Esophagogastroduodenoscopy
1.5.4.1 Preparation and anesthesia
Patients with GI disease and especially those that are vomiting sometimes have delayed gastric emptying. Therefore, food should be withheld for at least 24 hours prior to the procedure.
One should not administer barium or sucralfate for at least 1 and preferably 2 days before the procedure. Various preanesthetic-anesthetic regimens may be used; glycopyrrolate plus either butorphanol or acetylpromazine is effective. However, narcotics (e.g., morphine, oxymorphone, or fentanyl) and prokinetic agents (e.g., metoclopramide) should be avoided.5,6 Ketamine may relax the feline pylorus and may thus facilitate entry into the duodenum, although it also relaxes the lower esophageal sphincter, often making it necessary for someone to occlude the esophagus so that the stomach can be kept inflated during the procedure. Induction with propofol and maintenance with isoflurane is effective. Sevoflurane is also useful, especially in very ill animals, but it is important to assist respiration when using sevoflurane because the diminished tidal volume due to insufflation of the stomach with air may cause the patient to wake up in the middle of the procedure. The patient is placed in left lateral recumbency with the head slightly extended. A reliable mouth gag is always used, as a single bite on the endoscope may cause severe damage that requires expensive repairs.1.5.4.2 Technique
The hollow viscus to be evaluated should be insufflated with enough air so that all of the mucosal surface can be inspected. Excessive insufflation of the stomach, which causes symptomatic gastric dilation, should be avoided. Also, panoramic views are often more effective than getting too close. This is especially true when a “red out” (i.e., the endoscope is too close to the mucosa and everything is out of focus) is experienced.
The endoscope should only be advanced when the lumen can be visualized. Finally, while advancing the endoscope, it is often best to try to keep the tip of the scope aimed at the center of the lumen.1.5.4.3 Gastroduodenoscopy2,7
The insertion tube is lightly lubricated and gently inserted into the mouth, much like an orogastric tube. As the larynx is approached and one can see the endotracheal tube entering the trachea, the tip of the endoscope is directed slightly dor- sally and gently advanced towards the cricopharyngeal sphincter. Immediately upon entering the cricopharyngeal sphincter, the operator should begin to insufflate so that there is moderate distension of the esophagus allowing one to inspect the mucosa while advancing the endoscope towards the lower esophageal sphincter (LES) and the stomach. The LES usually appears as a “slit” although it sometimes is wide open. If the LES is closed, the operator should aim for the center of the sphincter and advance the endoscope gently rather than pushing hard and trying to force the tip into the stomach. The next step is determined by the size of the patient and the area(s) of interest. In small or medium-sized animals, one should first distend and examine the stomach (i.e., “typical gastroduodenoscopy”). In large or very long dogs in which examination and biopsy of the duodenum is important, it is often better to enter and examine the duodenum before examining the stomach (i.e., “modified gastroduodenoscopy” - see below).
Typical gastroduodenoscopy
It is critical to systematically examine all mucosal surfaces of the stomach because gastric lesions can be localized. After entering the stomach, the stomach is distended with air until the entire gastric mucosal surface can be examined. If the stomach cannot be distended because air escapes through an open LES, then an assistant should gently apply pressure on both sides of the cervical trachea in order to occlude the cervical esophagus and trap air in the upper GI tract.
However, insufflation must be limited in order to avoid excessive gastric distension. Even moderate overdistension impedes ventilation with both oxygen and inhalant anesthetics, and it may even become necessary to deflate the stomach so that the patient can be maintained under anesthesia.After the stomach is distended, a four-quadrant scan of the stomach should be performed. Starting with the tip of the scope near the LES, the tip is moved in a square pattern going from 10 o’clock to 2 o’clock to 5 o’clock to 7 o’clock. Second, the tip of the scope is advanced and then maximally retroflexed so that the LES and fundus can be examined (i. e., one can see the insertion tube of the endoscope entering the stomach through the LES). Insufficient examination of the fundic area is a common mistake of inexperienced operators, but this is the area where many foreign bodies as well as some infiltrative lesions can be found. After complete inspection of the gastric fundus, the tip of the endoscope is straightened and is advanced into the antrum by pushing the insertion tube into the patient. In this way, the tip of the scope will slide along the greater curvature, advancing into the antrum and towards the pylorus. The endoscopist may need to deflect the tip of the endoscope just a little bit upwards in order for it to enter the antrum without catching on a mucosal fold. Upon entering the antrum, one can see the pylorus at the back and to the left. The entire antral mucosa should be examined while advancing the tip of the endoscope towards the pylorus.
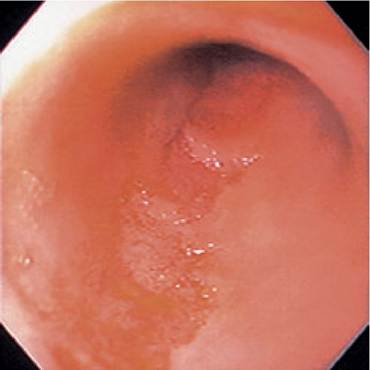
Figure 1.47:
Abrasions of the duodenal mucosa. Endoscopic view of duodenal mucosa with a linear abrasion caused by the endoscope. Such iatrogenic lesions must be distinguished from spontaneous ones.
To enter the duodenum, the pylorus should be kept in the middle of the viewing field while advancing the tip.
It should be noted that the tip of the endoscope is larger than the field seen by the endoscopist because the viewing port at the tip of the endoscope generally comprises 30 kg) or in very long-bodied dogs (e. g., Greyhounds), insufflation may result in the insertion tube being too short to enter the duodenum. If this is a concern, one should start by insufflating as little air as possible into the esophagus. Once in the stomach, one should slightly deflect the tip of the endoscope up about 30 degrees and gently advance it (blindly at times) attempting to slide it into the antrum. This can be done in almost all cases, although a small amount of air must sometimes be insufflated so that one can see the direction to the antrum (i. e., rugal folds point towards the antrum). If this approach is taken, the stomach cannot be examined until after the duodenum has been examined and biopsied.Patients in which it is difficult to enter the antrum
Occasionally it becomes impossible to direct the tip of the endoscope into the antrum. This can be caused by the configuration of the stomach or because of abdominal viscera (e. g., an enlarged spleen) pushing into the stomach and diverting the tip of the scope as it travels along the greater curvature of the stomach. This usually occurs when scoping larger dogs. Repositioning the dog into dorsal recumbency while the scope is still in the stomach will usually allow the endoscopist to direct the tip of the endoscope into the antrum. Then, with the tip of the endoscope in the antrum, the dog is repositioned into left lateral recumbency so that the pylorus can be entered.
Intraoperative gastroduodenoscopy
Sometimes it is necessary to view the gastric mucosa during abdominal exploratory surgery to pinpoint lesions that cannot be identified from the serosal surface during laparotomy. For intraoperative endoscopy the patient is typically in dorsal recumbency, which sometimes makes it more difficult to enter the antrum and duodenum. However, the surgeon can help to direct the endoscope in such cases.
1.5.5
More on the topic Esophagogastroduodenoscopy:
- Esophagogastroduodenoscopy
- Indications
- Technique
- ENDOSCOPY
- Steiner J.M. (ed.). Small Animal Gastroenterology. Schluetersche,2008. — 387 p., 2008
- Contents
- Subject Index