Conditions oftheUvea
Uveitis
The most common acquired condition of the uvea is inflammation, referred to as uveitis. Anterior uveitis involves the iris and ciliary body; posterior uveitis affects the choroid and by natural extension the retina since the choroid and the retina are so intimately associated.
When both the anterior and posterior segments of the eye are involved, it is termed panuveitis. Intraocular inflammation is a non-specific response to a wide variety of insults and etiologies, ranging from trauma, to infectious or neoplastic disease (local or systemic), to immune-mediated conditions (Massa et al. 2002; van der Woerdt, Nasisse, and Davidson 1992). Typically when uveitis becomes chronic, it is because the primary insult has not been removed or eliminated or the condition is primary or perpetuated by an auto-immune assault.Acute uveitis typically presents with a degree of pain, manifested as blepharospasm, episceral injection, corneal edema, miosis, aqueous flare and sometimes with anterior chamber hyphema, fibrin or hypyon (Figure 4.28). Chronic uveitis will often result iniriscolorchange,usuallyhyperpigmentation,

Figure 4.28 Acute uveitis in a dog. Note the episcleral injection and miosis.
and may cause permanent scarring in the ocular interior.
When uveitis is diagnosed, symptomatic therapy should be initiated as soon as possible and a workup looking for causative or concurrent conditions should be performed. A thorough ophthalmic examination may reveal local disease such as the presence of cataract, which invariable results in lens- induced uveitis or an intraocular neoplasm, although the severity may vary considerably (Massa et al. 2002; van der Woerdt, Nasisse, and Davidson 1992). If no causative lesion is noted within the eyes, a thorough physical examination may reveal other sites of disease.
Survey labwork (complete blood count, serum biochemical profile, and urinalysis), along with serology for infectious agents common to the species or geographic locale and imaging of the thorax and abdomen may be necessary to elucidate an etiology. Cats should be tested for feline leukemia and feline immunodeficiency virus, even if they previously tested negative for the viruses when healthy, and possibly for exposure to feline coronavirus (if clinical signs and chemistry results support this) and toxoplasmosis. Auto-immune uveitis is a diagnosis of exclusion and every effort should be made to identify a cause in order to implement directed therapy.However, regardless of the cause, antiinflammatory therapy is critical to eliminate or minimize the damage that unchecked inflammation within the eye will cause (Zarfoss et al. 2010). Severe or chronic uveitis may result in corneal edema, vascularization and fibrosis, anterior and posterior synechia, cataract formation, the development of secondary glaucoma and, if the uveitis involves the posterior segment, retinal edema, detachment and degeneration (Figure 4.29). All of these lesions will affect ocular clarity and will negatively impact the potential for sight. Uveitis is also a profoundly painful condition. Anterior uveitis is best treated with topical medications. Steroids are generally more effective at addressing and controlling uveitis than are

Figure 4.29 Chronic uveitis in a cat. Note the iris color change, iridal neovascularization and cataract.
non-steroidal anti-inflammatory agents, however, care must be taken to choose a topical steroid preparation that will be capable of penetrating the cornea and acting within the eye. Prednisolone acetate is the preferred steroid for intraocular inflammation, because the acetate formulation allows for effective penetration. Dexamethasone is, of course, more potent than prednisolone, but its penetration is less.
Avoid hydrocortisone and sodium phosphate formulations of prednisolone. The frequency of delivery will depend upon the severity of the condition. Therapy should continue for at least one month following resolution of all clinical signs, but in most cases of chronic uveitis must be continued indefinitely with the goal of decreasing medication to the least amount necessary to keep the condition under control. Chronic topical steroids may result in impaired corneal healing and local immunosuppression and may result in crystalline deposits within the corneal stromal. For these reasons, controlled cases of chronic uveitis secondary to cataract (or following cataract removal surgery) may be switched to topical NSAIDs for maintenance therapy, which may be slightly safer for long-term use. Additionally, cases of anterior uveitis usually benefit from the application of a cycloplegic medication such as atropine which will help to stabilize the blood-aqueous barrier, dilate the pupil, which will minimize the development of synechia, and decrease ciliary spasm, which causes significant pain. Atropine, however, is contraindicated if the IOP is elevated as it may exacerbate IOP elevations.Posterior uveitis must be addressed with systemically administered anti-inflammatory or immunosuppressive medications since topicals alone will be insufficient to control posterior segment disease. Systemically administered steroids may suppress the inflammation, but are associated with untoward systemic side effects, so long-term therapy may be switched to immunomodulating agents such as cyclosporine, azathioprine, or leflunomide. Uveodermatologic syndrome, also known as VKH syndrome, is an example of an autoimmune panuveitis that requires systemically administered medications, as well as topical medications (Lindley, Boosinger, and Cox 1990; Yamaki and Ohono 2008) (Figure 4.30). This condition is most frequently encountered in the arctic breeds of dog and has a very high incidence of secondary glaucoma.
Cases of chronic uveitis should be monitored frequently (q2-6 months), even once seemingly well-controlled, for continued responsiveness and IOP trends.Pigmentary Uveitis in the Golden Retriever
Recently, a chronic form of primary uveitis has been described in the Golden Retriever breed (Sapienza, Simo, and Prades-Sapienza 2000). It is referred to as either pigmentary uveitis (PU) or Golden Retriever uveitis

Figure 4.30 Uveodermatologic syndrome in a Jack Russell terrier. This dog has severe uveitis and secondary glaucoma as well as lesions on the nasal planum.
(GRU) and is characterized by low-grade inflammation and pigment changes within the eye (Sapienza, Simo, and Prades-Sapienza 2000; Holly et al. 2015; Esson et al. 2009). The iris will often become hyperpigmented and there will be radially oriented deposits of pigment on the anterior lens capsule (Figure 4.31). Fibrin may accumulate in the anterior chamber and posterior synechia is common. Uveal cysts are often present, but their role in the disease has yet to be firmly established (Figure 4.32). Secondary glaucoma is common and may result in blindness in many, if not most patients over time. Signs of inflammation are generally confined to the anterior segment, but damage to the optic nerve and retina will occur once the IOP begins to rise. The condition typically progresses despite extensive topical and systemic therapy. Early diagnosis and intervention in the form of topical steroids and NSAIDs may slow changes but will not prevent them. Regular monitoring for IOP elevation is warranted.
Uveal Neoplasia
Uveal neoplasia may form as either a primary (local condition) or the result of a metastatic lesion. In most cases, the course of disease is rather short once it is recognized with uveitis
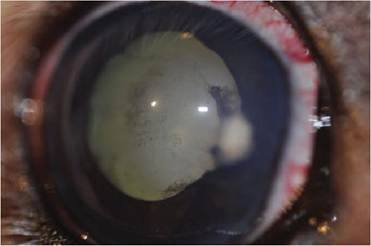
Figure 4.31 Pigmentary uveitis in the Golden Retriever.
Not the pigment deposition on the anterior lens capsule and the hyperpigmented iris.
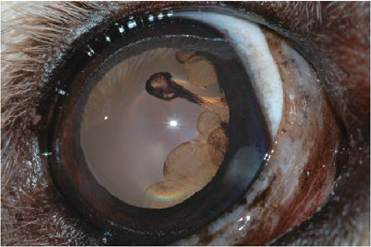
Figure 4.32 Uveal cysts in a Golden Retriever. This dog has no other active signs of pigmentary uveitis, but should be monitored closely.
and secondary glaucoma, usually necessitating removal of the globe. Most cases of intraocular melanoma develop as raised, nodular lesions arising from the iris or ciliary body. Feline diffuse melanosis and melanoma are the exceptions. Melanoma is the most common primary intraocular neoplasm in most species, but its appearance and behavior can vary. Cats may have a form that manifests as a progressive pigmentation of the iris which occurs over several months to several years (Kalishman et al. 1998; Acland et al. 1980) (Figure 4.33 and Figure 4.34). The pigmentation often develops simultaneously in several areas of the iris and over time will cause an increase in thickness of the iris and changes to the pupil shape and mobility. Eventually the tumor will invade the drainage apparatus and result in secondary glaucoma, but these changes often occur very slowly. The point at

Figure 4.34 Diffuse iris melanoma in a cat.

Figure 4.33 Diffuse iris melanoma in a cat.
which benign pigment cell proliferation on the surface of the iris transforms into invasive melanoma cells is difficult to define, which is problematic for prognostication and treatment recommendations. Once the tumor cells are in the iridocorneal angle and the scleral venous plexus, metastasis is likely, however (Kalishman et al. 1998). Frequent monitoring with photography of pigment progression and measurement of IOP is warranted until involvement of the angle, elevations of IOP or pupillary changes are noted or the client comes to terms with the prospect of enucleation (Acland et al. 1980).