgA but also IgM and IgG) and not with serum antibody levels to M. bovis antigens.1-3 Therefore an antigen delivery system that enhances lacrimal and mucosal immunity is an important feature of an effective vaccine.11 The presence of other agents contributing to IBK (e.g., Moraxella [Branhamella] ovis, Mycoplasma bovoculi, or BHV-1) should also be considered when there is poor M.
bovis vaccine efficacy.12 Autogenous M. bovis or M. bovis plus M. bovoculi vaccines have not been consistently effective against the disease.1,13,14 Use of MLV vaccines for IBR is contraindicated in the presence of an outbreak of IBK because it may exacerbate the IBK.1Staphylococcal Mastitis
S. aureus is considered one of the most important causative agents of bovine mastitis.1 Vaccination against S. aureus may be beneficial in dairy herds that have an existing mastitis problem,1,2 but vaccination in well-managed dairy herds with a low level of staphylococcal mastitis may not provide much economic benefit.2 Staphylococcal bacterins contain conserved antigens or antigens from multiple strains or serotypes of S. aureus.i- The typical recommended vaccination protocol is two doses given 2 weeks apart, followed by revaccination at 6-month intervals. Vaccination can start at 6 months of age, and one of the semiannual doses should be given 3 to 4 weeks before calving. Vaccination with S. aureus bacterins does not generally eliminate disease but can substantially reduce clinical mastitis and the incidence of subclinical and chronic staphylococcal infection.1,2,5,6 Vaccination may be more effective in heifers because of their initial lower basal immunity compared with older cows.6 The benefits of immunity induced early in life include the abilities to clear the organism and resist chronic infection on initial natural exposure. Vaccination during the dry period may be more effective than vaccination during lactation. In some but not all studies, vaccination has reduced somatic cell counts in milk.5,6 Vaccination in combination with antimicrobial therapy has been successfully used to eliminate chronic staphylococcal mastitis.7
In considering the use of staphylococcal vaccines, the prevalence of various pathogens that can cause mastitis must be considered. For mastitis caused by S. aureus, differences between the S. aureus strains in vaccines and the strains specifically responsible for the disease may diminish vaccine efficacy.1,4,8 Both long-standing bacterins and some newer-technology vaccines have achieved positive results.1,9 Experimental trials suggest that more effective vaccines may be derived by stimulating immune responses to combinations of S. aureus capsular polysaccharide.10 A vaccine based on technologies used for human staphylococcal vaccines that incorporates capsular polysaccharide from the three S. aureus serotypes most commonly associated with mastitis stimulated immunologic parameters necessary for protection.11 Other vaccines have used highly conserved membrane proteins, iron-regulated proteins, a staphylococcal superantigen conserved by many mastitis strains, and DNA vaccines directed against adhesin proteins in attempts to achieve the “universal” S. aureus vaccine.5,12-14
In herds where other pathogens are a major cause of mastitis, S. aureus vaccines may be of minimal benefit.2 Other important causes of bovine mastitis include Streptococcus spp. (e.g., Streptococcus uberis, Streptococcus dysgalactiae, and Streptococcus agalactiae) and coliform bacteria (e.g., E. coli). Recombinant vaccines containing S. aureus and S. agalactiae have shown some promise 15
in experimental models.15 Experimental vaccines composed of bacterial proteins derived from S. uberis and S. dysgalactiae reduced somatic cell counts compared with controls after challenge.16,17 E. coli J5 vaccines have also been used to successfully reduce the severity of mastitis (reviewed elsewhere in this section).
Anthrax
Anthrax is an acute, highly fatal disease caused by Bacillus anthracis.1 Vaccination has proven to be an effective means of controlling the disease in endemic areas and in the face of outbreaks.1-3 Bovine anthrax vaccines are derived from the live toxigenic, nonencapsulated spore vaccine developed by Sterne and consist of spores suspended in a diluent containing saponin and glycerin.1 Annual vaccination of livestock in areas of endemic anthrax is recommended 4 weeks before outbreaks are expected, typically in the spring to provide protection during the summer months.1 A single dose generally provides adequate immunity for about a year, but a second dose given 2 to 4 weeks after the first is sometimes recommended. Cattle should not be vaccinated within 42 days of slaughter. Antibiotics should not be administered within 7 days of vaccination to avoid interference with in vivo growth of the vaccine organism. Outbreaks can occur sporadically but often occur in areas with a history of flooding followed by drought.4,5 Vaccination in the face of an outbreak does not protect all cattle, but the spread of infection and the number of new cases generally declines within 10 days.3,5 Localized subcutaneous edema can develop at the injection site within 24 hours; it may last for several days and is sometimes severe.2 Since the intentional release of B. anthracis via the mail system in 2001, there has been increased interest in technologies for the development of an efficacious long-acting human vaccine for anthrax.2,6-8 Some of these technologies could hold promise to reduce some of the localized side effects of the current bovine vaccine,9 but it is unlikely a new bovine vaccine will match the safety, efficacy, and cost-effectiveness of the Sterne strain vaccine in the foreseeable future. All anthrax outbreaks should be reported to local regulatory and public health officials, and appropriate guidelines for vaccination should be followed, including quarantine and vaccination of all susceptible livestock on affected and surrounding premises.
Interdigital Necrobacillosis (Foot Rot)
Interdigital necrobacillosis (foot rot) in cattle results from interdigital infection with Fusobacterium necrophorum, with lesser contributions from Porphyromonas levii (previously classified as a subspecies of Prevotella [Bacterioides] melaninogenica) and sometimes Dichelobacter (Bacterioides) nodosus (the most common cause of foot rot in sheep) and other bacteria.1-3 Commercial F. necrophorum bacterins to aid in the prevention of foot rot (and hepatic necrobacillosis) are available for use in cattle. Recommendations for initial vaccination are two doses given 3 to 4 weeks apart, followed by annual revaccination. Vaccination is also recommended when endemic conditions exist or when exposure is imminent. The efficacy of F. necrophorum vaccines is unclear because hepatic abscesses are sometimes the study focus, but some benefit for foot rot has been demonstrated in experimental studies and field trials.4 Vaccination is especially recommended in herds with a high incidence of disease. Protective immunity most closely correlates with the level of anti- leukotoxin antibodies.5 In experimental models, truncated recombinant leukotoxin proteins provide protection and presumably would have some benefit against interdigital F. necrophorum infection.6,7 Most foot rot infections involve single rather than multiple strains of F. necrophorum, so a vaccine that targets the specific strain involved should be effective.8
Papillomatous Digital Dermatitis (Foot Warts)
Papillomatous digital dermatitis, or foot warts, can be a serious problem in dairy cattle.1 The disease is characterized by ulcerative to proliferative digital lesions that most often occur in replacement heifers and younger cows after introduction into a milking herd.1,2 Risk is greatest in larger dairy breeds in herds of greater than 500 head. Treponema spp. are most commonly isolated from lesions and are considered the most important cause of foot warts. A wide variety of Treponema are incriminated, including T. phagedensis, T. denticola, T. vincentii/T. medium, and T. pedis.3'5 No virus was seen in biopsies from multiple warts from dairy cattle in two herds.6 Several bacterial species have also been isolated from lesions, including Fuso- bacterium necrophorum, Serpens spp., and Porphyromonas levii.7,8 However, the precise combinations of these agents necessary to produce disease remain unclear. Commercial bacterins are available for use as preventives and/or aids to treatment and consist of killed cultures of Serpens spp. or Treponema spp. organisms. Recommendations are for three doses administered SC at 3- to 4-week intervals, followed by revaccination every 4 to 6 months. Company field trials report reduced onset of new infections and sometimes more rapid resolution of existing infections in vaccinated cattle. However, some trials failed to show significant improvement in vaccinated cows compared with unvaccinated ones.8,9 The requirement for frequent boosters and the high recurrence rates of natural infection suggest that immunity to the disease is short lived or weak.2
Rabies
Rabies is a highly fatal zoonotic neurologic disease caused by a rhabdovirus.1 Bovine rabies in North America is generally uncommon, and routine vaccination of cattle is not recommended in most situations.2 However, vaccination may be a consideration in rural areas of Latin America, where vampire bats are important sylvatic vectors, or Africa, where exposure to infected dogs is a major cause of bovine rabies.3,4 In endemic areas, vaccination of valuable cattle or herds may be a reasonable precautionary measure. This is particularly true in situations where cattle are in frequent contact with human beings, in order to reduce the anxiety of animal workers and minimize the likelihood of human exposure. Currently licensed rabies vaccines for cattle contain inactivated cell culture-derived virus.5 The recommended regimen is initial vaccination at 3 months of age followed by annual vaccination thereafter. Because the duration of protective neutralizing antibody levels after initial vaccination can vary, some experts have suggested that a second booster dose be given either 1 month after initial vaccination or at 6 months of age.6 Subsequent annual revaccination induces strong anamnestic responses that persist for 1 year or longer.6 In Latin America, modified live vaccines are sometimes used but do not stimulate the same level of immunity as inactivated virus vaccines. A Capripoxvirus vector expressing rabies virus glycoprotein has shown promise in providing long-term protection against rabies (and lumpy skin disease) and may be a cost-effective mechanism for rabies control in cattle in some developing countries.7,8
Fibropapillomas (Warts)
Fibropapillomas (warts) are manifested in a variety of forms and locations, each caused by 1 of over 13 different types of bovine papillomaviruses (BPV).1,2 Lesions associated with papillomaviruses can occur in the epidermis of the head, face, neck, and legs (BPV-1 and BPV-22); upper alimentary and urinary tracts (BPV-4); teats and udder (BPV-1, BPV-3, BPV-5, and BPV-6); and genital epithelium (BPV-1).1,2 Immunity after infection or vaccination is virus type specific and is induced by viral structural proteins.1 Therefore the efficacy of both autogenous and commercial vaccines depends on which viral antigens are incorporated into the vaccine and which virus type is responsible for the disease. Vaccines containing BPV-1 and BPV-2 are generally effective for prevention, with some reports that BPV-2 also aids in regression of existing lesions.1,3 Vaccines are usually ineffective for treatment or prevention of disease caused by BPV-3 and BPV-5.3 Vaccination with structural capsid proteins of BPV-4 generally induces long-lasting immunity and is effective in preventing papillomas caused by BPV-4.1 However, in immunocompromised cattle (e.g., those ingesting bracken fern), papillomas may spread and can progress to squamous cell carcinoma.2,4 Interpreting the response to vaccination against fibropapilloma can be complicated by spontaneous regression of some lesions. Lesions associated with BPV-1, BPV-2, and BPV-4 usually regress spontaneously within 1 to 12 months, whereas lesions caused by BPV-3 and BPV-5 do not normally regress spontaneously.2,3
Commercial vaccines consist of inactivated virus-laden tissue extracts derived from bovine papillomas.5 The recommended regimen is an initial dose divided and given in at least two different sites, followed by a second dose in 3 to 5 weeks. Vaccination should continue for at least 1 year after elimination of disease from the herd. Autogenous vaccines can be made by homogenization and inactivation (0.3% formalin) of excised wart tissue, followed by dilution of the homogenate in physiologic saline and filtration through gauze. Three 1- to 5-mL intradermal injections given at 1-week intervals are recommended. Because autogenous vaccines generally contain the virus type associated with the disease, these often provide favorable results for both regression and prevention.6 Vaccination is most commonly used with valuable animals destined for competitive shows or overseas sale.3 Recombinant or native BPV proteins derived from multiple virus types have shown promise in experimental studies and could form the basis for a vaccine that protects against all BPV types.7