Valvular Heart Disease
Definition and Etiology
In adult animals, disorders of the tricuspid, pulmonic, mitral, or aortic valves are usually acquired, resulting in insufficiency of the affected valve.
These disorders may be the result of degenerative changes, infection (bacterial or viral endocarditis or myocarditis), inflammation (valvulitis), trauma, myocardial disease (cardiomyopathy), or unknown causes. They are usually manifested by a cardiac murmur, most frequently of valvular regurgitation, with the PMI at the location of the affected valve or in the direction of the regurgitant blood flow. The mitral and aortic valves are the most common location of degenerative valve disease in horses.92 Chronic active infection such as foot abscesses, rumenitis, reticular abscess, or other septic process may lead to sustained or recurrent bacteremia, predisposing the animal to the development of bacterial endocarditis, particularly in cattle, or a nonvegetative valvulitis, probably more common in horses. Experimentally, valvular vegetative endocarditis can be induced by intravenous (IV) administration of bacteria without preliminary damage to a valve.93 Rupture of a valve leaflet or chordae tendineae can cause valvular heart disease, as can dilation of a cardiac chamber from any cause or rupture of the aortic root or of a sinus of Valsalva aneurysm. , In rare cases neoplasia, primarily lymphosarcoma of cattle, can cause valvular heart disease. Congenital valvular heart disease in adult animals is rare. The most common bacterial isolates from equine and bovine endocarditis cases are streptococci and Pasturella or Actinobacillus spp. and Trueperella pyogenes (formerly Arcanobacterium [Actinomyces] pyogenes) in horses and cattle, respectively, although a wide variety of organisms has been isolated from large animals with endocarditis.97-105Clinical Signs and Differential Diagnosis
Most animals with valvular heart disease have no clinical signs, but a cardiac murmur is usually detected during a routine examination.
Clinical signs vary depending on lesion severity and its rate of development. Murmurs of valvular heart disease are frequently holosystolic (Fig. 30.6), pansystolic, or holodia- stolic (Fig. 30.7). They radiate from the PMI in the direction of the abnormal blood flow; are coarse and band-shaped, crescendo or musical or honking (if systolic), or decrescendo and blowing or musical or sound like a “dive bomber” (if diastolic); and are usually moderate to loud in intensity (≥grade 3/6) but may be softer if holodiastolic. All these characteristics help distinguish these murmurs from functional or innocent murmurs, which generally occur early or late in systole or diastole but can be holosystolic; are soft and blowing or crescendo-decrescendo in quality; are localized to a small area; do not radiate; and are soft to moderate in intensity (≤3∕6). Murmur intensity is not a reliable indicator of lesion severity except in horses with tricuspid regurgitation (TR), in which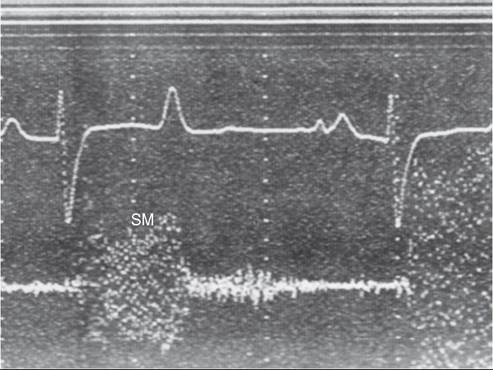
FIG. 30.6 Phonocardiogram obtained from a horse with a ruptured mitral valve chorda tendineae. A loud plateau-shaped holosystolic murmur (SM), which is variable in intensity, occurs when the free wall leaflet of the mitral valve is prolapsing into the left atrium.
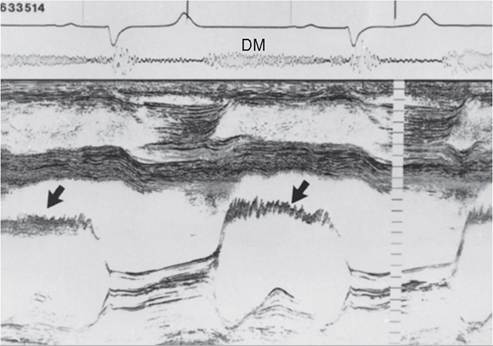
FIG. 30.7 Phonocardiogram and M-mode echocardiogram obtained from a horse with a holodiastolic murmur (DM) caused by aortic valve regurgitation. The M-mode echocardiogram shows diastolic flutter (arrows) of the septal mitral valve leaflet, characteristic of aortic valve insufficiency.
the longer, louder murmurs are associated with a larger jet of TR.106 In cattle in particular, severely involved valves (usually in cattle with endocarditis) commonly have faint or no audible murmurs.
The location of the PMI of the murmur is helpful in distinguishing which valve is involved, although more than one valve can be affected in the same animal.
The PMI for lesions of the mitral valve is often in the mitral valve area, although murmurs of MR usually radiate dorsally toward the left heart base and aortic valve area. Therefore loud systolic murmurs with the PMI in the aortic or mitral valve area in horses are usually MR murmurs. Disorders of the tricuspid valve commonly have the PMI on the right side of the thorax (third to fourth intercostal spaces [horses] or second to third intercostal spaces [cattle]). Rarely the murmur may also be heard on the left side of the thorax cranial to the pulmonic valve location in the second intercostal space. Aortic and pulmonic valve lesions produce murmurs with the PMI at the left heart base in the fourth or third intercostal space, respectively. Acquired valvular lesions of the mitral and tricuspid valves produce primarily systolic murmurs.26,97,98,100,106-111 Diastolic tricuspid flow murmurs have been reported, however, and may be associated with right-sided mural or valvular masses in horses80 or may be physiologic, associated with normal blood flow across the atrioventricular valves.112,113 Lesions of the aortic and pulmonic valves may produce diastolic murmurs, systolic murmurs (rare), or both, 6 but diastolic murmurs of regurgitation are most common in large animals. AR associated with degenerative valve disease is most common in horses, whereas pulmonic regurgitation (PR) associated with bacterial endocarditis is more common in cattle. Aortic valve lesions in horses have primarily holodiastolic, decrescendo, musical murmurs (see Fig. 30.7) but can also be decrescendo, soft, and blowing. AR murmurs are accompanied by a water-hammer or bounding arterial pulse if the AR is associated with a significant left ventricular volume overload.26,97,117,118 The musical quality of the murmur (harmonic) indicates that some part of the aortic valve is vibrating during diastole. The arterial pulse quality becomes more bounding as the AR becomes more severe and is a good clinical indicator of the degree of left ventricular volume overload. Ventricular premature beats and AF may also be detected in horses with significant AR.118Besides the cardiac murmur, animals with valvular heart disease may have exercise intolerance, arrhythmias, weight loss, or signs of CHF evidenced by tachycardia, coughing, respiratory distress, jugular venous distention, subcutaneous edema, and ascites (uncommon in large animals, especially horses). In adult cattle, mammary vein distention is another sign of CHF.98 Cardiac enlargement may be noted as an increased area of auscultation and/or percussion or caudal dislocation of the apical impulse of the heart. AF may be present. This development is usually an indicator of atrial enlargement in animals with valvular heart disease. If TR is present, there may be abnormal systolic jugular venous pulsations. If MR is present there may be tachycardia, tachypnea, poor recovery to resting respiratory rate after exercise, coughing, and frothy pulmonary edema (uncommon). Lung sounds may be harsh at rest and on deep inspiration may include crackles or moist bubbly sounds (both of the later auscultatory findings are rare). Most horses with pulmonary edema have only harsh breath sounds that are detected at rest and on deep inspiration.
One of the clinical signs of bacterial endocarditis is a cardiac murmur, the PMI and timing of which depend on the valve or valves affected. Other signs may include tachycardia, arrhythmias, auscultation of prominent heart sounds, tachypnea, coughing, recurring fever, anorexia, weight loss, or signs of CHF. Evidence of disseminated sepsis such as pneumonia, hematuria, or pyuria is usually present in cattle but not in horses. Shifting leg lameness and swollen joints or tendon sheaths are common but usually have an immune-mediated cause, although a horse with bacterial endocarditis and septic tenosynovitis has been reported.101 Mastitis and decreased milk production are common in cattle. The presence of weight loss, fever, and signs of recurring sepsis help distinguish bacterial endocarditis from other forms of acquired valvular disease.
The clinical signs of a major mitral valve ruptured chordae tendineae (RCT) or its characteristic murmur distinguish this disease from other mitral valve diseases. The murmur is usually a widely radiating musical murmur of MR (see Fig. 30.6) with a distinctive honking quality (the honking quality is consistent with vibration of the mitral valve chorda tendineae or leaflet with blood flow in systole).118 However, the honking quality may be absent and replaced by a band-shaped pansystolic murmur. There may be evidence of acute hemodynamic collapse. Acute onset of respiratory distress with coughing and expectorating foamy pulmonary edema fluid (this fluid is also detected at the external nares) is a relatively consistent feature with a major RCT. Signs of right-sided heart failure (jugular venous distention, subcutaneous edema, and ascites) may develop rapidly. Atrial arrhythmias, most frequently AF, often develop secondary to atrial enlargement. Supraventricular arrhythmias have also been reported in foals with a mitral RCT.109 Acute onset of respiratory distress, along with a honking systolic murmur, distinguishes mitral RCT from other causes of MR. The honking systolic murmur of a mitral RCT can also be heard in the absence of any clinical signs in horses with a minor chordal rupture. The murmur of mitral valve prolapse (MVP) is also a distinctive murmur and should be suspected in horses whenever a crescendo midsystolic to late-systolic or holosystolic murmur is auscultated with the PMI over the mitral valve area.26,118,119 A similar murmur is frequently auscultated in horses with tricuspid valve prolapse (TVP). Murmurs of MVP or TVP can be detected in horses with all degrees of valvular insufficiency. Most frequently, however, only small amounts of valvular regurgitation are associated with valvular prolapse. An increased prevalence of MR and TR has been reported in young horses in training.120-123
Clinical Pathology
Diagnosis of valvular disease is best performed with a complete echocardiographic examination including M-mode, 2D, and Doppler echocardiography.
Two-dimensional echocardiography is superior to M-mode for detection of valvular abnormalities (Figs. 30.8 and 30.9), measurement of valvular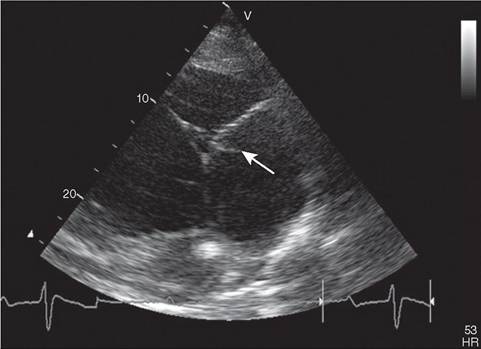
FIG. 30.8 Two-dimensional echocardiographic image obtained from the left parasternal window of a ruptured mitral chorda tendineae (arrow) in the left atrium of a gelding with mitral regurgitation and a honking pansystolic
murmur.
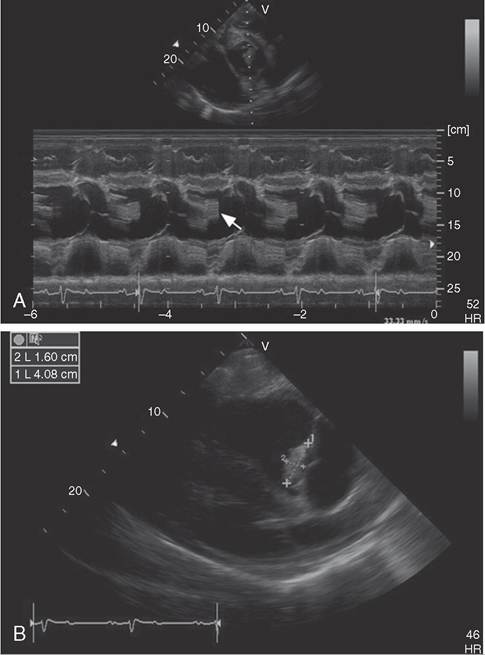
FIG. 30.9 Echocardiograms of a bacterial endocarditis lesion on the aortic valve of a horse. The lesion can be seen on the aortic valve M-mode (A) as a thick echoic band (arrow) and is measured in the two-dimensional echocardiographic image of the left parasternal long-axis view (B).
masses (see Fig. 30.9, B) (Video 30.3), and global assessment of ventricular function, but chamber enlargement, high-frequency vibrations of the valve leaflets (Video 30.4), and shortening fraction (an indication of ventricular systolic function) can be determined by both. Pulsed-wave, continuous-wave, and color-flow Doppler echocardiography can be used to semiquantitate the severity of valvular regurgitation and should
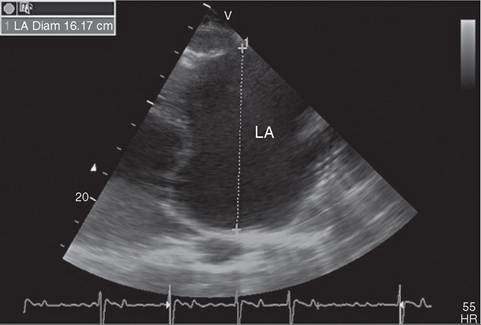
FIG. 30.10 Left parasternal echocardiographic image of the left atrium (LA) and mitral valve from a horse with left atrial enlargement (16.17 cm).
be performed from both sides of the thorax, interrogating the left atrium in multiple imaging planes.10,119,124,125 The size of the regurgitant jet at its origin and the extent of the jet within the left atrium detected with pulsed-wave and/or color-flow echocardiography are two indicators of the severity of the valvular insufficiency.26 Detection of proximal flow convergence indicates hemodynamically significant MR. The duration of the MR jet is also important in assessing severity. Clinically insignificant jets of regurgitation are detected only just behind the valve when it is closed. Valvular insufficiency is mild when the jet occupies one third or less of the receiving chamber, moderate when the jet occupies greater than one third but less than two thirds of the receiving chamber, and severe when the jet occupies greater than two thirds of the receiving chamber. The intensity and shape of the spectral Doppler tracing of the MR jet also provide information about its severity. Severe MR is associated with an intense triangular rather than parabolic signal that increases rapidly at the onset of systole.
Echocardiographic signs of MR are increased left atrial (Fig. 30.10; also see Fig. 30.3) and left ventricular dimensions, rounding of the left ventricular apex, and a pattern of left-sided volume overload. Left ventricular function may be normal (if MR is mild) or the FS may be increased (if there is a significant left ventricular volume overload associated with acute moderate to severe MR), unless there is concomitant myocardial disease. Normal or decreased contractility is present with chronic, severe MR. A round, turgid left atrium with bulging of the interatrial septum toward the right is another indication of hemodynamically severe MR. A larger-than-normal pulmonary artery (larger than the aortic root) is compatible with severe pulmonary hypertension and left-sided heart failure. A smaller-than-normal aortic root is detected echocardiographically in horses in low-output left-sided heart failure (Video 30.5).10,26,109,110,119
The cause of the valvular regurgitation can often be determined. Endocarditis, mitral RCT (see Fig. 30.8), a flail valve leaflet, valvular prolapse, or thickening of the valve leaflet are readily imaged echocardiographically.110 The regurgitant jet detected with pulsed-wave or color-flow Doppler echocardiography usually originates from the site of the valvular abnormalities detected with 2D echocardiography. In some animals, the lesion responsible for the valvular insufficiency is not visualized with 2D echocardiography, but the regurgitant orifice is detected with pulsed-wave or color-flow Doppler echocardiography.6,10,125 A mitral RCT is diagnosed by finding a mobile linear echo everting into the left atrium (see Fig. 30.8) or a flail leaflet that may prolapse into the left atrium during systole, systolic and chaotic diastolic mitral valve flutter, rapid mitral valve opening with increased excursion of the affected leaflet, and lack of coaptation of the mitral valve in systole. The asynchronous movement of any portion of the valve leaflet during any phase of the cardiac cycle indicates the presence of a flail valve leaflet.10,26,107,110
TR may produce echocardiographic evidence of right atrial and right ventricular enlargement with paradoxical septal motion. Frequently the cause of tricuspid valve regurgitation in cattle is bacterial endocarditis, and the incompetent valve can be visualized. In cattle, neoplasia of the right atrium, tricuspid valve, or right ventricle can usually be visualized when present.126 TR is common in horses with no obvious valvular lesion.113,121,127 However, tricuspid valve bacterial endocarditis is detected in some horses with septic jugular vein thrombophlebitis.128
AR is diagnosed echocardiographically by observing left ventricular dilation, increased aortic root diameter (Fig. 30.11), increased left ventricular FS (if the AR is moderate to severe and left ventricular function is normal), diastolic fluttering of the septal mitral valve leaflet (see Fig. 30.7), or less frequently by observing high-frequency vibrations of the interventricular septum (Fig. 30.12) or aortic valve in diastole.10,26,115,117,129 Rarely, premature closure of the mitral valve is detected. Thickening of the left cusp of the aortic valve is frequently detected echocardiographically, but prolapse, fenestration, healed
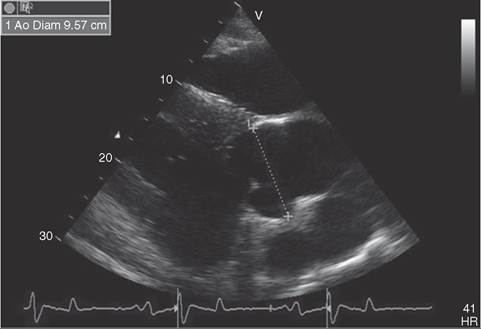
FIG. 30.11 Two-dimensional echocardiographic image of an enlarged aortic root (9.57 cm) obtained from an aged gelding with moderate aortic regurgitation that has been present for several years.
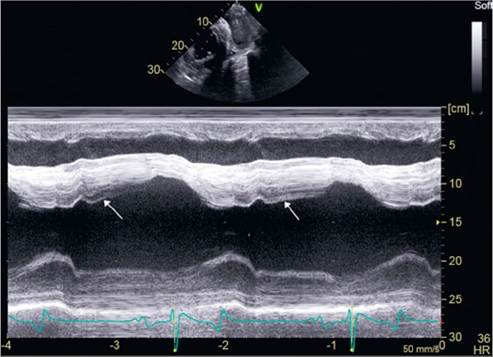
FIG. 30.12 M-mode echocardiogram obtained from a gelding with moderate chronic aortic regurgitation. Notice the high-frequency vibrations (arrows) on the interventricular septum.
endocarditis lesions, and tears of the aortic cusps also occur. A decrease in the aortic root diameter during diastole is an echocardiographic indicator of increased severity of the AR.
Acquired pulmonic valve lesions are uncommon in large animals and when present are usually associated with bacterial endocarditis.116,130 Diagnosis is established by finding the mass associated with the pulmonic valve. Severe PR associated with pulmonic valve rupture has been reported in one horse.131 PR is most common in horses with pulmonary hypertension and CHF but is rarely detected clinically.
Lesions of bacterial endocarditis (see Fig. 30.9 and see Video 30.3) may have a shaggy, ragged, or cystic appearance on 2D echocardiography. These lesions are even better visualized with 4D echocardiography. Occasionally the only abnormality noticed is valve thickening, with ventricular hyperkinesis and enlargement of the chambers on the side of the affected valve. Acoustic reverberation and production of microbubbles have also been associated with valvular bacterial endocarditis.109,112 Other laboratory evidence of bacterial endocarditis includes anemia, neutrophilia (a left shift may be present), an increased serum globulin concentration, increased serum amyloid A (SAA), and hyperfibrinogenemia. Liver enzymes are frequently mildly elevated, and a urinalysis sometimes shows hematuria or pyuria. Positive blood cultures taken during febrile episodes confirm the diagnosis when associated with these findings, but many times culture results are negative in large animals with bacterial endocarditis. Other laboratory evidence of disseminated sepsis includes neutrophilic response in peritoneal, tracheal wash, or joint fluid. Ventricular arrhythmias (VA) are frequently detected electrocardiographically in individuals with mitral or, more commonly, aortic valve endocarditis. Radiographic or sonographic evidence of disseminated pneumonia may also be found with bacterial endocarditis, usually in large animals with a right-sided lesion.
Other laboratory evidence of valvular heart disease is nonspecific. The ECG is valuable for documenting cardiac arrhythmias occurring secondary to chamber enlargement or the underlying myocardial disease. Radiographic findings of cardiac enlargement, increased pulmonary vascular pattern, or pulmonary edema are also nonspecific. Cardiac catheterization and pressure measurements help determine the degree of cardiac dysfunction. Nuclear angiocardiography shows cardiac enlargement or prolonged washout of contrast material. Time-activity curves can be helpful in accurately documenting ventricular dysfunction and the valvular regurgitant fraction.50
Pathophysiology
Acquired valvular heart disease that is slow in onset or gradually progressive may be asymptomatic at first, but cardiac changes occur that eventually may lead to CHF in some large animals. Valvular incompetence from endocarditis, degenerative changes, RCT, or other causes results in volume overload of the recipient chamber. Initially the output of the chamber is increased to maintain forward output, but the increased volume of the recipient chamber leads to compensatory dilation and a mild elevation in pressure. Compensatory hypertrophy may also result. In the later stages of valvular regurgitation, contractile function of the volume-overloaded chamber may diminish, leading to further elevation of pressure and decreased compliance. In the case of severe AR and MR, this causes elevation of left atrial pressure and eventually pulmonary venous hypertension. PAWP is higher at rest and during exercise in horses with moderate MR.132 With severe TR, right atrial pressure or CVP increases. Increased myocardial oxygen consumption is a natural sequela, and biventricular failure can ensue.
If valvular heart disease is acute in onset, as with major RCT of the mitral valve, the regurgitation and volume overload are imposed on the left atrium, which cannot dilate and adapt acutely to the increased diastolic filling. The sudden hemodynamic change leads to pulmonary venous hypertension and acute pulmonary edema. However, most horses with MR do not have acute fulminant pulmonary edema. Instead, chronic pulmonary hypertension leading to subtle respiratory signs associated with interstitial pulmonary edema and the subsequent development of right-sided CHF are common in horses with severe MR.110 In one study, 12 of 14 horses with CHF had jugular distentions or pulsations, 10 had abnormal lung sounds (crackles), and 9 had a cough.133
Bacterial endocarditis of the mitral or tricuspid valve may lead to RCT. Mitral RCT has been reported in adult horses and foals with bacterial endocarditis, leading to acute left-sided CHF.109 In addition to the hemodynamic load placed on the heart from an incompetent valve, bacterial endocarditis also results in disseminated sepsis. The vegetations are made up of layers of fibrin, blood cells, necrotic tissue, and bacteria and are relatively resistant to short-term antimicrobial therapy. Disseminated sepsis may be the cause of death or the reason for culling of the animal. Myocardial necrosis of a papillary muscle was associated with mitral chordal rupture in one foal.109
Epidemiology
Acquired valvular heart disease is common in large animals, involving 356 of 1557 horses (22.9%) in one abattoir survey.92 Endocarditis, one form of valvular heart disease, was reported in 4% of cattle in another study.134 Bacterial endocarditis most commonly affects the tricuspid valve in cattle but has been reported on the pulmonic, mitral, and aortic valves as well.98,111,115,116 Most cases of tricuspid valve bacterial endocarditis have been reported in horses with septic jugular vein thrombophlebitis.97,100,135 Tricuspid valve endocarditis has also been reported in a horse with a VSD.80 Aortic and mitral valve endocarditis are most common in horses, occurring with nearly equal frequency.99,100 In the largest survey of acquired valvular heart disease in horses, the aortic valve was affected most commonly with degenerative valve changes, followed by the mitral valve, tricuspid valve, and (uncommonly) pulmonic valve.92 Not all valvular lesions are associated with incompetency of the valve. Degenerative valvular changes, particularly changes involving the aortic valve, are seen more commonly in older horses.
Necropsy Findings
Acquired valvular disease is associated with finding nodular thickening, fibrous bands, valve fenestrations, rupture of mitral valve chordae tendineae, fibrinous masses typical of endocarditis, or combinations of these lesions on postmortem examination. There may be associated or secondary changes varying from enlargement of a chamber or vessel to degeneration, inflammation, and fibrosis. Enlargement (primarily dilation) of the chamber receiving the regurgitant flow, in addition to enlargement (primarily dilation) of the chamber or vessel from which the regurgitant flow arises, is commonly detected. Jet lesions, usually found in the receiving chamber, are associated with the high-velocity turbulent regurgitant blood flow.
Subcutaneous edema, congestion and mottling of the liver, and increased pericardial, pleural, or peritoneal fluid may be present and indicate CHF. Ascites associated with CHF is uncommon in large animals, particularly in horses. A primary source of chronic or active infection, along with evidence of bacterial embolization, may be seen in cattle with endocarditis but is rare in horses.
Treatment and Prognosis
Treatment and prognosis of acquired valvular heart disease depend on the cause, onset, duration, and severity of the lesion. In general, the prognosis is guarded to poor when evidence of valvular incompetence includes tachycardia, exercise intolerance, signs of CHF, or echocardiographic evidence of severe chamber enlargement. Degenerative valve disease may be asymptomatic except for a cardiac murmur, or it may be mild, but it generally is slowly progressive and therefore historically has been given a guarded prognosis. A more accurate prognosis for horses with murmurs can now be obtained from a complete echocardiographic examination, including Doppler echocardiography.10,26,118 The valve affected, the lesions detected on the valve leaflets, the degree of chamber enlargement and volume overload detected, the echocardiographic assessment of myocardial function, and the severity of the regurgitation determined with Doppler echocardiography, coupled with the animal's age and intended use, can be used to formulate a prognosis.10,26,118 Valvular regurgitation associated with no detectable abnormalities, valvular prolapse, and mild valvular thickening usually has a fair to good prognosis if the amount of valvular regurgitation is small.10,26,118,136,137 Individuals with RCT, flail valve leaflets, and marked valvular thickening usually have moderate to severe regurgitation, which is likely to progress more rapidly and usually warrants a guarded to poor prognosis.10,26,110,118,138 MR is the most likely valvular insufficiency to be associated with clinical signs of cardiovascular disease, whereas primary AR and TR infrequently result in the development of CHF or death of the animal, except in horses with severe AR. Bacterial endocarditis has a guarded to grave prognosis, even with longterm antibiotic therapy, and frequently results in sudden death of the animal, although bacteriologic cures are possible. When a bacteriologic cure occurs, severe scarring of the affected valve ensues. The severity of the valve damage depends on the size of the original endocarditis lesion. This scarring can lead to rapid progression of the regurgitation and, ultimately, result in the animal's demise.
Despite the guarded long-term prognosis, palliative therapy can be applied for most forms of acquired valvular heart disease. Bacterial endocarditis is treated with long-term administration (ideally intravenously) of bactericidal antimicrobials, the choice of which is based on blood culture and sensitivity results. Continuous IV infusion of antimicrobials is the ideal initial treatment when feasible. In cattle, initial therapy is directed at the likelihood of a gram-positive infection. Combination antibiotic therapy consisting of penicillin and an aminoglycoside is recommended for broad-spectrum coverage in a horse until the results of culture and sensitivity testing are available. Using rifampin at an oral (PO) dose of 5 mg/ kg twice daily in combination with another antibiotic with appropriate spectrum has improved the short-term outlook for large animals with bacterial endocarditis. Clopidogrel (2 mg/ kg/day PO) has largely replaced aspirin and subcutaneous SC low-dose heparin in the horse in patients with valvular endocarditis in an attempt to prevent platelet adhesion and increased size of the valvular mass. In ruminants however, aspirin (100 mg/kg/day PO) and subcutaneous (SC) low-dose sodium heparin (30 to 40 units/kg twice daily) continue to be used. Early diagnosis and aggressive treatment with the appropriate antimicrobials for a prolonged period are important for successful treatment of bacterial endocarditis. The long-term outcome for successfully treated cases is still poor because the scarring that results as the endocarditis lesion heals may lead to severe valvular regurgitation and death of the animal, particularly with left-sided bacterial endocarditis lesions.26,100 102,139 Compliance and economics are also major drawbacks in treating endocarditis.
The hemodynamic consequences of valvular heart disease (volume overload or CHF) may be improved by using diuretics. Furosemide has been used most commonly at a dose of 1 mg/ kg as needed. With the low bioavailability of PO furosemide, IV administration is preferred to obtain the maximal diuretic effect.140 Digoxin can be used to improve contractility when CHF has occurred. Conditions such as AR or MR may
■ BOX 30.1
show little or no long-term improvement, although many individuals improve for 2 to 6 months or more, before the CHF becomes refractory to treatment. Administration of a maintenance dose of digoxin at 2.2 μg7lcardiac output, increased right ventricular end-diastolic pressure, increased right atrial pressure or CVP, jugular venous distention, or subcutaneous edema) associated with chronic pulmonary disease is rare but may be more common than previously recognized. However, right-sided heart dysfunction associated with pulmonary hypertension and left-sided heart dysfunction is a common cause of CHF.
Clinical Signs and Differential Diagnosis
Frequently the primary presenting clinical sign of brisket disease is subcutaneous edema of the brisket, ventral thorax, submandibular area, and occasionally the limbs. Lethargy, weakness, bulging eyes, diarrhea, collapse, and death occur.151 Jugular venous distention or pulsations may be present. Dyspnea and tachypnea are frequent. Tachycardia is present, and a gallop rhythm may be auscultated. Splitting of the second heart sound (S2) is a variable finding. Pulmonary hypertension may accentuate the separation of the aortic and pulmonic valve closures, producing audible splitting of S2 that is most noticeable during inspiration. In some horses with moderate or severe equine asthma (also known as recurrent airway obstruction [RAO]) and increased vascular impedance, pulmonic valve closure occurs early and only a single S2 is audible.156
A cardiac murmur may be auscultated, caused either by TR or a pulmonic valve ejection murmur. The murmur of TR, which is secondary to right ventricular dilation, is regurgitant or plateau shaped, with the PMI over the right thorax or, less frequently, the left second intercostal space. The pulmonic valve ejection murmur, found less commonly, is audible as a crescendo-decrescendo murmur at the left heart base.6 Pleural or pericardial effusion is not common with cor pulmonale.157 In horses with RAO leading to cor pulmonale, tachypnea, labored breathing, coughing, and exercise intolerance are common complaints. Wheezes are usually auscultated bilaterally in the thorax of affected horses.
These clinical signs are not specific for brisket disease (cor pulmonale) and largely reflect right-sided heart failure. Other considerations when signs of right-sided heart failure are present should be bacterial endocarditis or TR from any cause, cardiomyopathy, cardiac lymphosarcoma or other thoracic neoplasms, traumatic reticulopericarditis or other causes of pericarditis, left-sided heart failure, pleuritis or pleural effusion, and congenital pulmonic valve stenosis (rare). With pericarditis, heart sounds may be muffled, or the characteristic “washing machine murmur7rub” may be audible. Left-sided heart failure is frequently accompanied by pleural effusion, pulmonary edema, and weak peripheral pulses. In horses, however, expectoration of pulmonary edema fluid occurs only with sudden onset of
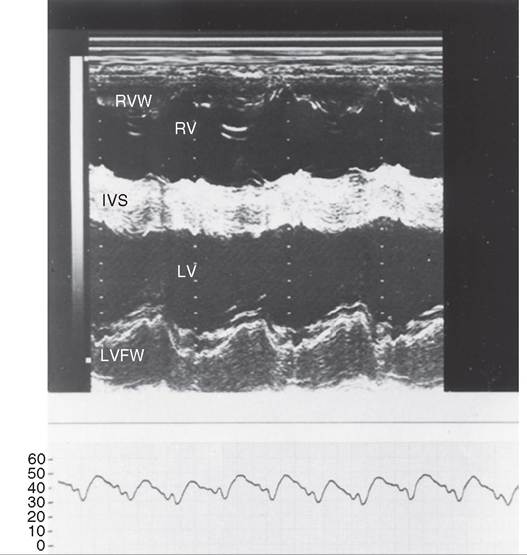
FIG. 30.13 M-mode echocardiogram and pulmonary artery pressure (PAP) curve obtained from a cow with pulmonary hypertension and cor pulmonale. The echocardiogram shows mild thickening of the right ventricular wall (RVW) and interventricular septum (IVS), dilation of the right ventricle (RV), and abnormal septal motion. LV Left ventricle; LVFW, left ventricular free wall. The PAP curve demonstrates elevated systolic and diastolic pressures. (PAP curve in millimeters of mercury [mm Hg].)
severe left-sided heart failure. In horses with chronic left-sided heart failure, tachypnea, coughing, poor recovery after exercise, and harsh lung sounds may be all that is detected.
Clinical Pathology
A complete blood cell count (CBC) may reveal a neutrophilia in cases of cor pulmonale caused by primary lung disease. Radiography of the thorax reveals primary pulmonary disease such as bronchopneumonia, bronchiectasis, or chronic bronchitis in cattle that have developed this disease at low altitudes. Radiographic findings in horses with RAO usually reveal an interstitial pattern. Arterial blood gases demonstrate the presence of hypoxia and may also show hypercapnia. Transtracheal wash fluid cytology and bacterial culture may provide evidence of the cause of the primary lung disease. Fecal sedimentation helps rule out parasitic bronchitis or pneumonia. Electrocardiographic findings are not specific. An echocardiogram may provide further evidence of pulmonary hypertension and right-sided heart dysfunction by showing right ventricular hypertrophy and dilation, increased septal thickness, and abnormal septal motion (Fig. 30.13).158,159 Dilation of the pulmonary artery is also detected with 2D echocardiography and is a sensitive indicator of pulmonary hypertension or increased flow through the pulmonary artery. A dilated pulmonary artery has been reported in horses with cor pulmonale and in horses with acute pUlmonary obstruction from RAO.159,160 Cardiac catheterization reveals elevated pressure in the pulmonary artery, right ventricle, and right atrium. Elevation of right ventricular end-diastolic pressure is a sign of right ventricular failure.
Pathophysiology
Pulmonary arteriolar constriction is the response to hypoxia from high-altitude dwelling or pulmonary disease. The response to hypoxia varies depending on the amount of smooth muscle in the pulmonary arteries. In cattle, increased pulmonary vascular resistance and pulmonary hypertension frequently develop. Chronic pulmonary artery hypertension causes a pressure overload on the right ventricle, which responds to the increased workload with hypertrophy, dilation, or failure, depending on the speed with which the condition develops. The disease is progressive, and at some stage the right ventricular myocardium is unable to compensate, dilates, and fails. With failure come the typical signs of jugular venous distention and development of subcutaneous edema. Chronic right-sided heart failure may result in diastolic dysfunction of the left ventricle.
Epidemiology
The disease is more common in cattle than in other animal species, especially when cattle are kept at altitudes over 6000 feet, where the incidence has been estimated at 0.5% to 5% in cattle native to high altitude.151,152 In cattle adapted to low altitude and moved to higher altitude for grazing, however, the incidence is much higher.151,152,161 Mainly calves and yearlings are affected. A genetic predisposition to develop pulmonary arterial constriction when subjected to hypoxia at high altitude is present in many breeds. Some breeds and pedigrees within breeds are more resistant than others to the effects of high altitude, and the inheritance appears to be complex.151,152 More cases of HMD are detected in the fall and winter and are due to cold weather exacerbating pulmonary hypertension.152 Ingestion of swainsonine contained in locoweed (Oxytropis and Astragalus spp.) also predisposes cattle to right-sided heart failure at high altitudes by causing toxic myocardial damage.153 Pulmonary hypertension has also been detected in cattle fed ionophores at high altitude.151
Necropsy Findings
There is evidence of right-sided heart failure (e.g., subcutaneous edema) in the submandibular area, brisket, and ventral abdomen. Findings include dilation and hypertrophy of the right ventricle, congestion of the liver, and ascites. Perirenal edema, mesenteric edema, and pleural effusion are often present. The lung may have evidence of concurrent pneumonia, bronchitis, bronchiectasis, or emphysema. Lesions of locoweed toxicity may be found in other organs in cattle.153 Lesions of chronic interstitial pulmonary disease are found in horses with equine asthma.
Treatment and Prognosis
Removing the animal from high altitude, treating the primary lung disease, and administering oxygen may help eliminate the hypoxia and thus the pulmonary hypertension. Cor pulmonale from high altitude is potentially reversible when the animal is returned to a lower altitude. However, cattle with other lung disease and a mean PAP of 50 to 55 mm Hg rarely have their mean PAP return to an acceptable level for high- altitude living.151 The heart failure can be treated with digoxin and diuretics. Beneficial effects of vasodilator therapy have not been documented. Once heart failure signs have developed, the prognosis is guarded even with appropriate treatment. Removing the horse from the environment inducing equine asthma is critical to treating the cor pulmonale. A more detailed discussion of the treatment and management of horses with equine asthma can be found in Chapter 31.
Prevention and Control
Selection of breeding stock with low or normal PAPs at altitudes above 5000 feet (mean PAP g/dL) and cellularity (white blood cell [WBC] count < 2500∕μL), with the predominant cell type being mononuclear cells unless the myocarditis is an extension of pericarditis. Serum should be tested for serologic evidence of bovine leukosis (BLV) infection in adult cattle, α-tocopherol, glutathione peroxidase, and copper concentrations. Whole blood
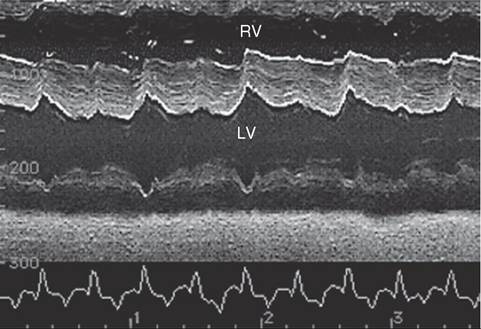
FIG. 30.15 M-mode echocardiogram of the left ventricle (LV) obtained from a mare with sustained uniform ventricular tachycardia. Note the small end-diastolic and end-systolic dimensions of the left ventricle and the little variation between systole and diastole in this dimension. RV Right ventricle.
selenium levels should be determined. In infectious myocarditis or inherited cardiomyopathy, results of these tests will most likely be normal. A negative BLV test result essentially eliminates lymphosarcoma as a cause of the myocardial disease; a positive test result does not confirm a causal relationship. In horses, serum should be tested for serologic evidence of a variety of equine viruses, particularly influenza, equine viral arteritis, and herpesvirus. Hemoglobinuria, if present, suggests consideration of monensin, gossypol, or nutritional myodegeneration as the cause of myocardial disease. Arterial blood oxygen tension may be reduced below 80 mm Hg in animals with myocardial disease.
An ECG may demonstrate sinus tachycardia or other cardiac arrhythmias; the frequency and severity of these arrhythmias are best demonstrated with continuous ECG monitoring. There may be some evidence of conduction abnormalities in the base-apex lead, but these findings are not specific for myocardial disease. Echocardiography may be normal in animals with myocarditis, or the abnormalities detected may be caused by the arrhythmias present. A small left ventricular internal diameter, thickened left ventricular free wall and interventricular septum, small aortic root diameter, and decreased FS may be detected in animals with sustained VT and decreased cardiac output (Fig. 30.15). A small left ventricular internal diameter, thickened left ventricular free wall, interventricular septum, and right ventricular free wall with an increased relative and mean wall thickness and left ventricular mass is present echocardiographically in horses with hypertensive cardiomy- opathy.166 More frequently, however, there is increased ventricular chamber size, decreased thickness of the interventricular septum and left ventricular free wall, and decreased myocardial function (decreased FS, decreased EF, and myocardial dyski- nesis), especially in more severe cases of myocarditis and in animals with dilated cardiomyopathy (Fig. 30.16 and Video 30.6). In humans with myocarditis there may be evidence of abnormal left ventricular wall motion, paradoxical motion of the interventricular septum, or an echo-free pericardial space.174 Additional echocardiographic features of dilated cardiomyopathy are increased end-systolic and end-diastolic dimensions of the left and right ventricles (see Fig. 30.16), increased left atrial size, and an increased left atrial-to-aortic root dimension ratio. There may be abnormal mitral valve closure (increased EF slope) and increased separation of the septal mitral valve leaflet and interventricular septum. A decreased aortic root diameter may be detected along with a shortened ET in animals with low-output, left-sided heart failure. An enlarged pulmonary artery indicative of pulmonary hypertension (Fig. 30.17) may also be present.
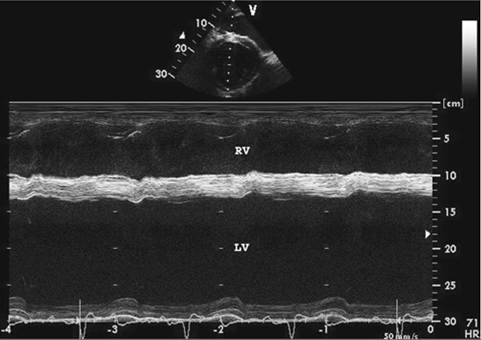
FIG. 30.16 M-mode echocardiogram of the left ventricle obtained from a mare with cardiomyopathy and severe left ventricular dysfunction. Note the large end-diastolic dimension of her left ventricle (LV), the thin interventricular septum and left ventricular free wall, and the poor left ventricular contractility. The fractional shortening in this mare varied from 2% to 8%. RV Right ventricle.
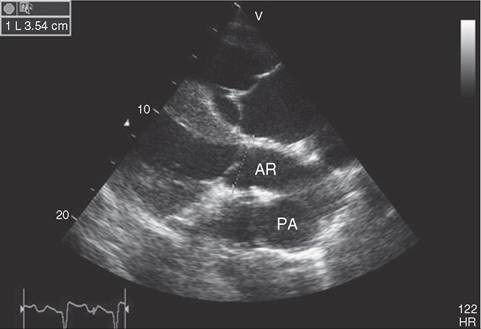
FIG. 30.17 TWo-dimensional echocardiogram of the aorta (AR) and main pulmonary artery (PA) obtained from a foal with cardiomyopathy and severe mitral and TR. The pulmonary artery is larger than the aorta, indicative of pulmonary hypertension and impending left-sided CHF. The aorta measured 3.54 cm at its origin.
Cardiac catheterization may reveal elevated intracardiac pressures (right atrial, right ventricular, pulmonary artery, pulmonary capillary wedge, and left ventricular end-diastolic) in animals with dilated cardiomyopathy. Horses with acute infectious myocarditis may show hypotension and a narrow pulse pressure. Nuclear angiocardiography may be used to show decreased EF50 in animals with myocardial disease.
Pathophysiology
The pathophysiologic changes associated with myocardial disease depend on the specific nature and extent of the disease. Acute myocarditis or angiopathic myocardial lesions162 may go on to develop into idiopathic dilated cardiomyopathy. It is speculated that changes in cellular metabolism occur with either acute myocarditis or dilated cardiomyopathy, resulting in ECG abnormalities and reduced myocardial performance (reduced cardiac output). In an attempt to compensate for reduced cardiac output, circulating fluid volume is increased by activation of the renin-angiotensin-aldosterone system and arterial resistance is increased. These compensatory mechanisms frequently lead to only minor improvement in the cardiac output of the failing heart, and the increase in ventricular preload (venous return) and afterload (arterial resistance) may cause pulmonary edema and a further reduction in cardiac contractility. Ventricular dilation, further reduction in cardiac output, and signs of heart failure occur.
Epidemiology
The prevalence of acute myocarditis is difficult to estimate because frequently the disease goes undiagnosed, is mild or masked by disease in another organ system, or the animal recovers spontaneously. Similarly, it is difficult to assess the clinical significance of postmortem findings of myocardial inflammation and fibrosis. The morbidity of myocarditis in large animals is probably underestimated because it is rarely the cause of mortality and is associated with viral, bacterial, and parasitic infections that manifest without specific signs of cardiovascular disease.
Inherited cardiomyopathy has been reported in cattle in Japan, Australia, the Netherlands, Canada, and Switzerland, with the incidence in inbred populations reaching 3% to 5%.170,171 A familial form of dilated cardiomyopathy has also been reported in cattle in Sweden, Denmark, Australia, and the United Kingdom.170 These cattle may be genetically linked by the presence of the red gene in Holstein-Friesian cattle.169 Although in some cattle, inherited cardiomyopathy resulted in death by 6 months of age,171,173 other cattle failed to show clinical signs until 2 to 6 years of age.126,168,170,172 No sex predilection is recognized in inherited cardiomyopathy of cattle.
The morbidity and mortality from cardiomyopathy stemming from other causes in cattle and horses is not known. From the number of clinical reports, inherited cardiomyopathy seems to be more prevalent in cattle than in horses. Idiopathic dilated cardiomyopathy or cardiomyopathy secondary to viral or bacterial infections may be more common in horses and is a cause for the acute onset of CHF in horses of racing age.
Necropsy Findings
There may be no gross lesions associated with myocarditis. Depending on the relationship between death and the occurrence of myocarditis, microscopic examination of the myocardium may show increased fibrous tissue in the interstitium in the absence of inflammation, or there may be foci of inflammatory cells (typically mononuclear cells), variation in the cross-sectional area of the cardiac myocytes, degeneration of adjacent myocardial fibers, myocardial necrosis, and fibrosis. Replacement of the myocardium by fibroadipose tissue has been reported in horses that experienced unexpected sudden death and were thought to have arrhythmogenic right ventricular cardiomyopathy at postmortem examination.18'-189 Focal interstitial nephritis and fibrosis were reported in eight of nine Holstein-Friesian cattle with dilated cardiomyopathy in Scotland.170 Often the inciting cause of myocardial necrosis in horses is unknown.195 Samples of gastric or ruminal contents should be obtained and submitted for analysis of ionophores if ionophore toxicosis is suspected. Feed samples should also be obtained and submitted for ionophore analysis in these cases. Submitting the heart muscle itself for ionophore analysis is the best tissue for identifying toxicosis and is superior to 198
gastric contents.198
On gross examination, the lesions of cardiomyopathy are recognized more easily as enlargement of the heart, which may be rounded to globose. Biatrial, biventricular, and pulmonary artery dilation are usually present. Patchy or uniform streaks of myocardial pallor may be detected. In rare cases, one of the chambers or major vessels (usually pulmonary artery) may rupture. Generalized edema is frequently found as ascites (uncommon in horses), pericardial or pleural effusion, and edema of the mesentery and subcutaneous tissues. There may be evidence of vascular congestion of the liver, lungs, and spleen. The kidneys may be pale and swollen and have an irregular, granular, pitted surface.
Microscopically the lesions of cardiomyopathy are characterized as myocardial vacuolation and degeneration with necrosis and fibrosis. Calcification may be associated with these lesions. Occasionally there is increased vascularization with proliferative regeneration of myofibers. Loss of cardiac myocytes and replacement by fibro-fatty tissue occurs in horses with arrhyth- mogenic right ventricular cardiomyopathy.187 189 In some cases of cardiomyopathy, no histopathologic abnormalities are found.
Treatment and Prognosis
Treatment of myocarditis includes treating the underlying causative agent if it is recognized and controlling complications such as arrhythmias, CHF, or shock. Thromboembolism is rarely a complication recognized in animals. Prompt administration of vitamin E may be beneficial to the survivors in cases of ionophore toxicosis. Performance animals should be rested. Corticosteroids may be beneficial in animals with severe toxemia, complicated arrhythmias, or intractable heart failure, but their use in early cases of myocarditis or in infections suspected of having a viral cause is controversial because viral recrudescence may occur. However, in many cases corticosteroids appear to have a beneficial effect. Prognosis is good if there are no signs of heart failure and if cardiac arrhythmias are managed successfully. Prognosis is guarded to poor if signs of CHF are present.
Therapeutic strategies currently used for treatment of dilated cardiomyopathy include positive inotropic agents (digoxin), diuretics, vasodilators, rest, and in some cases removal of pleural or abdominal fluid. The advantages of vasodilators (venodilators to relieve pulmonary edema and arterial dilators to reduce preload and afterload and improve contractility) in the treatment of cardiomyopathy are recognized in humans 199
and small animals.199
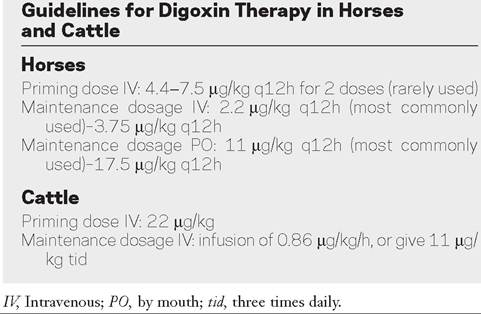
Digoxin is the positive inotropic agent used almost exclusively in large animals but is contraindicated in animals with acute monensin toxicosis. A priming or loading dose can be used in horses with acute severe CHF, followed by a maintenance dose, or more frequently, the horse is started on a maintenance dose from the onset of therapy. In horses, the drug can be administered PO or parenterally. In cattle, low bioavailability limits its use to the IV route of administration.177 Guidelines for the use of digoxin are given in Box 30.1.141,200,201 In general, maintenance dosages are used because of the lowered risk of adverse reactions. A peak and trough serum digoxin concentration should be obtained 3 to 5 days after digoxin therapy is begun, and the dosage should then be adjusted accordingly. Ideally, the trough and peak digoxin concentration should be between 1 and 2 ng/mL.
Dehydration, acid-base imbalance, and electrolyte abnormalities should be corrected before digoxin therapy. The dose of digoxin should be decreased in animals with elevated creatinine or blood urea nitrogen (BUN) until these values return to normal. In horses, the IV loading dose of digoxin should be administered slowly or divided and given at a rate of one third of the loading dose hourly until completion.200 Alternatively, therapy can be initiated with the maintenance dose. Close monitoring of body weight, appetite, electrolyte concentrations, creatinine or BUN concentration, and cardiac rhythm is essential during therapy. Therapeutic drug monitoring with digoxin plasma concentrations can be helpful during initial therapy, when the volume of distribution of the drug and the patient's body weight may be in a state of flux. Samples for determination of peak serum digoxin concentrations should be obtained 1 to 2 hours after digoxin administration and should not exceed 2.5 ng/mL.141,202
The diuretic used most commonly in large animals is furosemide. It is administered parenterally at the rate of 1 mg/ kg twice daily or as needed to control edema. Oral absorption of furosemide is poor or variable in horses.140 A continuous-rate infusion of furosemide is recommended in horses when rapid profound diuresis is needed.203 The half-life and diuretic effect of bumetanide, a sulfonamide diuretic, are shorter than those of furosemide in horses.204 The PK/PD information about torsemide, a new loop diuretic that is much more potent than furosemide, indicates it may be a better diuretic for long-term diuresis in horses.205 The recommended dosage is 0.5 to 1 mg/kg orally twice daily, which should be adjusted accordingly thereafter. Electrolyte concentrations and water consumption should be monitored closely in patients receiving diuretics.
The vasodilator used most frequently in horses in the United States is the ACE inhibitor benazepril. However, the cost of the ACE inhibitors varies wildly in different countries, so other ACE inhibitors or hydralazine are often used because of cost and availability issues. Other ACE inhibitors that have been used but are less effective include quinapril, ramipril, and enalapril. These vasodilators have resulted in clinical improvement in animals treated for CHF. Benazepril at 1 mg/kg PO twice daily has recently been shown to be most effective at suppressing ACE activity.145,150 Quinapril at a dose of 0.25 mg/kg PO once daily has also been shown to increase stroke volume and cardiac output in horses with MR after 8 weeks of therapy.146 Ramipril resulted in clinical and echocardiographic improvement of a horse with CHF at a dosage of 50 μg∕kg daily PO.149 Enalapril has been used at a dose of 0.5 mg/kg PO twice daily in the management of horses with moderate to severe MR or AR and in the treatment of horses with CHF. However, after a single 0.5-mg/kg oral dose of enalapril, neither enalapril nor enalaprilat was detectable in the serum, and ACE activity was not significantly reduced.147 Hydralazine is administered PO at a dose of 0.5 to 1.5 mg/kg twice daily.
Control of cardiac arrhythmias should be attempted in animals that are hemodynamically unstable or threatened with development of worsening arrhythmias. Quinidine is usually the drug of choice for control of atrial and VA in cattle and is one of the drugs of choice in horses. Procainamide, lidocaine, propafenone, phenytoin, and sotalol have also been successful in treating VA in horses (Table 30.3). Although flecainide has been used successfully in horses, its use is not recommended due to the risk of sudden cardiac arrest. Although administration is limited to the IV route in cattle, oral or IV administration in horses results in adequate plasma concentrations to control arrhythmias. Quinidine is administered IV by infusion or divided bolus injections as shown in Box 30.2.
When quinidine is used IV, concurrent IV administration of a balanced electrolyte solution at the rate of 3 to 4 mL/ kg/h may be desirable to maintain blood pressure in animals with severely compromised cardiovascular status.
Prognosis for animals with dilated cardiomyopathy is poor. Echocardiography is useful in determining the severity of the myocardial dysfunction and in formulating a prognosis. The results of the initial echocardiographic examination were the best prognostic indicator of survival in a recent outbreak of monensin toxicosis.177 Recovery of animals with cardiomyopathy is unusual, constant therapy is required for maintenance of animals with CHF, and sudden death can occur at any time. Some animals may have significant myocardial dysfunction without CHF and are “cardiac cripples,” comfortable at pasture but not safe to use for performance. These animals may later develop CHF.
Prevention and Control
Maintenance of a good vaccination program may limit the bacterial and viral causes of myocarditis. Parasite control may also reduce myocardial injury that predisposes to myocarditis or cardiomyopathy in horses. Toxic myocardial diseases are prevented by making horse feed in mills where feeds containing
■ TABLE 30.3
Drug Therapy for Ventricular Tachycardia
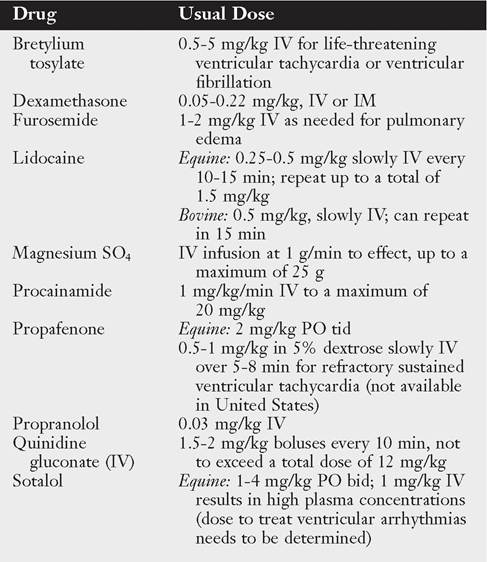
bid, Twice daily; IM, intramuscular; IV, intravenous; PO, by mouth; tid, three times daily.
■ BOX 30.2
Quinidine Administration in Horses and Cattle Horses
IV: 1.5-2 mg/kg every 10 min until conversion or desired effect,
not to exceed a total dose of 12 mg/kg
PO: 22 mg/kg (1 g/100 lb of body weight) q2h until conversion or desired effect, not to exceed a total dose of 132 mg/kg q2h. If quinidine plasma concentrations cannot be obtained promptly, a total dose of 88 mg/kg q2h should not be exceeded.
Cattle
IV: 48 mg/kg infused IV over a 4-hr period
IV, Intravenous; PO, by mouth.
ionophores are not made, by proper mixing of feeds containing monensin, salinomycin, or lasalocid in feed mills in which horse feed is made, by not shipping bulk horse feed in trucks in which medicated ionophore-containing feed has been transported, and by preventing horses from ingesting these medicated feeds. Gossypol toxicity can be prevented by feeding no cottonseed meal or cottonseed meal with low gossypol content, especially when feeding preruminants.206 Feeding of cottonseed meal can be limited by providing more forage or additional protein sources in the diet of ruminants so that ingestion of gossypol is limited to concentrations of 1 to 2 g/kg or less of feed for adult cattle and 0.5 to 1 g/kg or less of feed for immature cattle.207 Nutritional myocardial disease can be prevented by adequate feeding of vitamin E, selenium, and copper with supplementation as required. Inherited cardiomyopathy is controlled by avoiding breeding of known or suspected carriers of the polled Hereford and Holstein-Friesian breeds. Not grazing horses on pastures containing Acer spp. will eliminate myocardial injury associated with consumption of the hypoglycin A toxin that
p 208 ypgy causes atypical myopathy.208