Intraocular Disease
Glaucoma
Glaucoma is perhaps the most frustrating ocular disease for the practicing small animal veterinarian, client, and patient. It is an insidious disease that occurs in many breeds of dog (including mixed-breeds) and is associated with an increase in intraocular pressure (IOP) that is incompatible with the health of the eye.
Loss of vision results in time and the acute and sustained pressure spikes that occur are quite frequently very painful for the veterinary patient. Glaucoma is a leading cause of blindness in dogs, affecting approximately 2% of the canine population, and uncontrolled IOP can threaten life quality as a result of the discomfort that results (Gelatt and MacKay 2004a, 2004b).
Figure 4.22 Bilateral corneal edema in a Bichon Frise from endothelial degeneration.

Figure 4.23 This Boston Terrier has had bilateral keratectomies and Gunderson conjunctival flaps placed laterally in an attempt to minimize the progression and complications from endothelial decompensation.
Aqueous humor is essential to the health of the eye in that it functions to provide oxygen and nutrition to the avascular structures of the eye and acts as a waste sink for the products of metabolic breakdown. Aqueous humor is produced in the ciliary body by active secretion and ultrafiltration of plasma (Samuleson 2013). The enzyme carbonic anhydrase participates in the energy-dependent secretory phase of aqueous production. Most of the aqueous humor flows from the posterior chamber, through the pupil, to the anterior chamber, and exits at the iridocorneal angle into the intrascleral venous plexus. A small percentage of the outflow in dogs and cats, known as the uveoscleral or nonconventional pathway, exits through the iris, ciliary body, choroid, and sclera.
The balance between formation and drainage of aqueous humor maintains IOP within a normal range of approximately 15 to 25 mmHg. Due to conformational differences, brachycephalic animals tend to have slightly higher IOPs than mesocephalic and dolichocephalic individuals, hence the wide range. With most modern instruments for estimating IOP, the normal IOP is in the low to middle teems.Glaucoma is a set of diseases that all have the common risk factor of IOP elevation. Essentially increased IOP with associated visual deficits due to damage to and death of the retinal ganglion cells and their axons are the hallmarks of the disease. IOP-independent alterations such as excitotoxic amino acids, defects in the optic nerve head microcirculation, and extracellular matrix abnormalities of the iridocorneal angle and optic nerve may also contribute to damage in glaucoma. In most cases in dogs and cats, glaucoma is caused by obstruction or stenosis of the aqueous humor outflow pathways. It remains a challenge to the veterinarian to detect the early subtle disturbances of glaucoma and to effectively treat this condition. Delayed or inadequate therapy can lead to irreversible blindness and a painful, cosmetically unacceptable eye.
When a patient presents with a painful, red eye, glaucoma should be ruled out among the possible diagnoses of conjunctivitis, uveitis, or keratitis. Pain may manifest as depression, anorexia, rubbing at the eye, or squinting. However, in chronic cases wherein the patient has had time to acclimatize to the IOP elevation, overt signs of pain or discomfort may be absent. All ocular tissues are affected by an elevated IOP. Clinical signs include a “red eye,” the result of congestion of episcleral vessels, corneal edema, mydriasis, blepharospasm, blindness, and buphthalmos (Figure 4.24). With the exception of buphthal- mos, which is a finding in the chronic condition, the remainder of these clinical signs may occur at any stage of glaucoma (Figure 4.25).
Pupillary light reflexes may be normal, slow, or absent in early glaucoma, depending on the functional status of the iris sphincter muscle, retina, and optic nerve and the IOP. Acute elevations of IOP above 45 mm Hg cause paralysis of the iris sphincter muscles and subsequent mydriasis. Buphthalmos, or enlargement of the globe, may occur more rapidly in young dogs and cats, due to the elastic nature of young globes. Rupture of the cornea's Descemet's membrane may accompany elevated corneal tension and buphthalmos to produce multiple, linear corneal striae. Persistent corneal
Figure 4.24 Acute glaucoma in a dog. Note the episcleral injection, corneal edema and mydriasis.
endothelial damage can result in permanent corneal edema. Buphthalmos causes increased tension on the lens zonules, which in turn can result in zonular disinsertion and lens subluxation or luxation. Prolonged or recurrent elevations of IOP lead to degeneration of the retina and optic nerve, with cupping or atrophy of the optic nerve head. The onset of clinical signs of glaucoma in cats is often insidious, as this species is less likely to demonstrate the acute intense corneal edema and episcleral congestion exhibited by dogs. Clinical signs of the glaucomas depend on the stage of disease and, to some extent, on the type of glaucoma. The signs of glaucoma may be asymmetric in the same patient, with different stages occurring in different eyes. The signs of the secondary glaucomas are like those of the primary glaucomas, but clinical signs of the antecedent etiology, such as an anterior uveitis, an intraocular mass, or a lens luxation, will be present as well. The congenital glaucomas affect young animals, usually within the first 3 to 6 months of life. Often, the first clinical sign in these animals is rapid onset of buphthalmia and lagophthalmos, or the inability to completely close the palpebral fissure.
A diagnosis of glaucoma is made based upon clinical signs and an index of suspicion for the disease. It can be confirmed or supported with tonometry, or an estimate of IOP that is above the reference range of normal. Tonometry in the outpatient clinic provides only a “snapshot,” and diurnal variations in IOP occur, but it is the easiest way to monitor the progression and response of the disease. In the dog, the higher levels occur in the early morning and the lowest readings in the early evening. The most common tools for tonometry in the veterinary clinic are the TonoPen, an applanation tonometer that measures the amount of force necessary to indent a fixed surface area of the cornea, and the TonoVet, a rebound tonometer that measures the rebound force and velocity that a pin returning from contacting the cornea has (von Spiessen et al. 2015; Gorig et al. 2006). Both instruments have similar accuracies and the choice of which to use is mostly based upon clinician preference. IOP must be accurately measured to diagnose and monitor glaucoma.
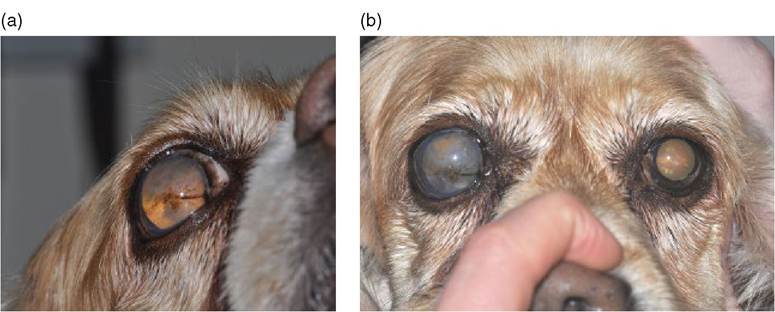
Figure 4.25 a and b Chronic glaucoma in a Cocker Spaniel. Note the buphthalmos, corneal edema, fibrosis and pigmentation. The tapetal reflection is bright, indicating likely retinal degeneration secondary to chronic elevations of IOP or segmental vascular infarcts.
Types of Glaucoma
Glaucoma is classified on the basis of the probable cause, the appearance of the drainage angle and the stage or duration of the condition (Gelatt and MacKay 2004a, 2004b) (Table 4.3). In the primary glaucomas, there is an inherited anatomic or functional defect in drainage of the aqueous humor in the absence of concurrent ocular disease (Komaromy and Petersen-Jones 2015). It is common in some breeds of dog and is always bilateral, although development of clinical
disease is usually asymmetric (Table 4.1). Siamese cats also have an inherited form of primary glaucoma (Dietrich 2005).
In the secondary glaucomas, the increase in IOP is associated with some known antecedent or concurrent ocular disease that results in physical obstruction of an outflow pathway (Gelatt and MacKay 2004b; Johnsen, Maggs, and Kass 2006). These cases are not inherited and may be unilateral or bilateral, depending upon the presence of the underlying condition in each eye. Many of the conditions that initiate these forms of glaucoma may be genetically determined in certain breeds, such as cataract or zonular dysplasia (lens luxation). The secondary glaucomas are nearly as prominent in the canine population as are primary forms, so making the distinction between the two forms is critical. Clinical management of the secondary glaucomas, however, is often more clear-cut, because the cause of the increased IOP can usually be ascertained and the prognosis for development of glaucoma in the non-affected eye is clear. Secondary glaucoma may be initiated by uveitis, cataract development and its resultant uveitis, lens luxations, or intraocular neoplasia (Figure 4.26 and Figure 4.27). Medical or surgical treatment of the secondary glaucomas is directed toward removing, if possible, the cause of the elevated IOP. Secondary glaucoma is by far more common in cats than is primary glaucoma. Congenital glaucomas are rare in dogs and cats and usually occur due toTable 4.3 Types of Glaucoma.
| Primary | Secondary Congenital |
| Open/normal angle Narrow/closed angle | Uveitis Anterior segment Lens luxation dysgenesis Lens-induced (chronic cataract, intumescent cataract, phacolytic uveitis, phacoclastic uveitis) Hyphema Intraocular neoplasia Pigmentary/melanocytic proliferation |

Figure 4.26 Secondary glaucoma in a dog. Note the episcleral injection, peripheral corneal vascularization, and edema.
The pupil is mid-range, which is commonly noted when uveitis is present concurrently.

Figure 4.27 Chronic lens-induced uveitis has resulted in considerable intraocular damage, including 360 degree posterior synechia.
developmental abnormalities of the aqueous humor outflow pathways. The extent of the angle anomaly may affect the time of onset for the elevation of IOP. The more severe the defect, the sooner the elevation in IOP occurs.
Therapy for Glaucoma
There is no cure for glaucoma unless the condition is secondary and the initiating condition or insult can be removed or corrected promptly. The goals of therapy are retention of vision as long as possible and elimination of pain, since glaucoma can cause remarkable discomfort when IOP elevation is uncontrolled. Glaucoma is a progressive condition and requires regular and frequent monitoring to determine if current medical therapies are sufficiently controlling IOP.
IOP is the primary risk factor in glaucoma and the easiest aspect of the disease to monitor, therefore it has become the main target of therapy (von Spiessen et al. 2015; Gorig et al. 2006). In general, it is desirable to achieve the “target” or “safe” IOP for each canine eye that is at or lower than the bottom of the reference range of normal IOP. An IOP reduction to levels that decrease retinal ganglion cell (RGC) loss from glaucoma to normal, age-related levels is usually lower than what would be considered a normal IOP in a normal animal. To achieve this reduction of IOP, a means of either decreasing the production of aqueous humor or increasing the outflow or drainage of fluid from the eye must be found. It is critically important that “prophylactic” therapy be initiated in the normotensive fellow eye when primary glaucoma has been diagnosed in one eye, since studies have demonstrated that early therapy in the normotensive eye may delay the onset of IOP elevation for a considerable amount of time (up to a mean of 30 months) (Miller et al. 2000). In secondary glaucoma, the inciting cause is identified and either removed or suppressed and anti-hypertensive medical therapy is usually indicated concurrently.
Both medical and surgical options for glaucoma therapy are available, however, as with any condition that has a multitude of treatment options, there exists no single gold standard treatment (Table 4.4). Therapy should be individualized and will change as the stage of the disease advances and whether or not vision is still present. Medical therapy for the narrow- and closed-angle glaucomas is usually short term when employed alone, because eventually, the outflow becomes so impaired that effects of drugs become inadequate. Some clinical studies suggest that there are higher long-term success rates for controlling IOP and maintenance of vision if surgery is performed earlier in the glaucoma process (Gelatt and MacKay 2004a;
Table 4.4 Treatment of Glaucoma.
| Control stage | Treatment |
| Initial control | IV mannitol (1-2 g/kg IV) or Glycerine (1-2 g/kg PO) Prostaglandin analogues (SID-BID) (in the absence of uveitis or lens luxations) Aqueocentesis (when medical therapies fail to lower IOP) Address concurrent or causative ocular condition (when glaucoma is secondary) Initiate topical maintenance medications in affected and fellow eye |
| Short-term control | Beta-blockers or other adrenergics (BID-TID) CAIs (topical dorsolamide or brinzolamide BID-TID) Prostaglandin analogues (SID-BID) Neuroprotective drugs - memantine, amlodipine Laser cyclophotocoagulation Gonioshunt |
| Long-term control | Laser cyclophotocoagulation Gonioshunt Supplement with medical control |
| Salvage control | Enucleation Evisceration with intraocular prosthesis Chemical ciliary body ablation |
Miller et al. 2000; Sapienza and van der Woerdt 2005; Hardman and Stanley 2001).
In most cases, multiple drug therapy to decrease IOP by reducing production of aqueous humor and diminishing the resistance to aqueous humor outflow will be necessary, even if surgical options are pursued. B eta-adrenergic antagonists, such as timolol and betaxalol, act by decreasing production of aqueous humor (Plummer, MacKay, and Gelatt 2006). Although the exact mechanism by which it is decreased is unknown, and will lower IOP only a few millimeters, therefore they are not good single agent drugs for the control of IOP in eyes that have documented elevations (Plummer, MacKay, and Gelatt 2006). They do, however, work synergistically to lower IOP even greater than the additive effect would be when used in combination with carbonic anhydrase inhibitors (Plummer, MacKay, and Gelatt 2006). They are also inexpensive options for prophylactic therapy of the fellow eye that has not yet developed ocular hypertension. Carbonic anhydrase inhibitors (methazolamide, acetazolamide) reduce ciliary body production of aqueous humor (Gelatt and MacKay 2001a). These drugs when given systemically can cause metabolic acidosis, and the dosage should be carefully adjusted to minimize side effects, which include panting, nausea, and vomiting. Topical formulations (dorzolamide, brinzola- mide) have been developed that do not typically cause these untoward side effects and are more efficacious at lowering IOP (Plummer, MacKay, and Gelatt 2006; Gelatt and MacKay 2001a). These drugs make up the mainstay of chronic medical therapy for glaucoma and may be formulated in combination with a beta-blocker drug. Prostaglandin analogues (latanaprost, bimatoprost) decrease IOP by increasing the percentage of aqueous humor outflow through the uveoscleral or unconventional drainage pathway (Gelatt and MacKay 2001b). These drugs have become a go-to for emergency treatment of severe hypertensive episodes. In many instances, they will lower IOP abruptly within 15-30 minutes. However, they may exacerbate any uveitis present and will result in profound miosis that may make examination of the posterior segment difficult or impossible. They should not be used when anterior lens luxations are present since the miosis that results behind the lens can cause a condition called malignant glaucoma wherein the IOP rises due to further occlusion of aqueous drainage. Topical parasympathomimetic drugs (pilocarpine, demecarium bromide) act primarily to cause ciliary muscle contraction, increasing the outflow of aqueous humor (Gelatt et al. 1983). This action is independent of their effect on the iris sphincter muscle. Parasympathomimetics are contraindicated in glaucoma associated with anterior uveitis and they should be used with caution in glaucoma associated with anterior lens luxations. These drugs are not single agent treatments since they do not lower IOP dramatically and are most often used to augment therapy already instated. Sympathomimetic drugs (dipivefrin, brimonidine) reduce IOP by increasing production of aqueous humor and increasing outflow (Gelatt et al. 1983; Gelatt and MacKay 2002). These drugs, too, are not employed as single agents and are most effective in reducing IOP when combined with parasympathomimetics. Brimonidine may have some neuroprotective effects (Gelatt and MacKay 2002).
Oral and intravenous hyperosmotic agents (mannitol, glycerin) lower IOP rapidly by osmotically reducing the volume of the vitreous (Dugan, Roberts, and Severin 1989). They are used in the emergency treatment of acute glaucoma but are ineffective or impractical for long-term or maintenance therapy.
Intravitreal glutamate levels are elevated in canine glaucoma. Glutamate is extremely toxic to the retinal ganglion cells, resulting in their overstimulation. Glutamate excitotox- icity is mediated by intraneuronal calcium influx. Intraneuronal homeostatic imbalance induces apoptosis and cell death (Almasieh et al. 2012). The use of glutamate receptor antagonists (memantine) and calcium channel blocking drugs (amlodipine) for neuroprotection is being studied and may become standard care in the future.
Since glaucoma once established (any primary cases and many secondary cases if the damage is considerable or the primary cause has not been eliminated) is a progressive condition, frequent and diligent monitoring is necessary. It is generally recommended that “stable” patients have their IOP measured every 2-3 months in perpetuity.
Surgical Treatment for the Glaucomas
With the narrow-angle and angle-closure glaucomas in dogs, surgical treatment is recommended early (Gelatt and MacKay 2004a; Sapienza and van der Woerdt 2005; Hardman and Stanley 2001; Almasieh et al. 2012). Medical treatment usually provides a few months of effective IOP control. Surgical intervention is recommended to augment the effects of medical therapy, however, these will neither cure nor prevent the possibility of progression. Anterior chamber shunts (i.e., gonioimplants) and laser cyclophotocoagulation appear to offer the longest periods of successful IOP control (Sapienza and van der Woerdt 2005; Hardman and Stanley 2001; Almasieh et al. 2012; Westermeyer, Hendrix, and Ward 2011; Bras, Robbin, and Wyman 2005). Targeted laser ablation with the aid of endoscopic visualization may improve our ability to decrease aqueous humor production and lower IOP for longer periods of time (Bras, Robbin, and Wyman 2005). If the glaucoma is secondary in origin, surgical therapy will be aimed at removing the offending cause (i.e., lens extraction with luxated or subluxated lenses).
Treatment for Blind, End-Stage Glaucoma
Salvage procedures to prevent ocular pain, to reduce the enlarged and blind globe to nearnormal size, and to provide a cosmetically acceptable eye include pharmacologic destruction of the ciliary body with intravit- real injection of gentamicin, intraocular prosthesis, in which a silicone ball is placed in an eviscerated globe, and enucleation (i.e., surgical removal of the globe).