Congenital Cardiovascular Disease
The cause of congenital cardiac defects has not been established, although hereditary factors may be responsible for some defects. In humans, additional factors such as maternal infection, age, and nutritional status have been identified; fetal anoxia from placental insufficiency, fetal infection or metabolic dysfunction, or other causes may contribute to the development of congenital cardiac defects.
The same factors may apply in animals. Congenital cardiac defects in large animals can occur alone or in combination. The most commonly reported is VSD.25,39,51-54 Multiple cardiac anomalies including PDA,55,56 tetralogy of Fallot,57,58 truncus arteriosus,59,60 total anomalous pulmonary venous connection,61 and Eisenmenger complex in calves62 have been reported. Congenital anomalies of the tricuspid,59,63-65 mitral,66 and pulmonic valves59,67,68 are uncommon. Congenital abnormalities of the aorta are reported in calves and foals but are also uncommon.54,69,70 ASD occurs more commonly in calves than in foals and is frequently accompanied by other defects.54,60,71,72 Hypoplasia of the left and right ventricles has been infrequently reported in calves and foals.54,73,74Congenital cardiovascular disease should be suspected in a young patient if examination reveals a holosystolic (pansystolic), holodiastolic, or continuous murmur or a murmur with a palpable thrill or wide radiation over the thorax. Cyanosis at rest or with exercise in a patient with a cardiac murmur warrants consideration of a right-to-left cardiac shunt, obstructive pulmonary disease, or severe stenosis of the structures of the right side of the heart. The presence of any of these findings in a young animal with a history of lethargy, weakness, or failure to thrive constitutes grounds to suspect congenital cardiovascular disease.
Ventricular Septal Defect
DEFINITION AND ETIOLOGY. A VSD is an opening in the interventricular septum that creates communication between the left and right ventricles. In large animals most defects occur in the perimembranous septum and are imaged ventral to the right and/or noncoronary cusp of the aortic valve and cranioventral to the septal leaflet of the tricuspid valve, including or adjacent to the fibrous part of the interventricular septum.25,39,52,54 VSD can occur as a single defect or as part of a complex anomaly. Many cardiac malformations such as tetralogy and pentalogy of Fallot, truncus or pseudotruncus arteriosus, common atrioventricular canal defect, tricuspid atresia, and double outlet right ventricle include a VSD. The cause of VSD is unknown, although it has been documented to be a heritable defect in Limousine54 and possibly Hereford75 cattle. VDSs are more common in Welsh Mountain ponies (Section A) and in the Arabian, Standardbred, and Quarter Horse breeds, suggesting a possible hereditary predisposition.76,77 The defect is thought to result either from failure of fusion of a part of the endocardial cushion and the muscular ventricular septum or failure of fusion of the truncal and conal septa.78
Clinical Signs and Differential Diagnosis
The clinical signs of an isolated VSD vary and depend on the size of the defect, direction of the shunted blood, and presence of concurrent valvular or myocardial disease. In isolated VSD the blood flow is shunted from the left ventricle to the right ventricle through the defect in the interventricular septum. The size of the shunt depends on the size of the defect and the pressures in the left ventricle, right ventricle, and pulmonary artery.
VSD is suspected when there is a loud, grade ≥4 to 6/6 harsh, plateau-shaped pansystolic murmur with its point of maximal intensity (PMI) in the tricuspid valve area and a slightly softer (usually one grade softer), more crescendo-decrescendo holosystolic murmur that is loudest in the pulmonic valve area.
The murmur on the left side has its PMI in the pulmonic valve area, associated with a relative pulmonic stenosis (increased blood flow across a normal pulmonic valve). Occasionally there is splitting of the second heart sound. The murmur may be the only clinical sign identified if the defect is small or moderate size. On the other hand, poor growth, lethargy, dyspnea, exercise intolerance, and signs of CHF can be exhibited by animals with a large VSD. This usually develops by the time the animal is 5 years old. CHF may develop later in horses with a moderatesized VSD and cardiomyopathy or in those with a moderate to large VSD with aortic prolapse who then develop aortic regurgitation (AR). Occasionally there is a diastolic murmur of aortic insufficiency associated with a large VSD, the location of which compromises the support of one of the aortic valve cusps.10,25,53 Cardiac arrhythmias, particularly AF, may be associated with VSD when there is cardiac enlargement or failure. The development of AF may be the “tipping point” for the development of congestive heart failure.If the systolic murmur is loudest on the left side of the thorax, a subpulmonic VSD or a complex anomaly with pulmonic stenosis (or some form of right ventricular outflow tract [RVOT] obstruction) should be suspected.10,25,53,79 The pulmonic murmur is usually louder than the tricuspid murmur in large animals with tetralogy of Fallot. Large animals with tetralogy of Fallot may have cyanosis at rest (uncommon in horses) or with exercise or exertion. Cyanosis is also a distinguishing feature of Eisenmenger complex, a defect in which right-sided heart resistance to blood flow causes the shunt associated with VSD to become right to left (which is rare). Congenital abnormalities of the mitral and tricuspid valves (dysplasia) cause a loud systolic murmur audible on both sides of the thorax but are rare. The PMI of the left-sided systolic murmur is more caudally located (in the mitral to aortic valve area) than the relative pulmonic stenosis murmur.
Usually the murmur of mitral regurgitation (MR) is louder than the murmur of tricuspid regurgitation (TR). An innocent flow murmur of neonates can usually be distinguished from VSD by its crescendo-decrescendo shape, PMI at the left heart base, lack of radiation, and low to moderate intensity.Clinical Pathology
Echocardiography is the diagnostic technique of choice for identifying a VSD. With 2D echocardiography the VSD can be imaged directly (Fig. 30.5, A) and the shunt size, location, and direction demonstrated with color-flow Doppler echocardiography (Video 30.1) or the injection of microbubbles. Maximal shunt velocity is obtained with continuous-wave Doppler echocardiography (Fig. 30.5, B). Careful scanning of the interventricular septum should be performed with 2D echocardiography to directly image the VSD and measure its maximal diameter in two mutually perpendicular planes.10,25,53 The typical perimembranous VSD (≤2.5 cm in both planes) is missed if the long-axis view of the left ventricular outflow tract (LVOT) is not examined. The membranous VSD is located underneath the right and/or noncoronary leaflet of the aortic valve and ventral to the septal leaflet of the tricuspid valve. If a perimembranous defect is not found, the entire septum should be carefully scanned in all imaging planes to detect the VSD. The subpulmonic location, more common in calves, is easy to miss. This defect is usually best imaged in the short-axis view, scanning the interventricular septum between the LVOT and RVOT. With a left-to-right shunt a high-velocity turbulent jet is depicted from the right parasternal window, originating in the left ventricle, traversing through the defect in the interventricular septum into the right ventricle with color-flow Doppler echocardiography (Video 30.1), whereas a negative contrast jet is imaged in the right ventricle with a right-sided injection of microbubbles.10,25,53 Moderate to large VSDs show left atrial and left ventricular enlargement, right ventricular enlargement, and pulmonary artery dilation.
The left atrial- to-aortic root ratio is increased. Aortic valve prolapse and AR may also be detected because of loss of support of the aortic root from the VSD, more likely with larger VSDs and VSDs with malalignment of the ascending aorta with the upper portion of the interventricular septum. Myocardial dysfunction and subsequent CHF may occur with a large VSD. Most horses with VSDs that are compatible with a normal life expectancy ultimately develop MR secondary to the chronic left atrial and ventricular volume overload. Continuous-wave Doppler echocardiography should be used to noninvasively assess the hemodynamic significance of the shunt (see Fig. 30.5, B). A peak shunt flow velocity of 4.5 m/s or greater indicates a restrictive VSD with normal or near-normal right ventricular pressures.77 The radiographic presence of cardiomegaly and increased vascularization of the lungs provide only nonspecific evidence of VSD. If polycythemia is found, a complicated VSD should be suspected.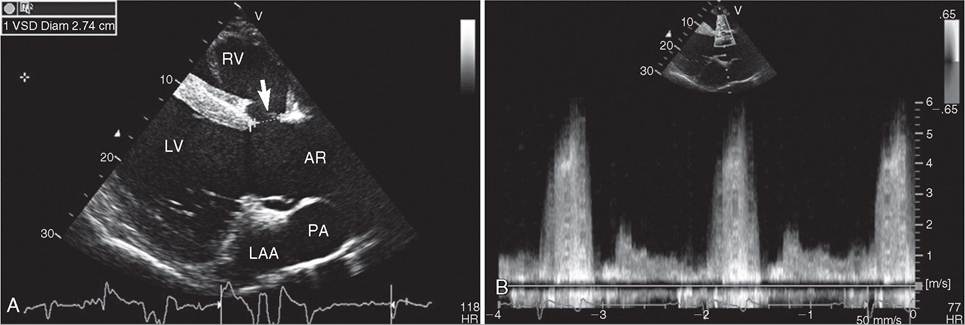
FIG. 30.5 Two-dimensional echocardiographic image (A) and continuous-wave Doppler spectral tracing (B) of a ventricular septal defect (VSD) (arrow) in a Thoroughbred gelding who presented for poor racing performance. The VSD is located just underneath and cranial to the septal leaflet of the tricuspid valve and just ventral to the noncoronary and right coronary cusp of the aortic valve and measured 2.74 cm in this view. There is significant left ventricular enlargement in this gelding. The right ventricle (RV), left ventricle (LV), left atrial appendage (LAA), aortic root (AR), and pulmonary artery (PA) are all visible in this view. The spectral tracing shows a peak shunt velocity of over 5 m/s in systole. Some turbulent flow (spectral broadening) is also detected in diastole, with a peak flow velocity of approximately 1.75 m/s.
Cardiac catheterization can be used for qualitative and quantitative assessment of the VSD but has been supplanted by echocardiographic diagnosis.
Elevated cardiac pressures provide qualitative evidence of a VSD. Right ventricular systolic pressure elevation is most common and may equal left ventricular pressure with a large VSD. Pulmonary artery pressure (PAP) can be increased as a result of increased blood flow from the left-to-right shunt or increased pulmonary vascular resistance and decreased flow (restrictive pulmonary hypertension). Elevation of left or right ventricular diastolic pressure provides evidence of cardiac failure in the patient with VSD. Oximetric data (oxygen content or oxygen saturation) can be used to locate the shunt and provide some evidence of the size of the defect. A step-up in oxygen content or saturation between the right atrium and the pulmonary artery suggests a moderate or large VSD. Because most VSDs are located high in the RVOT, there may be inadequate mixing of shunted blood in the right ventricle to detect the shunt in this chamber, unless the catheter is directed to the outflow tract for sampling. When the oxygen step-up is detected first in the pulmonary artery, a PDA cannot be ruled out. A small shunt may be missed by oximetry as described earlier under oxygen sampling.By using the indicator dilution methods described previously, the shape of the concentration-time or temperature-time curve can be used to demonstrate the left-to-right shunt of a VSD. A comparison of the cardiac output measured in the right ventricle with the cardiac output measured in the pulmonary artery can give an estimation of the percent of pulmonary blood flow coming from shunted blood and therefore an estimation of the size of the defect.40
Angiocardiography in the anesthetized neonate can definitively demonstrate VSD if there is simultaneous opacification of the left and right ventricles when dye is injected into the left ventricle but has been supplanted by color Doppler echocardiography.
Pathophysiology
A small VSD may provide enough resistance to flow that the left-to-right shunt is minimal and the patient remains asymptomatic. Horses can race successfully with small VSDs (≤2.5 cm in diameter with peak shunt velocities ≥4.5 m/s), although they are not usually successful as elite racehorses.10,25,77 In smaller horses and ponies or very large horses, a VSD-to- aortic root ratio less than 0.3 is unlikely to be hemodynamically significant.76,77 Most horses in this study that presented with CHF or exercise intolerance had a VSD-to-aortic root diameter of 0.64.76 VSDs produce a left-to-right shunt because the pressure in the left ventricle exceeds that in the right ventricle. A peak shunt velocity of 3.5 to 4.5 m/s indicates an increased right ventricular pressure and a less restrictive VSD, but the defect is usually compatible with a normal life expectancy. A peak shunt velocity less than 3.5 m/s is indicative of a large shunt that is hemodynamically significant. These animals usually develop CHF by 5 years of age. Occasionally the VSD is so large that the pressure between the two chambers is equalized. The right ventricle, pulmonary circulation, left atrium, and left ventricle must compensate for this volume overload, which generally results in dilation of cardiac chambers and development of pulmonary hypertension.
Simultaneous pulmonary disease or left-sided heart failure due to chronic volume overload can increase pulmonary vascular resistance. In addition to volume overload, the right ventricle is subjected to a chronic pressure overload that may be sufficient to reverse the direction of the shunt (Eisenmenger complex, more common in cattle). Because of the pressure and volume overload with moderate to large VSDs, patients with this condition run a greater risk of developing CHF.
Considerable turbulence associated with left-to-right shunts and endocardial damage increase the risk of endocarditis in patients with VSD.80 Because the VSD is usually located high in the LVOT, structural support of the aortic valve cusps may be lost, especially with large VSDs and/or malalignment VSDs, and AR may develop.10,25,77 Significant AR adds to the left ventricular volume overload caused by the VSD.
Epidemiology
The true incidence of VSD in large animals is unknown, although it is recognized as the most common congenital cardiac defect. In one study, 36 calves had 78 congenital cardiac defects, of which 11 were VsDs.54
Necropsy Findings
VSD is usually located high in the interventricular septum just ventral to the right or noncoronary cusp of the aortic valve in the left ventricle and underneath the septal leaflet of the tricuspid valve or caudal or ventral to the crista terminalis in the right ventricle.77 It can be an isolated defect or accompanied by other cardiac or organ anomalies. If the defect is moderate or large, there is right ventricular, left atrial, and left ventricular enlargement and pulmonary artery dilation. Increased pulmonary blood flow can lead to lung congestion and secondary pneumonia is not uncommon. If pulmonary vascular resistance is increased, right ventricular hypertrophy may be present. There may be secondary endocarditis (infrequent in large animals)80 or endocardial lesions as a result of turbulent blood flow across the defect.
Treatment and Prognosis
There is no practical treatment for VSD in large animals. A complete echocardiographic examination is indicated to identify the presence and significance of a VSD. The size of the VSD, peak shunt velocity through the VSD, degree of left atrial and left ventricular volume overload, presence of aortic valve prolapse, detection of AR or MR, and myocardial function all have to be assessed to determine the VSD's significance. It is important to identify those animals with moderate to large defects, because the prognosis for normal production or function is poor. Horses with large defects (>3.5 cm or VSD/aortic root ratio of 0.64) and peak shunt velocities through the defect of less than 3.5 m/s are likely to develop CHF early in life and have a shortened life expectancy.25,76 These horses are not suitable for use by a child or in a lesson program. Animals with small defects may remain asymptomatic throughout life. Rarely, spontaneous closure of the VSD may occur.81 It is important to recognize that small defects, which provide a large resistance to flow, can produce loud murmurs, so murmur intensity is not a good predictor of defect size.
VSDs may be heritable in some breeds, and because of the increased risk of heart failure and other cardiac complications, breeding animals with this defect is not advised. As a general rule, bull studs do not accept animals with this defect into a breeding program.
Patent Ductus Arteriosus
DEFINITION AND ETIOLOGY. A PDA is persistent patency of the vessel (normally present in the fetus) that connects the pulmonary arterial system to the aorta. The ductus arteriosus fails to close at birth when breathing begins and placental circulation is removed. Closure of the ductus arteriosus occurs in response to decreasing pulmonary vascular resistance and increased systemic vascular resistance.
A PDA can occur as a single defect (rare in large animals) or with other cardiac anomalies. In large animals the most common other defects reported with PDA are tetralogy of Fallot and pseudotruncus arteriosus.
Clinical Signs and Differential Diagnosis
The clinical signs of PDA depend on the length and diameter of the ductus arteriosus, direction of the shunted blood, and presence of other cardiac defects. A PDA should be suspected when a continuous “machinery murmur” is auscultated. The murmur may be heard on the left and right sides of the thorax but is usually loudest in the left third or fourth intercostal space at the level of the point of the shoulder. The intensity of the murmur increases with increased heart rate, exercise, or excitement. The arterial pulses are usually bounding because of the runoff of blood from the systemic to the pulmonary circulation. Occasionally the PDA is manifested by a holosystolic murmur82 because the diastolic component is barely audible, except at the left heart base. Large PDAs can exist without producing a murmur. In the animal with increased pulmonary vascular resistance and reversal of the shunt, there may be cyanosis of the caudal parts of the body if the PDA enters the aorta caudal to the brachiocephalic trunk (rare). Stunting of growth may also occur.
Other causes of a continuous murmur in neonatal large animals are extremely rare, but detecting a continuous machinery murmur should lead the veterinary clinician to suspect a complex congenital cardiac defect that includes a PDA, rather than an isolated defect. In older horses an aorticocardiac fistula should be suspected, particularly if the machinery murmur is of recent onset and is loudest on the right side of the chest. If the horse is a Friesian, an aortopulmonary fistula should be suspected. A systolic and diastolic murmur can be present in young animals with a large VSD causing AR. A similar murmur is possible with vegetative endocarditis of one of the atrioventricular or semilunar valves, producing insufficiency and stenosis of the affected valve. These latter conditions should not have the machinery murmur characteristic of the PDA. A loud systolic ejection murmur, which is confused with a PDA, frequently can be heard at the left heart base of foals shortly after closure of the PDA. This murmur may persist for 2 to 3 months.55
Clinical Pathology
No characteristic clinicopathologic changes are associated with a PDA. Radiography may show enlargement of the cardiac silhouette and pulmonary overcirculation in an uncomplicated PDA. Pulmonary venous congestion, interstitial pulmonary edema, and alveolar edema are evidence of a large PDA with left-sided heart failure. These signs are not specific for PDA and can be present with any congenital heart defect that results in a left-to-right shunt. No consistent electrocardiographic pattern has been identified with PDA. Echocardiographic detection of an enlarged left atrium and left ventricle, with a pattern of left ventricular volume overload and increased values for the ratio of the left atrial to aortic root dimension, are consistent with a PDA.10,53,82,83 Direct visualization of the ductus arteriosus echocardiographically is difficult but is most successful from the left cardiac window looking dorsally between the aorta and main pulmonary artery. A PDA arising from the pulmonary artery has been imaged echocardiographically in an 11-month-old Friesian-Holstein heifer.56 A PDA has also been imaged by the author in a 9-year-old Quarter Horse mare. High-velocity turbulent flow in the pulmonary artery and ductus arteriosus is detected throughout the cardiac cycle with pulsed-wave, continuous-wave, or color-flow Doppler echocardiography.10
Cardiac angiocardiography and nuclear angiocardiography using a selective aortic angiogram provide definitive evidence of a PDA. Oximetric data show a step-up in oxygen content or saturation in the pulmonary artery proportional to shunt size. Indicator dilution methods also provide evidence of a left-to-right shunt occurring in the pulmonary artery in cases of an uncomplicated PDA. Pulmonary arterial and right ventricular pressures may be increased with a large PDA.
Pathophysiology
Normally the ductus arteriosus narrows near term and constricts rapidly after birth in response to lowered pulmonary vascular resistance, increased systemic vascular resistance, increased blood volume, and increased left ventricular pressure when breathing begins and the placental circulation is removed. If the ductus arteriosus is large or the resistance to flow across the ductus is minimal, there is a significant left-to-right shunt that produces a large left ventricular volume overload. The left ventricular response may be failure or, with time, dilation (primarily) and hypertrophy. Pulmonary hypertension and congestion result. The right ventricle can be affected by the pulmonary pressure load, and right ventricular hypertrophy can also develop. If the pulmonary resistance equals or exceeds the systemic vascular resistance, a right-to-left shunt occurs.
Epidemiology
Normal foals may have a PDA for a few days after birth, but functional closure of the ductus arteriosus is expected by 96 hours of age.82 Normal ruminants rarely have a PDA after birth, and if one is present it is considered abnormal. Functional closure may precede anatomic closure of the PDA. This defect is uncommon in older animals. No evidence suggests that this is an inherited defect in horses or cattle.
Necropsy Findings
The ductus arteriosus can be of variable length and diameter but is patent between the aorta and pulmonary artery. The PDA often enters the aorta caudal to the origin of the brachiocephalic trunk. Changes in the left and right ventricles and lung and pulmonary vasculature are variable and depend on the size of the shunt. When the PDA is large, there may be cardiomegaly with left atrial and left ventricular dilation, right ventricular hypertrophy, dilation of the pulmonary artery, pulmonary congestion, and edema.
Treatment and Prognosis
There is insufficient evidence on which to base a prognosis for animals with PDA. The condition can be corrected surgically in neonates, but future performance has not been documented. Animals with small defects may remain asymptomatic throughout life. However, a marked dilatation of the pulmonary artery around the shunt is a safety concern in a horse that is to be ridden or driven, as pulmonary artery rupture is possible. The prognosis is poor if the defect is large, because the risk for left (primarily) and right ventricular failure is increased. Pharmacologic closure of the PDA using inhibitors of prostaglandin synthesis has been successful in humans but is not without risk of complications and recurrence. The efficacy of prostaglandin inhibitors has not been evaluated in large animals.
Tetralogy and Pentalogy of Fallot
DEFINITION AND ETIOLOGY. Tetralogy and pentalogy of Fallot are characterized by biventricular origin (overriding) of the aorta, VSD, obstruction of pulmonary arterial flow, and secondary right ventricular hypertrophy. When there is an associated ASD or PDA, the anomaly is referred to as pentalogy of Fallot. The defect is caused by abnormal development of the conal septum in the embryonic heart, which leads to narrowing of the right ventricular infundibulum (pulmonic stenosis), an inability of the conal septum to participate in closure of the interventricular foramen (VSD), and overriding of the aorta. Right ventricular hypertrophy due to pulmonary outflow obstruction develops.
Clinical Signs and Differential Diagnosis
Tetralogy of Fallot is one of the more common congenital cardiac defects that cause cyanosis in large animals. Resting cyanosis is rare in horses, although it may be detectable after exercise. Cyanosis of the oral and nasal mucosa, tongue, vaginal mucous membranes, and occasionally the nose and skin of light-colored animals is noticed when >5 g/dL of hemoglobin are reduced (unoxygenated). Exercise intolerance is often marked and is usually characterized by dyspnea or collapse. Frequently the owner complains of slow growth or small size. A loud pansystolic murmur associated with a palpable thrill is loudest in the left third to fourth intercostal spaces. The murmur may be a crescendo-decrescendo murmur of pulmonic stenosis or the harsh, plateau-shaped murmur of a VSD; one of these usually predominates. A harsh band-shaped pansystolic murmur is also auscultated in the tricuspid valve area but is usually one or two grades softer than the pulmonic stenosis murmur. Excitement of the animal may result in auscultation of a gallop rhythm or an early systolic ejection click. A continuous machinery murmur associated with continuous shunting through the PDA can be auscultated in some patients with pentalogy of Fallot.
Tetralogy and pentalogy of Fallot must be distinguished from other causes of cyanosis in young animals. Respiratory distress syndrome of neonates can be distinguished by the presence of tachypnea, dyspnea, and abnormal lung sounds in the absence of a cardiac murmur. Cyanosis caused by central nervous system disease has other neurologic manifestations. Cyanosis from congenital cardiac disease may be caused by a right-to-left shunt or heart failure with pulmonary edema. Cyanosis resulting from heart failure or respiratory disease improves with oxygen administration, whereas the patient with a right-to-left cardiac shunt fails to improve. Right-to-left cardiac shunting does or can occur with tetralogy and pentalogy of Fallot, reverse PDA or VSD (rare), tricuspid valve or right ventricular atresia, left ventricular hypoplasia, persistent truncus arteriosus, pseudotruncus arteriosus, and other complex congenital cardiac disease, all of which may occur with cyanosis and a cardiac murmur. A complete echocardiographic examination (Video 30.2) using a segmental approach to cardiac anatomy is necessary to accurately diagnose the correct congenital cardiac malformation and has widely supplanted other methods of diagnosing complex congenital cardiac disease in large animals. Radiography and cardiac catheterization provide supplemental information that may be helpful in distinguishing among the causes of right-to-left cardiac shunting.
Clinical Pathology
Increased packed cell volume (PCV), red blood cell count, and hemoglobin concentration (polycythemia) may be present in some animals with tetralogy and pentalogy of Fallot.58 However, polycythemia is uncommon in foals with cyanotic congenital cardiac disease and the PCV is usually valve dysplasia is a rarely reported early developmental anomaly in the horse.10,66,84 Affected foals have a grade 3/6 to 5/6 holosystolic decrescendo or coarse-type murmur loudest in the mitral to aortic valve area. Echocardiographically in the foal with mitral valve dysplasia, the mitral valve leaflets appeared thickened, bright, and irregularly nodular with a cleft in the free wall leaflet and abnormal papillary muscle and chordae tendineae.66 In the other foal, the parachute configuration of the mitral valve was readily imaged echocardiographically.84 The foals died or were humanely euthanized due to their poor prognosis. Other congenital variations in the configuration of mitral valve leaflets, usually the free wall and accessory leaflets, occur more frequently in horses, usually compatible with a normal life expectancy. These horses usually a have mild MR with little or no progression over many years.
Ventricular Hypoplasia. Ventricular hypoplasia has been reported in foals and calves.54,73 The defect may be present with other cardiac defects and is usually associated with early death. The defect was present in three closely related Holstein calves, suggesting possible genetic factors.54
Truncus or Pseudotruncus Arteriosus. Persistent truncus arteriosus refers to the condition in which one arterial vessel leaves the heart above a VSD. The coronary and pulmonary arteries and aorta arise from this vessel. Persistent truncus arteriosus has been diagnosed in foals and calves.60 Subclassifications of this condition have been applied to humans, depending on the origin of the pulmonary trunk or arteries. Pseudotruncus arteriosus has also been described in foals and a calf and is characterized by the presence of a remnant of an atretic pulmonary trunk.59,85 With pseudotruncus arteriosus, the pulmonary blood supply comes from bronchial arteries or a PDA. Clinical manifestations of these conditions include tachycardia, exercise intolerance, and a cardiac murmur. The murmur may be a continuous machinery murmur if a PDA is also present; holosystolic and crescendo-decrescendo, loudest at the left heart base; or the coarse murmur of the VSD may be auscultated, although the relative pulmonic stenosis component is absent. Cyanosis, dyspnea, or syncope may be seen with exercise or excitement. CHF and stunted growth may be present. Polycythemia was detected in a calf with a pseudotruncus arteriosus.85 The presence of cyanosis with the cardiac murmur helps differentiate this condition from a simple VSD or PDA. Definitive diagnosis may be made by echocardiography, angiocardiography, or nuclear angiocardiography. These foals and calves have a guarded to grave prognosis. Their life expectancy depends on the magnitude of their pulmonary blood flow.
Aortic Anomalies. Dextropositioning or transposition of the aorta are the most common aortic anomalies of foals and calves and are seen most frequently with other defects. Other aortic anomalies of foals and calves are persistence of the right aortic arch and double aortic arch, which may cause esophageal compression. The clinical presentation is one of esophageal obstruction. Interruption of the aortic arch in two foals with VSD, ASD, and PDA has been reported.70 The foals showed weakness, lethargy, cyanosis, and tachycardia. The murmur was pansystolic and plateau shaped, with the PMI on the right side of the thorax. Radiology showed cardiomegaly and increased vascularization of the lungs. Cardiac catheterization showed left ventricular failure.
Bicuspid and quadricuspid cusps of the aortic and pulmonic valves occur in large animals and usually result in both stenosis and valvular insufficiency. An aneurysm of the sinus of Valsalva was detected in a 3-year-old Thoroughbred gelding as an incidental finding.86 Occasionally a diastolic murmur may be associated with AR in horses with sinus of Valsalva aneurysms.87 These sinus of Valsalva aneurysms usually rupture later in life, and the horse develops acute distress, colic, and uniform VT. A continuous machinery murmur associated with the presence of an aortico cardiac fistula (ACF) is usually present on the right side of the thorax (see Vascular Disease).
Eisenmenger Complex. Eisenmenger complex has been described in a stunted 24-month-old Holstein heifer that had a loud, crescendo-decrescendo, pansystolic murmur heard best over the pulmonic valve.62 The heifer had a prominent gallop rhythm from a loud fourth heart sound, exercise intolerance without cyanosis, and polycythemia. Cardiac catheterization showed increased pressures in the right atria, right ventricle, and pulmonary artery, with normal left-sided pressures. The echocardiogram was characterized by a VSD, overriding aorta, and dilation of the pulmonary trunk, a feature that distinguished this from tetralogy of Fallot. Left ventricular function was decreased, and at necropsy the heart was enlarged and rounded with a dilated pulmonary trunk and small aorta. The right ventricle was dilated and hypertrophied, whereas the left atria and ventricle were only mildly dilated.
Ectopia Cordis Cervicalis. Ectopia cordis cervicalis is a relatively common defect of cattle.54,69 Although this defect usually results in the heart being in the cervical region, a few animals may have the heart in the pectoral region (14%) or abdomen (3%).69 Various defects are associated with ectopia cordis cervicalis, including defects of the heart, great vessels, neck (torticollis), ribs, and sternebrae. The heart is usually contained within the pericardium under the muscles of the skin in the ventral cervical area, with the double apex of the heart pointing craniodorsally. The ligaments of the pericardium are most frequently attached to the mandibles and the parotid fascia cranially, the cervical fascia laterally, and the first rib or manubrium caudally. The lung may lack the cardiac notch and often protrudes to the base of the heart. Although the prognosis for a productive life is poor, some calves lived until about 1 year of age.
Miscellaneous Cardiac Defects. Other cardiac defects occur, but the defect has been recorded infrequently. Complete atrioventricular canal defect has been reported in several foals.71,72,88 Anomalous coronary artery development has been reported at postmortem examination in both calves and horses and has been thought to be the cause of death in most cases.89-91 Congenital hematomas of the atrioventricular valves also have been noted, but the significance is unknown.54 Endocardial fibroelastosis, an anomalous development of the endocardium associated with left ventricular hypertrophy, is usually a severe defect resulting in death of the animal. The frequency of this defect in large animals is not established.