CONSTIPATION
Constipation is defined as absent, infrequent, or difficult defecation. Obstipation is intractable constipation and results in severe fecal impaction throughout the rectum and colon (Figure 1-19).
Both conditions should be differentiated from megacolon, which is a clinical disorder characterized by chronic dilation and hypomotility of the colon and rectum. Not all patients with constipation have megacolon. Constipation is a common problem in dogs and cats. This problem is discussed in detail in Chapter 8. The causes and treatment of constipation are listed in Tables 8-3 and 8-4, respectively.The main consideration discussed here is the importance of a careful review of the history and
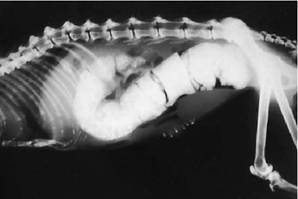
Figure 1-19 Severe obstipation in a 16-year-old cat with idiopathic megacolon.
physical examination by the clinician when an owner believes that his or her pet is constipated. Whenever possible, owners who telephone the clinician to describe their pet's symptoms of straining should be encouraged to bring their pets for an examination unless past pertinent history is well known by the clinician and the likelihood of what the problem is can be accurately assessed without an examination. It is extremely important that urethral obstruction in cats and dogs (a potentially life-threatening problem) be differentiated from straining related to constipation, proctitis, colitis, or other less worrisome causes. The caudal abdomen is palpated for evidence of an enlarged and difficult-to-express urinary bladder, distended colon with hardened stool, colonic sensitivity (often increased in patients with colitis), and any masses that might be present. A small, painful bladder suggests cystitis or cystic calculi. If the alimentary tract seems to be the cause of the problem, a rectal examination is mandatory to evaluate mucosal sensitivity and texture, to evaluate presence and consistency of fecal material in the rectal canal, and to look for evidence of obstruction (stricture, mass, prostatomegaly, foreign body, perineal hernia).
Once the initial physical assessment is completed, a more detailed line of questioning can begin based on the problem that has been identified (i.e., constipation versus some other cause of straining). Important areas to investigate for the problem of constipation include diet, environment (e.g., likelihood of ingestion of foreign body material, ready access to clean litter for cats), normal defecation habits, exercise patterns, drug therapy, and any history of sacrocaudal or pelvic trauma. Because some patients with constipation do not strain to defecate, it is important that owners become familiar with their pet's normal defecation patterns (frequency, amount, time of day). This is especially important regarding cats with megacolon. It is useful to teach owners of cats with a history of a constipation problem how to palpate the colon so that they can recognize a state of constipation early enough to seek treatment, well before development of obstipation.
Diagnostic testing during the initial detailed assessment of the patient should include a CBC, biochemical profile, urinalysis, and thyroid studies. These tests are done to investigate for systemic problems that can cause colonic inertia (peripheral neuropathies, hypercalcemia, hypokalemia, hypothyroidism). Survey radiographs of the abdomen, lumbosacral spine, and pelvis are made to confirm the presence and assess the degree of constipation and to look for evidence of such causes as prostatomegaly, enlarged sublumbar lymph node, presence of a mass, narrowed pelvic canal, and stricture (Figure 1-20). Colonoscopy is not commonly required in patients

Figure 1-20 Severe obstipation in a 13-year-old spayed female DSH cat. Note that the fecal column ends abruptly ventral to L6. There are small radiopaque densities posterior to the fecal column that are presumably in the colon. Enemas and transabdominal manual manipulation performed under sedation failed to move the fecal mass any closer to the anus.
Exploratory laparotomy revealed an annular constricting lesion in the colon approximately 4 cm proximal to the rectum. The histologic diagnosis was adenocarcinoma. Mesenteric lymphadenopathy and extensive nodular involvement in the mesentery were also found. The annular adenocarcinoma in the colon caused nearly complete obstruction of the descending colon. In cats with idiopathic constipation and obstipation, the fecal mass generally extends into the rectum (see Figure 1-19). with constipation. The primary indication would be to evaluate an intraluminal mass or stricture site. Ultrasonography may be useful for localizing a site of obstruction.Treatment
The treatment of constipation and obstipation is reviewed in detail in Chapter 8. Treatment often involves dietary manipulation (high-fiber diets) used alone or in combination with stool softeners. The promotility drug cisapride, used in conjunction with a stool softener such as lactulose, is often effective in managing colonic inertia problems. Manual deobstipation under general anesthesia is generally required in dogs and cats with severe constipation or obstipation. Balloon catheters for dilation of colonic strictures are available and are used under endoscopic guidance. Surgery is required for removal of masses, severe benign strictures and any malignant stricture, and some foreign body impaction cases. Colectomy may be indicated for the occasional cat with megacolon that does not respond to combination therapy using cisapride, stool softeners, and dietary management.
References
Beaver BV: Feline ingestive behavior. In Beaver BV, ed: Feline behavior: a guide for veterinarians, Philadelphia, 1992,WB Saunders.
Berk JE: Gaseousness. In Berk JE, Haubrich WS, eds: Gastrointestinal symptoms, Philadelphia, 1991, BC Decker.
Burbridge HM, Guilford WG: Barium-impregnated polyethylene spheres (BIPS): clinical observations, Vet Radiol Ultrasound 37:79,1996.
Burrows CF: Diarrhea in the dog: a clinical perspective.
In Viewpoints in veterinary medicine, ed 2, Lehigh Valley, Pa, 1993, Alpo Petfoods.Burrows CF: Vomiting and regurgitation in the dog: a clinical perspective. In: Viewpoints in veterinary medicine, ed 2, Lehigh Valley, Pa, 1993, Alpo Petfoods.
Dean PW, Bojrab MJ: Defecation and fecal continence. In Bojrab MJ, ed: Disease mechanisms in small animal surgery, Philadelphia, 1993, Lea & Febiger.
Friedman G: Diet and irritable bowel syndrome. In Friedman G, ed: The irritable bowel syndrome: realities and trends, Gastroenterol Clin North Am 20:313, 1991.
Giffard CJ et al.: Administration of charcoal, Yucca schidi- gera, and zinc acetate to reduce malodorous flatulence in dogs, J Am Vet Med Assoc 218(6):892, 2001.
Guilford WG:Approach to clinical problems in gastroenterology. In Guilford et al., eds: Strombeck' small animal gastroenterology, ed 3, Philadelphia, 1996,WB Saunders. Giulford WG, Lawoko C: Validation of radiopaque markers for assessment of gastric emptying rates of food in dogs, J Vet Intern Med 10:170,1996.
Hedlund CS: Surgery of the perineum, rectum, and anus. In Fossum TW, ed: Small animal surgery, St. Louis, 1997, Mosby.
Lorenz MD: Coprophagy and pica. In Lorenz MD, Cornelius LM, eds: Small animal medical diagnosis. Philadelphia, 1987,JB Lippincott.
Luescher UA, McKeown DB, Halip J: Stereotypic or obsessive-compulsive disorders in dogs and cats. InVoith V, Marder A, eds:Advances in companion animal behavior, Vet Clin North Am Small Anim Pract 21:401,1991.
Niebauer GW: Rectoanal disease. In Bojrab MJ, ed: Disease mechanisms in small animal surgery, Philadelphia, 1993, Lea & Febiger.
Polsky R: Electric shock collars: are they worth the risks? J Am Anim Hosp Assoc 30:463, 1994.
Richter KP: Diseases of the rectum and anus. In Kirk RW Bonagura JB, eds: Current veterinary therapy XI, Philadelphia, 1992,WB Saunders.
Tams TR: Endoscopic examination of the small intestine. In Tams TR, ed: Small animal endoscopy, ed 2, St. Louis, 1999, Mosby.
Tams TR: Gastroscopy. In Tams TR, ed: Small animal endoscopy, ed 2, St. Louis, 1999, Mosby.
Tams TR: Vomiting, regurgitation, and dysphagia. In Ettinger SJ, ed: Textbook of veterinary internal medicine, ed 4, Philadelphia, 1995,WB Saunders.
Willard M: Clinical manifestations of gastrointestinal disorders. In Nelson RW, Couto CG, eds: Small animal internal medicine, ed 2, St. Louis, 1998, Mosby.