Lenticular Changes
Nuclear Sclerosis
Nuclear sclerosis is a consistent finding in dogs older than 7 years that occurs from progressive lens fiber formation and internal
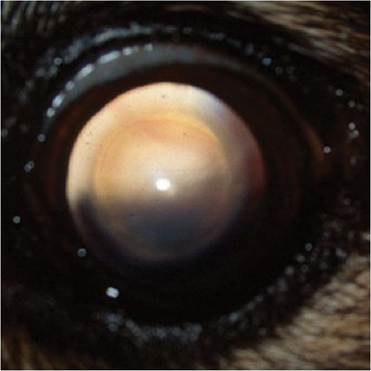
Figure 4.35 Nuclear sclerosis in a middle aged dog.
Note the homogenous spherical structure in the central lens and the unobstructed tapetal reflex.compression of older lens fibers, especially those in the lens nucleus (Samuleson 2013). The change is associated with senescence and alters the optical properties of the compressed central lens fibers causing lightscattering. The result is a clinically apparent, whitish-blue or gray appearance to the nucleus on diffuse illumination of the lens. Distant diffuse illumination, however, will reveal an intact and normal tapetal or fundic reflex (Figure 4.35). The nucleus will appear as a clear, homogenous circular ring in the axial lens. Visual examination of the fundus via direct or indirect ophthalmoscopy is possible through the central lens, except in the most severe of examples in which there may be a subtle decrease in fine detail. In contrast, early or immature cataracts appear as dark structures with distant retroillumination or as irregular opacities that typically obscure visualization of the fundus. The patient's functional sight is not typically significantly affected when nuclear sclerosis develops, although depth perception may be affected in older animals or in those who participate in speed and agility competition (Murphy, Zadnik, and Mannis 1992).
Cataract
Cataracts classified as “senile” or “age-related” are commonly seen in the aged dog. They are typically classified as senile if no other antecedent etiology is known or apparent. The age of onset at which a cataract should be considered to be age related is arbitrary (usually greater than 6-7 years of age) and related to the breed.
It was reported in one study, however, that all dogs over 13 years of age had some degree of cataract formation (Williams, Heath, and Wallis 2004). The clinical appearance and progression rate of age-related cataracts can vary, but they often appear as punctate or linear opacities in the axial lens concurrent with or after the development of nuclear sclerosis. Cortical cataractous changes, often in a wedge or spoke pattern in the peripheral lens, may also occur to varying extents.Other etiologies of cataract in the dog include heredity (by far the most common cause of cataract development in canines), diabetes mellitus, and intraocular disease, such as uveitis or glaucoma (Williams, Heath, and Wallis 2004; Gelatt and Mackay 2005; Basher and Roberts 1995; Oberbauer et al. 2008). In cats, the majority of cataracts are secondary to uveitis or some other intraocular condition (Stiles 2013). Inherited cataracts and metabolic cataracts do occur sporadically in cats, but not nearly with the frequency of uveitis cataracts (Stiles 2013). Thorough physical and ophthalmic examinations and minimum data base collection should be performed to look for potential underlying systemic or metabolic disease when a diagnosis of cataract has been made.
If an owner is interested in cataract removal surgery for their pet, an early referral to a veterinary ophthalmologist should be made in order to determine eligibility for surgery and to counsel the owners about the pre- and post-operative requirements of cataract surgery. Patients that have had cataract removal surgery will require regular examinations of the eyes and intraocular pressure monitoring and often topical medical therapy for the rest of their lives. Patients that are not candidates for cataract removal, will also require regular eye examinations. Cataracts invariably initiate the development of uveitis, often referred to as lens-induced uveitis (LIU), which can result in either subclinical or overt and severe clinical signs (van der Woerdt, Nasisse, and Davidson 1992; Wilcock and Peiffer 1987).
If left untreated, many cataractous eyes will develop synechia (adhesions of the iris to the lens or the peripheral cornea) and preiridal fibrovascular membranes which interfere with normal drainage of aqueous humor with subsequent elevation of intraocular pressure and eventual overt secondary glaucoma (Zarfoss et al. 2010; Wilcock and Peiffer 1987). Topical therapy with steroidal or nonsteroidal anti-inflammatories is necessary to prevent or delay the consequences of LIU. Diligent monitoring of IOP, as well as for the signs of anterior uveitis, is strongly recommended at least 2-3 times annually.Lens Luxations and Subluxations
Lens luxations develop due to an inherited dysplasia of the zonules that suspend the lens in its normal location or secondary to chronic inflammation or another insult that is damaging to these zonules (Gould et al. 2011; Morris and Dubielzig 2005). Lens luxations in the terrier breeds and some others are common due to zonular dysplasia, and these dogs may present with either unilateral or bilateral and acute or chronic secondary glaucoma (Table 4.1). The glaucoma is either associated with the iridocyclitis that results from microtrauma between the unstable lens and iris, with resultant increases of aqueous humor fibrin, proteins, and inflammatory cells, which can clog the drainage apparatus

Figure 4.37 Lens subluxation in a mixed-breed dog. Note the dorsolateral aphackic crescent.

Figure 4.36 Anterior lens luxation of a clear, non- cataractous lens in a Chinese Crested dog.
Figure 4.38 Posterior lens luxation in a dog.
and contribute to the formation of preiridal fibropupillary membranes and synechiae or due to mechanical impairment of aqueous humor passage through the pupil by and anteriorly luxated lens (Wilcock and Peiffer 1987).
A completely luxated lens can remain in the patella fossa, luxate into the anterior chamber, or move posteriorly through the torn anterior vitreal face and into the vitreous (Figure 4.36, Figure 4.37, Figure 4.38, and Figure 4.39). A large number of animals with partial or complete lens luxations, both anterior and posterior, will develop glaucoma (Gelatt and MacKay 2004b; Dietrich 2005; Johnsen, Maggs, and Kass 2006; Glover et al.

Figure 4.39 Anterior lens luxation of a mature cataract in a cat. Note the iridal neovascularization that had adhered to the nasal aspect of the lens. This luxation was secondary to chronic uveitis.
1995). Regardless of the direction of lens displacement, anterior uveitis is invariably present and is one of the targets of medical therapy. When a patient presents with anterior lens luxation, the displaced lens will in many cases be in contact with the corneal endothelium resulting in focal edema. If there is significant elevation of IOP or moderate to severe uveitis, there may be diffuse corneal edema. It may be difficult to accurately assess IOP with the lens in such close proximity to the cornea. Care should be taken not to indent the cornea so that it presses into the lens; the IOP in that case may be falsely elevated.
Early removal of displaced lenses, particularly in Terriers, has the highest possibly of success for retention of vision and prevention of secondary glaucoma (Gelatt and MacKay 2004b; Dietrich 2005; Johnsen, Maggs, and Kass 2006; Glover et al. 1995). The primary objective of lens extraction is to prevent or treat secondary glaucoma and to diminish inflammation. Early referral to a veterinary ophthalmologist for counselling and surgical therapy is recommended. Medical therapy should consist of topical anti-inflammatory medications (prednisolone acetate 1%, dexamethasone 0.1% q6-12h; or an NSAID if the cornea is compromised) and topical anti-hypertensive medications, depending upon the measured IOP. In some cases of posterior lens luxation or subluxation when surgery is not possible or is declined, it may be helpful to use a miotic agent such as demecarium bromide to prevent anterior movement of the lens (Binder, Herring, and Gerhard 2007). Due to the high risk of secondary glaucoma, these patients should be monitored regularly for elevations in IOP (q2-6 months).