RADIOLOGY OF THE DIGESTIVE SYSTEM
Pharynx
Radiographic Anatomy
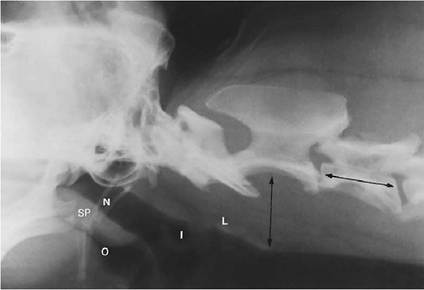
The air-filled pharynx provides contrast for visualization of the soft palate, epiglottis, hyoid apparatus, and retropharyngeal area. Therefore any changes in shape, size, or opacity of these structures can be readily discerned.
The pharynx is divided into four anatomic regions (Figure 2-1): nasopharynx—the area between the soft palate and the base of the skull; oropharynx—the area between the soft palate and the base of the tongue; pharyngeal isthmus—caudal to the soft palate and cranial to the larynx; and laryngopharynx—dorsal to the larynx and ventral to the second cervical vertebra (position varies slightly in different species and breeds).The craniocaudal limits of the retropharynx extend from the caudal border of the pharyngeal isthmus to the level of the third cervical vertebra. The dorsoventral limits are ventral to the cranial cervical vertebra and dorsal to the larynx. A general guideline for the normal dorsoventral dimension of the retropharynx is that it should be no greater than the length of the third cervical vertebra (see Figure 2-1).
swallowing is a dynamic process that is best assessed fluoroscopically while administering radiopaque contrast medium. There are three phases in normal swallowing: oral—action of the tongue forms the bolus; pharyngeal—propulsion of the bolus from the base of the tongue to the
Figure 2-1 Normal pharynx: nasopharynx (N), soft palate (SP), oropharynx (O), pharyngeal isthmus (I), and Iaryngopharynx (L). The width of the retropharyngeal area should be no greater than the length of the third cervical vertebra (arrows).
laryngopharynx; and cricopharyngeal—the cricopharyngeal sphincter opens as the isthmus contracts, to allow passage of the bolus into the esophagus.
The sphincter rapidly closes after the bolus moves into the esophagus.Pharyngeal Contrast Study
Indications include dysphagia, excess salivation, cough, pain, visible tissue swelling, and suspected foreign object.
The following materials are needed for a pharyngeal contrast study: thick barium paste,[*] [†] 100% micropulverized barium sulfate or barium-food mixture1; water-soluble iodinated contrast (used if perforation is suspected)*; and a dose syringe.
Administer the contrast medium orally in the buccal pouch. Obtain lateral and ventrodorsal (VD) views. Make the exposures while the patient is swallowing.
A normal-appearing contrast study of the pharynx shows smooth coating of the pharyngeal mucosa, absence of pooled contrast medium in the pharynx, and no reflux of contrast medium into the nasopharynx or trachea.
Radiographic Signs of Pharyngeal Disease
Mass Lesions. Common causes of mass lesions in the pharynx include abscess, neoplasia, cyst, foreign object, granuloma, and inflammation.
Abnormal location of soft tissue or mixed opacities (mineral, fat, fluid, and/or gas) may be visualized. These opacities may cause compression of or may impinge on the normally gas-filled pharynx (Figure 2-2). Closely evaluate the VD view for asymmetric opacities in the pharyngeal and laryngeal areas (many lesions are unilateral). Contrast studies may show compression or extravasation.
Swallowing Disorders. Oral dysphagia is related to functional impairment of tongue movement. Radiographically, poor bolus formation is seen

Figure 2-2 A soft tissue mass is seen impinging on the nasopharynx (arrowheads). This mass was a tonsillar carcinoma.
from the base of the tongue caudally. Aspiration pneumonia is rare in oral dysphagia.
Pharyngeal dysphagia results in decreased pharyngeal peristalsis. Weakened contractility impairs movement of a bolus through the pharynx.
On the survey film the pharynx may appear distended with gas. Contrast medium is retained in the oropharynx, pharyngeal isthmus, laryngopharynx, and piriform recesses. Contrast medium can be seen in the trachea. Aspiration pneumonia is often seen in pharyngeal dysphagia.Cricopharyngeal dysphagia is due to insufficient relaxation of the cricopharyngeal sphincter. This is the most common form of oropharyngeal dysphagia (Figure 2-3). On the survey film, gas may be seen in the cervical esophagus. There is contrast reflux into the nasopharynx and trachea, and there is contrast retention in all other pharyngeal regions. Aspiration pneumonia may be seen in cricopharyngeal dysphagia.
Esophagus
Radiographic Anatomy
Because the esophagus has the same opacity as that of surrounding soft tissue structures in the neck and mediastinum, it is not usually seen on survey radiographs. However, normal transient dilation of an air-filled esophagus may be visualized. Common nonpathologic causes of air in the esophagus include aerophagia, anxiety, dyspnea, and anesthesia.
On the lateral view the cranial thoracic esophagus is dorsal to the trachea, and caudally it is located about halfway between the aorta and the

Figure 2-3 A dog with cricopharyngeal achalasia. There is accumulation of contrast medium in the pharyngeal isthmus (I). Some contrast medium is present in the esophagus, but there is considerable accumulation in the trachea.
vena cava. On theVD view the esophagus is to the left of the trachea, approximately on midline.
Esophagram
Indications include regurgitation of undigested food, persistent vomiting or gagging, suspected foreign object or mass, and assessment of position or compression of the esophagus.
The following materials are needed for an esophagram:
1. A dose syringe.
2. Barium paste, micropulverized barium suspension, or a food-barium mixture.
Barium paste offers the best mucosal coating and should be used to evaluate suspected mucosal or mass lesions. Liquid barium suspension is used to evaluate an enlarged esophagus because a large volume may be required to fill the esophagus. A food-barium mixture is used to evaluate motility because peristalsis may be adequate for liquids and insufficient for solid food. Some strictures may allow fluid to pass normally but will restrict passage of solid food.3. Aqueous organic iodide (used if perforation is suspected).
Administer the contrast medium orally in the buccal pouch.The dose is approximately 10 to 20 ml, to be administered before each exposure. Obtain lateral and VD oblique views (esophagus and spine are superimposed on the straight VD view).
In the dog a normal esophagram shows barium outlining longitudinal, parallel folds and a small diverticulum at the thoracic inlet (Figure 2-4); the diverticulum is more pronounced in brachycephalic breeds.
In the cat a normal esophagram shows a cranial esophageal mucosal pattern that is similar to that of the dog; caudally the mucosa has transverse mucosal folds, referred to as a herringbone pattern (Figure 2-5). Esophageal distention by a bolus of contrast medium in transit may be seen in all patients.
Radiographic Signs of Esophageal Disease
Megaesophagus (Figure 2-6). Megaesophagus appears as an enlarged esophagus containing fluid, ingesta, or air. There is ventral deviation of the trachea. A “tracheoesophageal stripe”—a thickened soft tissue opacity composed of dorsal tracheal wall and ventral esophageal wall—is more often seen on the left lateral view. The “stripe” is visible when there is air in the esophagus, as well as in the trachea. On the VD view the terminal esophagus
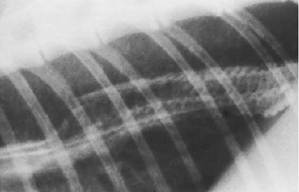
Figure 2-5 Close-up view of a normal barium study of the caudal feline esophagus. Note the normal transverse mucosal folds outlined by barium.
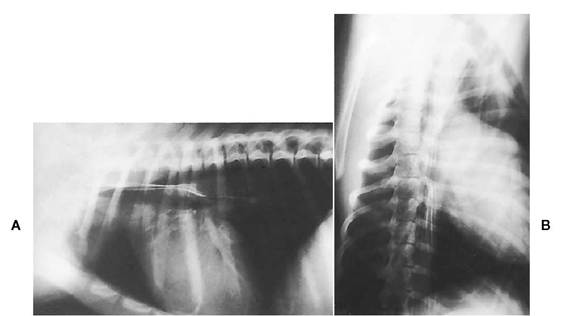
Figure 2-4 A, Lateral view of a normal canine esophagram. Note the normal longitudinal folds outlined by contrast medium. B, Ventrodorsal oblique view of a normal canine esophagram. The patient is at an oblique angle to avoid summation of the spine and esophagus.
tapers into the diaphragm. Evidence of aspiration pneumonia may be present.
Vascular Ring Anomalies (Figure 2-7). Dilation of the esophagus cranial to the heart base is seen. The caudal esophagus is usually of normal size but may be enlarged. There is ventral depression of the trachea. The aorta may descend on the right side. The contrast study shows stricture at the heart base, and the aorta compresses the esophagus on the right side. Evidence of aspiration pneumonia may be present.
Esophageal Foreign Objects (Figure 2-8). A radiopaque foreign object is often visible. Esophageal dilation may be seen proximal to the obstruction. There may be mediastinitis, pleuritis, and pneumomediastinum if the esophagus has been perforated. On the esophagram, barium surrounds the intraluminal filling defect. Esophageal stricture is a potential sequela.
Esophagitis. On the contrast study there is prolonged retention or pooling of barium in the affected area of the esophagus. The normal linear mucosal pattern is indistinct, blurred, or completely absent.Abnormal motility is present on fluoroscopy.
Esophageal Neoplasia (Figures 2-9 and 2-10). A soft tissue mass may be seen on survey radiographs in the area of the esophagus. The opacity may be homogeneous or may contain air or calcification. Dilation proximal to the mass may be present. Diverse changes seen on the contrast study, depending on the nature of the mass, include irregular or smooth mucosal pattern, wall rigidity, wall thickening, luminal lucent filling defect (protruding mass), and extravasation of contrast medium into the mass.
Stomach
Radiographic Anatomy
Complete evaluation of the lateral abdominal view includes appraisal of the stomach axis.
The stomach axis is a line drawn from the fundus to the body of the stomach. The normal axis is roughly parallel to the ribs. Changes in the stomach axis correspond to changes in liver size. The pylorus and body are displaced caudally if the liver is enlarged, and they are displaced cranially if the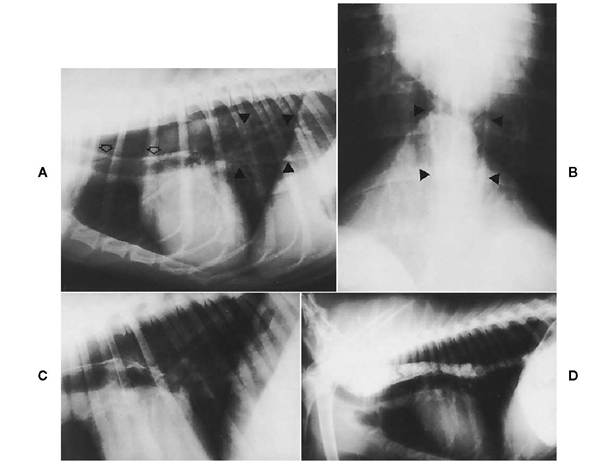
Figure 2-6 A, Lateral view of a dog with megaesophagus. The trachea is ventrally depressed by an enlarged, airfilled esophagus. Note the “tracheoesophageal stripe” (open arrows), which is seen when air is in the esophagus as well as in the trachea. Dorsal and ventral esophageal walls are seen caudally (arrowheads). B, Ventrodorsal view of the dog in A. This view is centered on the caudal esophagus. The air-filled esophagus appears as two linear opacities on either side of midline that taper into the diaphragm (arrowheads). C, Lateral view of a dog with mild megaesophagus. No abnormalities are seen with barium liquid. D, Same dog as in C. When food-barium mixture is used, esophageal dilation is seen, suggesting abnormal esophageal motility. Use of food mixed with barium should be considered when evaluating esophageal swallowing dysfunction.
liver is small or has herniated through the diaphragm into the thorax.
On the VD view the stomach position in the dog is slightly different from that in the cat: In the dog the fundus is cranial-left, the body is midline, and the pylorus is cranial-right. In the cat the fundus and body are cranial-left and the pylorus is midline or slightly to the right of the spine.
Stomach location varies with stomach distention, but the stomach is usually between the tenth and thirteenth ribs. Competent assessment of liver size and diagnosis of liver masses depend on knowledge of normal stomach position.
The variably sized stomach may contain non- persistent air, fluid, or mineral opacities. The wall of the fundus has pronounced rugal folds that appear uniform and parallel in a distended stomach and undulant and tortuous in a nondistended stomach. The rugal pattern is negligible in the body and pyloric areas of a normal stomach.
Gastrogram
Indications include chronic vomiting, hemateme- sis, suspected foreign object or mass, pyloric disease, and identification of stomach position.
The following materials are needed for a gas- trogram: micropulverized barium suspension diluted to 50% with warm water; gas source (room air, carbonated beverage, gas-producing tablets or granules); water-soluble iodinated contrast medium (used only if a gastric perforation or rupture is suspected); and a stomach tube, mouth gag, and large-dose syringe.
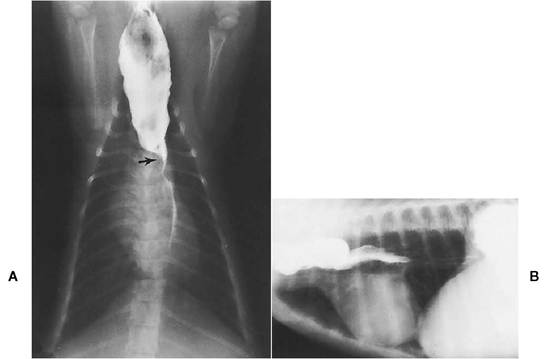
Figure 2-7 A, Ventrodorsal view of a cat with persistent right aortic arch. Note the abrupt change in diameter of the esophagus at the heart base. The right aortic arch compresses the esophagus, causing deviation of contrast medium to the left (arrow). B, Lateral view of a dog with persistent right aortic arch. Contrast medium outlines the dilated cranial thoracic esophagus. There is a change in esophageal diameter at the heart base. The esophagus is partially dilated caudal to the vascular ring anomaly.
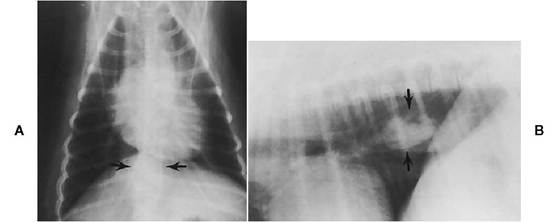
Figure 2-8 Survey ventrodorsal (A) and lateral (B) views of a dog with an esophageal foreign object. An opacity is located in the area of the caudal esophagus on both views (arrows). Two views are necessary to determine the exact location of soft tissue opacity.
In a positive or negative gastrogram the following technique is best used to identify stomach position or gastric foreign objects:
1. The stomach should be empty.
2. Use the following doses: for barium, 1.5 to 2 ml of previously diluted (50%) micropulverized barium per lb; for room air, 1.5 to 2 ml of air per lb; for oral iodinated contrast, 0.7 ml of iodinated contrast mixed with 0.7 ml warm water per lb.
3. Administer the contrast medium via a stomach tube rather than orally to achieve maximum stomach distention. Make sure that the tube is not in the trachea (by palpation or radiograph).
4. Obtain right and left lateral views, VD and dorsoventral views, and additional oblique views as needed.

Figure 2-10 Lateral view of a cat with esophageal neoplasia. Irregular and asymmetric filling defects are in the midcervical esophagus. Contrast medium extends around the mass, suggesting a broad-based intramural mass. Diagnosis was an esophageal carcinoma.
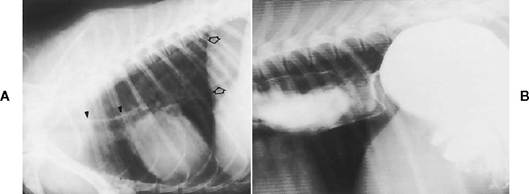
Figure 2-9 A, Lateral view of a dog with megaesophagus. The trachea is ventrally depressed by an air-filled esophagus. A “tracheoesophageal stripe”is seen (closed arrowheads), and the caudal esophagus is dilated (open arrows). No obvious cause for the dilated esophagus is seen. B, Lateral esophagram of dog in A. A smooth, curvilinear filling defect is in the caudal esophagus, which is caused by an intramural esophageal mass located proximal to the gastroesophageal junction. Contrast studies should be performed to determine the cause of megaesophagus. Diagnosis was leiomyosarcoma.
In a double-contrast gastrogram, which is the best method for evaluating mucosal lesions, mural masses, and ulcerations, the following technique is used:
1. The stomach must be empty.
2. Via a stomach tube, give 0.25 ml diluted (50%) barium per lb followed by 1 to 1.4 ml gas per lb.
3. Obtain right and left lateral views, VD and dorsoventral views, and additional oblique views as needed.
A normal-appearing gastrogram (Figure 2-11) shows even gastric distention; smooth parallel rugal folds in the fundus, not in the body or pylorus (guideline: a rugal fold should be no thicker than the space between the folds); smooth mucosal surface; transient peristalsis in the body and pyloric areas; and stomach beginning to empty within 30 minutes and empty by 1 to 4 hours (normal stomach emptying of food is 5 to 6 hours but may be as long as 8 to 10 hours in some patients and still be considered normal).
Radiographic Signs of Gastric Disease
Pylorospasm. A pylorospasm is indicated by delayed gastric emptying and gastric dilatation with visible peristalsis.
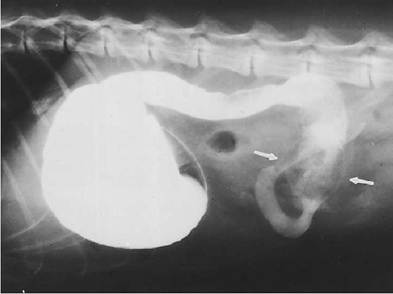
Pyloric Stenosis. This disease may be congenital or acquired. Common causes of acquired stenosis include pyloric neoplasia, chronic hypertrophic gastritis, and uremic gastritis (Figure 2-12). Radiographic signs are delayed gastric emptying; gastric dilatation with peristalsis usually present; narrowed pylorus with contrast medium projecting into the pyloric canal (beak sign); and often the development of a distinct bulge in the stomach immediately proximal to the pyloric canal, especially on the lesser curvature.
Gastric Foreign Objects (Figures 2-13 and 2-14). Radiopaque foreign objects are often visible on survey radiographs. On a barium study soft tissue or air-filled foreign objects appear as lucent filling defects. The foreign object is usually freely movable in the stomach and changes location on different radiographic views.
Gastritis. This diagnosis is suggested when one or more of the following radiographic changes are evident (Figure 2-15):
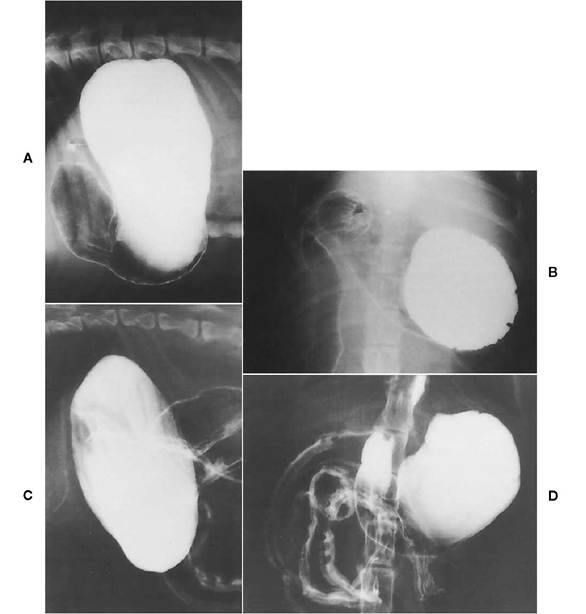
Figure 2-11 Lateral (A) and ventrodorsal (B) views of normal canine double-contrast gastrogram. Contrast medium is pooling in the fUndus. Note the smooth mucosal surface and peristalsis in the body of the stomach. Filling defects seen in the wall of the fundus on the ventrodorsal view are normal rugal folds. Lateral (C) and ventrodorsal (D) views of normal feline double-contrast gastrogram. Rugal pattern, seen as lucent linear filling defects, is normally more evident in the fundus. Note that the cardiac area is slightly irregular.This is a normal finding in cats.
1. Thickened, irregular, or indistinct rugal folds
2. Prominent rugal folds in the pylorus and body
3. Rigid stomach wall that is nondistensible, is often thickened, and lacks peristalsis
4. Hyperperistalsis or hypoperistalsis
5. Barium precipitation caused by abnormal stomach contents, such as blood, excess mucus, or incorrect pH
6. Stomach emptying that is delayed or more rapid than normal
7. Calcification of gastric mucosa, secondary to chronic renal disease, appearing as faint linear opacities that accentuate rugal folds on survey radiographs
Gastric Dilatation-Volvulus (Figures 2-16 and 2-17). The following radiographic signs indicate gastric dilatation-volvulus:
1. Gastric dilatation.
2. Compartmentalization of the stomach (double bubble sign) due to the stomach's folding on itself.
3. Pylorus located dorsally and to the left of midline, and fundus located ventrally and to the
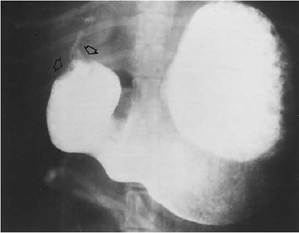
Figure 2-12 A dog with pyloric hypertrophy. A small, annular filling defect (arrows) extends into the pyloric antrum just proximal to the pylorus. A small amount of barium extends into the pyloric canal.

Figure 2-13 Gastrogram of a dog with a gastric foreign object (ball). The ball appeared as a soft tissue opacity on survey radiographs. When surrounded by barium, the ball appears radiolucent. The lucent filling defect is completely surrounded by barium, suggesting an intraluminal foreign object.
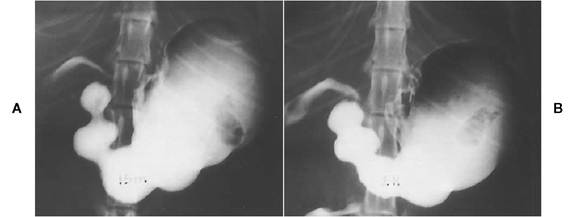
Figure 2-14 A and B, Ventrodorsal views of a cat that swallowed a toy fish. Note the normal irregular cardia. The toy fish is clearly seen as a lucent filling defect in the stomach. Between the two views the position of the toy has changed. This mobility indicates that the object is intraluminal.
right of midline. The fundus is the larger of the two “bubbles” and has a rugal pattern.
4. Splenomegaly caused by venous congestion or possible torsion.
5. Small liver and caudal vena cava caused by portal vein and caval compression by the enlarged stomach.
6. Small intestinal ileus.
7. Dilated esophagus.
Gastric Masses. Gastric masses usually require a barium study for identification and evaluation. Oblique views may be necessary. Because masses vary markedly in appearance, the signs listed below represent possible radiographic appearances (Figures 2-18 to 2-20):
1. Mural thickening.
2. Ulceration, which may be seen as an outpouching of barium beyond the lumen; focal pooling of barium beyond the lumen; or wall rigidity adjacent to the ulcer with a radiating rugal pattern from the site of the ulcer. The rugal pattern may be indistinct, and there may be evidence of perforation and peritonitis.
3. Rigid, nondistensible areas in the stomach.
4. Barium filling defect (lucency) if the mass protrudes into the lumen. The filling defect does not move with gravity on positional studies.
5. Smooth or irregular mucosal surface.
Ruptured Stomach. The radiographic signs of a ruptured stomach include the following:
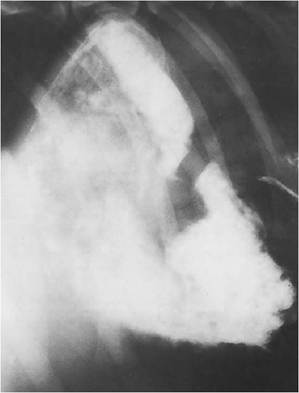
Figure 2-15 Lateral view of a dog with severe ulcerative gastritis. The mucosal margin is irregular, with spicules of barium extending into small ulcers in the stomach wall. This is primarily seen in the body and pyloric antrum. Barium appears smudged, suggesting poor mixing of contrast medium. This is probably due to abnormal stomach contents.
1. Free gas in the abdomen. Small amounts of free gas appear as bubbles outside the lumen and often in abnormal locations, such as near the kidneys or bladder. Larger amounts of free gas outline serosal surfaces of the stomach, intestine, liver lobes, and diaphragm.
2. Ingesta in the abdomen.
3. Indistinct stomach border is seen with large rupture.
4. Poor abdominal visceral detail caused by fluid and/or peritonitis.
5. Contrast extravasation into the abdomen. Use water-soluble iodinated contrast if intestinal rupture is suspected.
Small Intestine
Radiographic Anatomy
The duodenum is located about halfway between the spine and the ventral body wall on the lateral view. It descends along the right body wall and ascends in the midabdomen on the VD view. Jejunum is evenly distributed throughout the abdomen. The ileum is that portion of the distal small intestine that joins with the colon and is located in the right midabdomen.
Intestinal shape is uniform and tubular with transient narrowings due to peristalsis. Intestinal contents include nonpersistent air, fluid, or mineral opacity.
A general guideline used to evaluate intestinal size is that the diameter should be no larger than one to two rib widths or no larger than the height of a lumbar vertebral body (not the vertebral arch or dorsal spine, just the body).
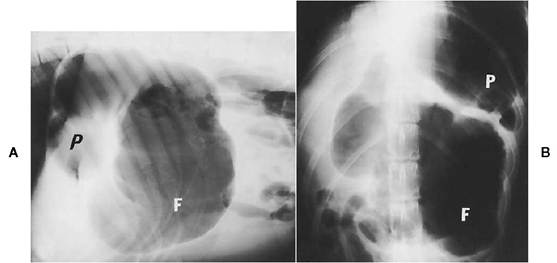
Figure 2-16 Lateral (A) and ventrodorsal (B) views of a dog with gastric dilatation-volvulus. There is compartmentalization of the stomach. The fundus (F) is the largest compartment. The pylorus (P) is displaced dorsally and to the left.
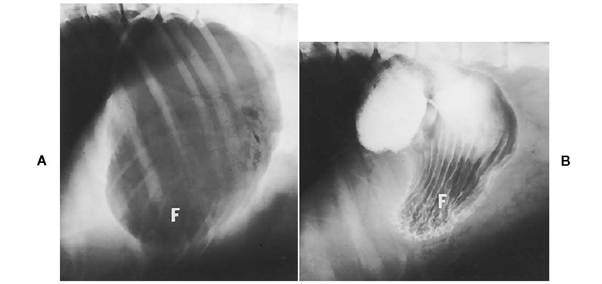
Figure 2-17 Lateral survey (A) and contrast study (B) of a dog with gastric dilatation-volvulus. Rugal folds are identified in the ventrally displaced fundus (F). Pattern of rugal folds is helpful in identifying fundus of stomach.
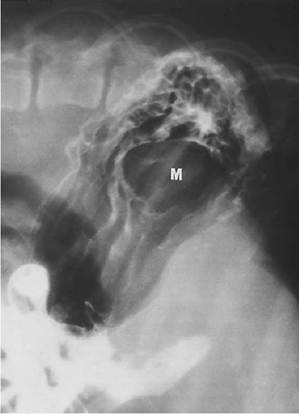
Figure 2-18 Lateral view of a dog with a fundic mass (M) protruding into stomach lumen. The mass causes a lucent filling defect in contrast medium. Rugal folds are distorted by the mass.
Small Intestinal Contrast Study
Indications include persistent vomiting and/or diarrhea, hematemesis, melena, and suspected foreign object or obstruction.
The materials needed for a small intestinal contrast study are micropulverized barium diluted to 50% concentration with warm tap water; watersoluble iodinated contrast if intestinal perforation is suspected; and a stomach tube, large syringe, and mouth gag.
The following technique is used:
1. Administer barium (0.7 to 1.4 ml/lb) orally in swallows or by stomach tube. Use the lower dose for larger dogs to avoid having too much barium in multiple bowel loops and thus to allow adequate evaluation of individual bowel loops.
2. Administer organic iodide (0.25 ml/lb) diluted with tap water (0.5 to 1 ml/lb) orally or by stomach tube. Undiluted organic iodides are extremely hypertonic and can lead to severe dehydration and shock in a compromised patient.
3. If sedation is necessary, studies have shown that acepromazine or triflupromazine can be used in dogs without significantly affecting gastrointestinal (GI) transit time. Recommended sedatives for cats are a ketamine/ace- promazine combination or ketamine alone when motility is not a primary concern (both regimens cause more rapid transit of barium through the GI tract) or ketamine/diazepam if a motility problem is suspected, because there is no significant effect on GI transit time (each sedative should be administered in a separate syringe).
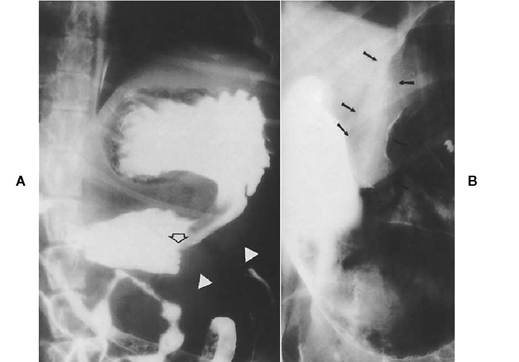
Figure 2-19 A, Ventrodorsal view of a dog with an intramural gastric mass. There is an abrupt change in diameter of stomach lumen (open arrow). This is referred to as a “shelf sign.” Stomach wall is markedly thickened (closed arrowheads). B, An intramural mass is seen on the lesser curvature of the stomach body (arrows). Barium is adherent to an irregular mucosal surface.

Figure 2-20 Barium pools in an ulcer in the gastric fundus (arrow). Note how the rugae radiate from the area of the ulcer.
4. Make exposures in right lateral and VD positions at 0, 15, 30, and 60 minutes (45-minute films may be needed if transit time is rapid). Take films hourly thereafter until the contrast medium reaches the colon.
In a normal-appearing small intestinal contrast study:
1. The mucosal surface is either smooth or finely fimbriated (Figure 2-21).
2. Bowel is evenly distributed throughout the abdomen.
3. The normal feline duodenum may appear hyperperistaltic with multiple simultaneous contractions, giving the appearance of a “string of beads” (Figure 2-22).
4. The normal canine duodenum often has out- pouchings in areas of lymphoid follicles (pseudoulcers) (Figure 2-23).
5. Normal canine small intestinal transit time is 3 to 5 hours for barium to reach the colon.
6. Normal feline small intestinal transit time is 15 to 60 minutes for barium to reach the colon.
7. Organic iodides are irritating and cause hyperperistalsis, so transit time is rapid. Iodinated contrast agents usually reach the colon within 1 hour.

Figure 2-21 Barium contrast study of normal small intestine. The mucosal surface is slightly fimbriated. Lucent areas in the intestine are gas in the lumen. This is differentiated from foreign objects on serial films. Gas opacities are nonpersistent.
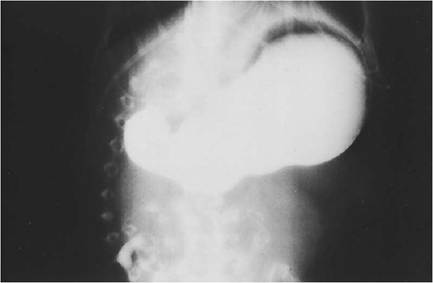
Figure 2-22 Normal feline duodenum with contrast medium. Duodenal hyperperistalsis is a normal finding in many cats. This is referred to as “string of beads” and must not be confused with a linear foreign object (see Figure 2-26).
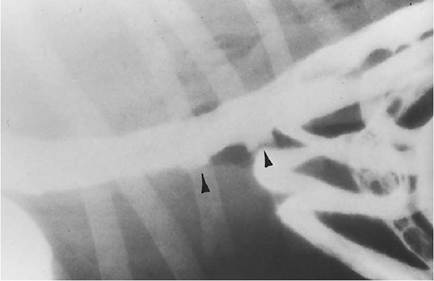
FIGURE 2-23 Pseudoulcers (arrowheads) are normal in the canine duodenum. These appear somewhat conical or square when filled with barium.
Radiographic Signs of Small Intestinal Disease
Excess Gas. Causes of excess gas in the small intestine without dilation include aerophagia, enteritis, anorexia, recent enema, and incomplete or high obstruction where vomition relieves gas/fluid distention; and, with dilation, paralytic ileus, obstructive ileus due to foreign objects, neoplasia, abscess, and granuloma.
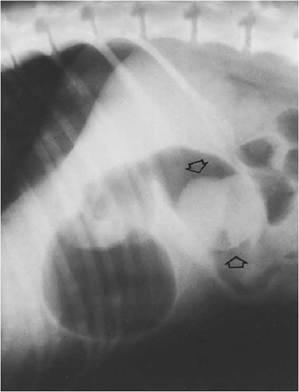
Figure 2-24 There is a smooth soft tissue opacity (foreign object) in the descending duodenum (arrows). This opacity is visible because it is surrounded by air. The duodenum proximal to the foreign object is dilated.
Foreign Objects. Radiopaque foreign objects are visible on survey radiographs (Figure 2-24). Radiolucent foreign objects may be seen on survey radiographs. On a contrast study, foreign objects cause a lucent intraluminal filling defect in the contrast medium (Figure 2-25).
Bowel proximal to the foreign object may be dilated with fluid or gas. If bowel has been perforated, there may be free abdominal gas, loss of abdominal visceral detail, and fluid opacity in the abdomen.
Linear Foreign Objects. Survey radiographs may show numerous end-on loops of small intestine. This is not a definitive sign because hyperperistalsis may give this appearance.
A contrast study reveals plication or gathering of small intestinal loops (Figure 2-26). Do not confuse plication with the normal “string of beads” sign in cats. The “string of beads” appears as a symmetric widening and narrowing of the intestinal lumen. Plicated intestine has a serpentine appearance.
Perforation may occur, causing free gas and/or peritonitis.
Enteritis—Nonulcerative. Radiographic signs of nonulcerative enteritis include rapid intestinal transit time; severe accentuation of the fimbriated villous pattern; persistent narrowing or “stringing” of small intestinal lumen diameter, not to be confused with normal peristalsis; hypercontractility or hyperperistalsis; and precipitation of barium due to abnormal luminal contents, such as blood, excess mucus, or abnormal pH.
Enteritis—Ulcerative (Figure 2-27). Radiographic signs of ulcerative enteritis include severe
Figure 2-25 Barium study of a cat that swallowed a backgammon chip. The duodenum is dilated proximal to the foreign object. Barium surrounds the object (arrows) and then passes into bowel of normal diameter.
bowel spasticity or rigidity and irregular mucosal surface, with contrast medium extending beyond the lumen (in a spiculated pattern if ulcerations are small and diffuse, and with conical, rounded, or squared outlines if the ulcers are larger).

Figure 2-26 Ventrodorsal barium study of a cat with a linear foreign object. Contrast in intestine shows classic accordionated or plicated appearance associated with linear foreign object.
Intussusception. An intussusception is invagination of a segment of intestine into the lumen of an adjoining part of the intestine—usually the proximal segment enters the lumen of the distal segment. The intussusceptum is the invaginated segment. The intussuscipiens is the receiving segment.
On survey radiographs one may see intestinal distention and the intussusceptum may be identified if surrounded by gas.
On an upper GI contrast study, the intestinal transit time is markedly delayed, there is abrupt narrowing of intestinal lumen as barium enters the intussusceptum (Figure 2-28), and intestine proximal to the intussusception is usually dilated.
Intramural Lesions. These can be solitary, multiple, or diffuse. Common causes include neoplasia, granuloma, abscessation, stricture, and adhesions. Radiographic appearance is variable (Figures 2-29 and 2-30):
1. Wall thickness is difficult to assess on survey radiographs because fluid in the lumen adjacent to intestinal mucosa can mimic mural thickening. A contrast study or ultrasound examination is the best way to noninvasively determine actual wall thickness.
2. A mass is visible on survey radiographs.
3. A contrast study may show diffuse or focal increase in wall thickness.
4. A mass may impinge on the lumen concentrically or eccentrically, causing luminal narrowing.
5. Abnormal luminal dilation is seen.
6. A smooth, irregular, or ulcerative mucosal surface is seen. A “scalloped” surface is common

Figure 2-27 Dog with ulcerative enteritis. Mucosal surface has a spiculated appearance due to barium accumulating in small ulcers.
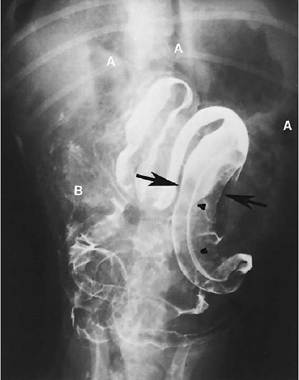
Figure 2-28 Ventrodorsal view of a dog that had surgery 3 days previously to correct an intussusception. Free air (A) is seen in the abdomen, presumably caused by the surgeryA second barium study was performed because of suspected recurrence of intussusception. Arrows indicate lumen of intussuscipiens; arrowheads show lumen of intussusceptum. Free barium seen in the abdomen (B) indicates intestinal rupture.
in multifocal intramural diseases such as lymphosarcoma, pyogranulomatous disease, and diffuse infiltrative diseases.
7. The lesion must be present on more than one film in a barium study to be significant because the radiographic appearance during peristalsis and spasms may mimic that in intramural disease.
Intestinal Perforation (Figures 2-31 and 2-32). Radiographic signs of intestinal perforation include loss of abdominal visceral detail and/or free fluid in the abdomen (suggesting peritonitis); ileus; and free abdominal gas. Small amounts of free gas appear as small extraluminal gas bubbles, usually seen in odd locations, such as near the kidneys or bladder. Larger amounts of free gas outline liver lobes, diaphragm, kidney borders, and serosal surfaces of intestine. A left lateral recumbent view obtained with a horizontal beam shows small amounts of free gas against the right abdominal wall.
Large Intestine
Radiographic Anatomy
The cecum and ascending colon are located in the right midabdomen. The transverse colon parallels the caudal border of the greater curvature of the stomach. The descending colon is in the left abdomen, and the rectum descends into the pelvic canal. The large intestine assumes the shape of a question mark (?) on the VD view. On the lateral view the regions of large intestine are usually superimposed in the midabdomen.
Figure 2-29 Jejunal intramural mass (arrows) is annular and has an irregular mucosal surface. There is minimal distention of intestine proximal to the mass.
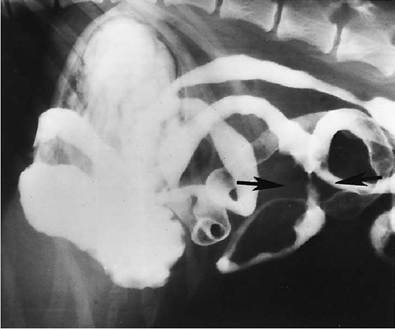

Figure 2-30 Dog with diffuse intestinal lymphosarcoma. The mucosal surface is irregular, with asymmetric filling defects and narrowed areas of small intestine (arrows).
The canine cecum is very large, having a spiral or C shape, whereas the feline cecum is a small blind sac. In the cat there is no distinct border between the cecum and the ascending colon. The junction is defined only by viewing the site where the ileum joins the colon.
Normal size and opacity are extremely variable. Formed feces of heterogeneous opacity, including mineral or bone material, are commonly seen. A large amount of air in the colon can be normal.
Barium Enema
The large intestine should not be assessed on a small intestinal contrast study. Filling is incomplete, and barium inadequately coats large intestinal mucosa.
Indications for a barium enema include recurrent or persistent large bowel diarrhea; fresh blood in the feces; chronic constipation; suspected large bowel obstruction, pelvic masses, colonic or rectal masses, or intussusception; and chronic

Figure 2-31 A, A large amount of free abdominal gas is present (arrowheads). Gas outlines serosa of stomach, abdominal surface of diaphragm, and dorsal caudal abdomen. There is loss of abdominal visceral detail. B, Small amounts of free abdominal gas are more difficult to discern. Several small gas accumulations are seen superimposed over the bladder (arrowheads). These gas opacities are not associated with bowel. There is loss of abdominal detail due to peritonitis and free abdominal fluid.

Figure 2-32 Positional studies are of value in determining the presence of small amounts of free abdominal gas. The patient is placed in left lateral recumbency, and an exposure is made using a horizontal beam. Free abdominal gas accumulates against the abdominal wall (arrowheads).
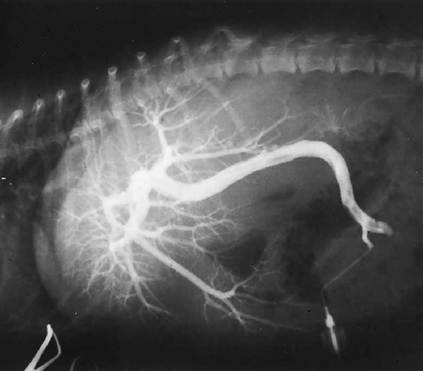
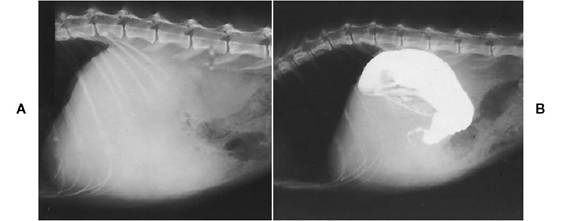
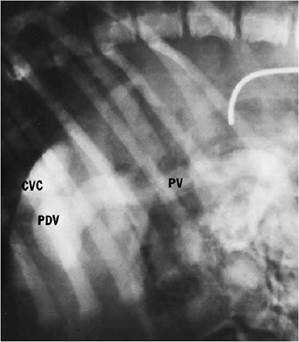
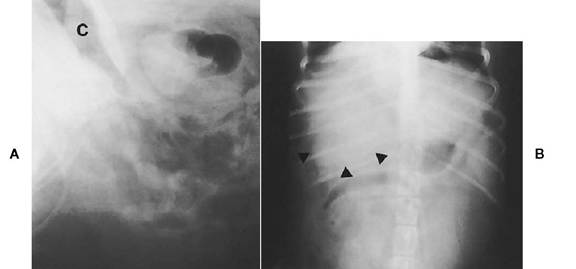
inflammatory large bowel disease. Do not perform a barium enema within 2 hours of enema (spasms induced), 6 to 12 hours after colonoscopy (spasms induced), or within 3 to 4 days after colon biopsy (may rupture colon).
The following materials are needed for a barium enema:
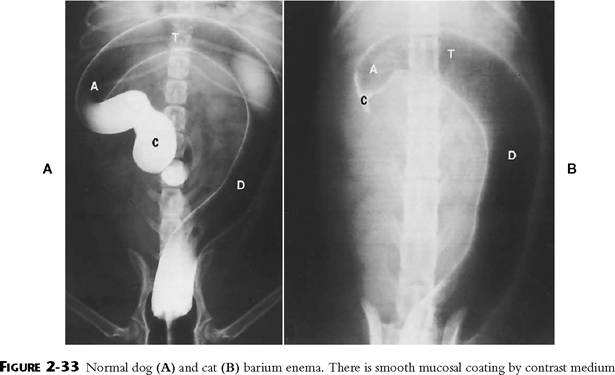
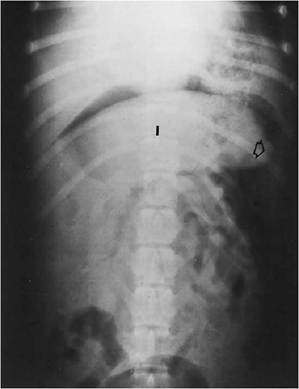
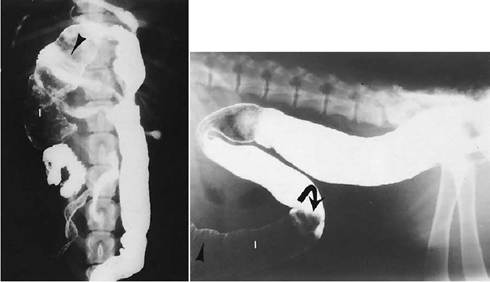
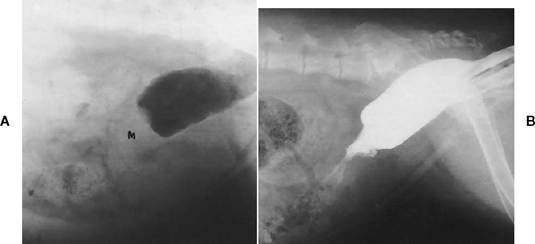
1. Pediatric or adult-sized balloon catheters.*
2. Gravity-flow enema bag with tubing[III] [IV] or dose syringe with adapter and three-way valve. 3. Micropulverized barium diluted to 50% with warm tap water. 4. Aqueous organic iodides diluted to 50% with tap water, used only if perforation is suspected. Barium is the contrast medium of choice to achieve satisfactory mucosal definition. 5. Room air. The following technique is employed for a barium enema: 1. A 24-hour fast is desirable, and multiple high- volume, warm-water enemas are essential to clean out the large intestine. Feces in the colon can obscure small lesions and mimic mass lesions. 2. General anesthesia is desirable to eliminate colonic spasms, facilitate manipulation and positioning, and alleviate patient anxiety and discomfort. 3. Avoid using narcotics that induce severe colonic spasms. 4. Use 2.3 ml/lb of diluted (50%) barium liquid as a general guideline because the dose is extremely variable. Infuse contrast medium slowly through an inflated balloon catheter. 5. Obtain a VD film after 2.3 ml/lb is administered or if there is resistance to flow. Administer more contrast medium as required. 6. Obtain lateral,VD, and two oblique views. 7. Perform a double-contrast study, best for evaluating mucosal detail, by removing most of the positive contrast medium and slowly infusing room air into the colon. Repeat exposures in lateral,VD, and oblique positions. 8. If a rectal lesion is suspected, the balloon catheter may obscure the lesion. A method to outline rectal lesions, if endoscopy is not available, is to inflate the balloon catheter cranial to the lesion, place a purse-string suture around the anus, and tighten the suture after positioning the tip of an additional catheter just inside the anus. A small amount of contrast medium given through the second catheter will outline the extent of a rectal lesion. A normal-appearing barium enema study (Figure 2-33) shows uniform distention of the colon and cecum and a smooth mucosal surface. A redundant or long convoluted colon is a normal variant, and a spasm at the catheter tip is common. Radiographic Signs of Large Intestinal Disease Megacolon or Dilation of Large Intestine. This disease has numerous causes: neurologic disease such as trauma to the spine, spinal neoplasia, or congenital spinal abnormalities; mechanical obstruction such as neoplasia, foreign objects, extrinsic masses compressing or infiltrating the colon wall, or narrowed pelvic canal from malunion of pelvic fractures; abnormal diet; and psychogenic factors. There are no published guidelines for determining megacolon, so diagnosis of abnormal colonic dilation is subjective. Colitis and Typhlitis (Figure 2-34). Radiographic signs of these diseases include mucosal irregularity (“cobblestone” appearance); increased wall thickness; spasticity and shortening of colon and/or cecum; and mucosal ulceration. Emphysematous Colitis. Survey radiographs show gas in the bowel wall. Extensive amounts of gas in the wall parallel luminal gas, in a linear fashion, distinctly showing mucosal surfaces. On a barium study contrast covers the mucosal surface and gas in the colon wall is still visible. Ileocolic Intussusception. On survey films a tubular soft tissue mass outlined by colonic gas may be seen. The leading edge of the intussusceptum has an oval or rounded shape (Figure 2-35). On a contrast study barium surrounds the intussusceptum, which appears as an intraluminal radiolucent filling defect. Barium may define linear bands, sometimes referred to as a “coil spring” appearance, in the wall of the intussus- cipiens, as it contracts on the intussusceptum (Figure 2-36). Colonic or Cecal Intramural Masses. These vary widely in appearance (Figure 2-37). On survey films fecal impaction may occur proximal to the mass. A solid soft tissue mass may be seen; the mass may be focal or diffuse. There is annular constriction or eccentric invasion of the colon by a mass. and even distention of the large intestine. Note the question mark configuration of the canine and feline colon. A, Ascending colon; C, cecum; D, descending colon; T, transverse colon. Figure 2-34 Ventrodorsal view of a dog with severe typhlitis and colitis. Small filling defects are seen protruding into the lumen of the cecum (Ce) and colon (Co). The colon is markedly shortened, and the cecum no longer has a normal shape. Arrow indicates ileocolic junction. Figure 2-35 Ventrodorsal view of a dog with an ileocolic intussusception. The intussusceptum (I) appears as a large soft tissue opacity that is surrounded by air in the intussuscipiens. Note the round contour of the leading edge of the intussusceptum (arrow). Visualization of this abnormal shape is usually associated with intussusception or intestinal foreign object. B Figure 2-36 A and B, Two examples of ileocolic intussusception identified on a barium enema. The intussusceptum (I) appears as lucent filling defect within the colon. Abnormal rounded leading edge is visible (curved arrow). Faint linear bands in the intussuscipiens are outlined by barium (arrowheads). Figure 2-37 A, Survey radiograph of a dog with an intramural colonic mass. Gas is seen in the colon distal to the mass (M), and feces can be seen proximal to the mass. B, Same dog as in A. Barium enema shows an annular colonic mass. Note the abrupt change in colonic diameter caused by the nondistensible intramural mass. On a barium study an irregular or smooth mucosal surface is seen. Ulceration may be diffuse and spiculated or large and cavitated. Polypoid masses cause luminal lucent filling defects on barium study. Liver Normal Anatomy The liver has a soft tissue opacity; therefore internal structures are not defined. Much of the liver is silhouetted by the diaphragm, stomach, and right kidney, making it difficult to evaluate the liver borders. The ventrocaudal liver border is usually well visualized on the lateral view, with sharply defined edges and a triangular shape that projects just beyond the ribs. In the cat the ventrocaudal liver border is often displaced dorsally by falciform fat and may be located in the cranial midabdomen. Normal liver size is best defined by the location of the stomach. On the lateral view the stomach axis from the fundus to the body should be parallel to the ribs, although this varies somewhat with breed, body conformation, and stomach distention. On the VD view an empty stomach is usually located between the tenth and thirteenth ribs. The pylorus and body are located more on midline in the cat. Angiography of the Portal Venous System This is an invasive procedure and is employed less frequently now that ultrasound and nuclear medicine scans are capable of diagnosing vascular anomalies. Indications include suspected congenital or acquired portal vein anomalies, such as patent ductus venosus, portocaval shunts, or portosystemic shunts; and suspected arteriovenous fistulas. The following techniques are used in angiography of the portal venous system: 1. Selective catheterization of the cranial mesenteric artery under fluoroscopic guidance. Because this method requires equipment that is prohibitively expensive for routine private practice, it is not described here. 2. Surgical catheterization of a mesenteric vein, which is invasive but will impart necessary information concerning liver vascular supply. 3. Percutaneous splenic puncture, using an 18- gauge styletted spinal needle,[**] on a patient that is heavily sedated or anesthetized, which will outline most portal shunts. Blood should be easily aspirated before contrast injection into splenic pulp, and then slow infusion of 10 to 20 ml of sterile, water-soluble iodinated contrast medium is performed.+ Three to four lateral radiographs, exposed 7 to 10 seconds after injection, should be obtained at 1- to 2-second intervals. This is possible with any radiographic equipment if a “tunnel” is constructed. The patient is placed on a Plexiglas board, which is elevated off the table high enough to allow easy passage of x-ray cassettes. Cassettes can be rapidly pushed through the “tunnel” using an object as simple as a broomstick. To ensure correct cassette placement under the abdomen, markers should be placed at appropriate locations on the broomstick before the initiation of the procedure. On a normal-appearing angiogram, mesenteric or splenic veins normally drain into the portal vein, the portal vein branches with the liver (Figure 2-38), and hepatic venous blood flows into the caudal vena cava. Radiographic Signs of Liver Disease Hepatomegaly. Radiographic signs of hepatomegaly include the following: 1. Stomach displacement is usually more evident in the body and pyloric regions. The stomach is displaced caudally and dorsally, causing the stomach axis to be more horizontal. 2. With symmetric, diffuse liver enlargement, liver borders are often rounded and extend well beyond the ribs. Because the liver is larger on FIGURE 2-38 Normal hepatic portal venogram. Contrast medium was injected into a mesenteric vein, which drains into the portal vein. Note the extensive branching of the portal vein in the liver. (Courtesy Dr. Kathy Spaulding, North Carolina State University Veterinary Teaching Hospital, Raleigh, NC.) Figure 2-39 A, Lateral radiograph of a cat with an enlarged liver. On the survey film there is increased soft tissue opacity in the cranial abdomen. Liver cannot be delineated. B, Same cat as in A. Contrast medium in the stomach shows caudodorsal gastric displacement by an enlarged liver. the right side, there is often axial displacement of the stomach on the VD view. 3. Asymmetric liver enlargement is usually due to liver masses. Concurrent displacement of the stomach, kidneys, spleen, and colon is directly influenced by the location of the mass. The liver borders are often spherical or nodular. Positive or negative contrast in the stomach can aid in evaluating liver size (Figure 2-39). Small Liver. This is commonly due to chronic liver disease and cirrhosis, portal vein anomalies, or physical displacement of the liver into the chest (diaphragmatic hernia). On the radiographic study, the stomach axis becomes more vertical or may be directed cranially, liver borders may be sharply defined or nodular, and free abdominal fluid often occurs secondary to chronic cirrhosis. With diaphragmatic hernia, soft tissue opacity is present in the thorax and the diaphragmatic outline is not well defined. Portal Vein Anomalies—Angiography. On angiography a patent ductus venosus or other portosystemic shunt may be identified (Figures 2-40 and 2-41). Portal circulation in portocaval or portosystemic shunts is decreased or absent. Gallbladder Diseases. These are difficult to diagnose on a survey radiograph. Changes in size and shape are not usually perceived. Only changes in opacity can be consistently detected radiographically. Mineral opacity in the area of the gallbladder or biliary system is usually due to calculus formation, which is a rare occurrence in the dog and cat. Gas in the area of the gallbladder also is rare and is most likely associated with emphysematous cholecystitis. Pancreas Normal Anatomy The normal pancreas is not visible radiographically. The pancreas is located medial to the descending duodenum and caudal to the pylorus Figure 2-40 Venous phase of a cranial mesenteric arterial injection of contrast medium. The portal vein (PV) bypasses the liver through a patent ductus venosus (PDV) to empty into the caudal vena cava (CVC). Normal portal circulation through the liver is not seen. and greater curvature of the stomach. The transverse colon lies caudal to the area of the pancreas. Any significant pancreatic enlargement may be appreciated in these areas. Figure 2-41 Percutaneous splenic portography shows numerous tortuous splenic veins draining into both the portal vein (pv) and the caudal vena cava (vc). There is some portal blood flow through the liver (arrow). S, Spleen. Radiographic Diagnosis of Pancreatic Disease Unfortunately, more than 50% of dogs with pancreatic disease have no detectable radiographic abnormalities. Any radiographic changes seen in pancreatic disease are nonspecific, with similar changes detected in acute or chronic pancreatitis and pancreatic neoplasia. The ill- defined increased opacity in the pancreatic region can be related to edema, necrosis, fibrosis, abscessation, or tumor spread. Changes include the following: 1. Loss of detail and increased soft tissue opacity in the area of the pancreas. This loss of detail may be subtle, and diagnosis relies heavily on judgment and experience in evaluating radiographs. Close comparison of other areas of the abdomen, such as the spleen and fundic border of the stomach, with the pancreatic area may facilitate the diagnosis (Figure 242). 2. On the VD view the pylorus may be displaced toward midline and the duodenum displaced to the right abdominal wall. This causes an increase in the size or width of the cranial duodenal flexure. A barium study may be necessary to confirm this finding. 3. The transverse colon may be displaced cau- dally away from the greater curvature of the stomach on both the lateral and the VD views. Figure 2-42 A, Lateral radiograph of a dog with clinical signs of pancreatitis. There is loss of abdominal visceral detail in the cranial ventral abdomen. A hazy, streaky fluid opacity is apparent in this region. C, Transverse colon. B, Ventrodorsal radiograph of a dog with clinical signs of pancreatitis. There is an increased soft tissue opacity in the area of the pancreas (arrowheads). 4. The duodenum may be displaced dorsally or ventrally on the lateral view. 5. The duodenum may have persistent gas dilation or may appear “fixed”in position on serial radiographic studies. 6. A barium study may show the duodenum to have a thickened wall, corrugation or spasm, stricture formation, ulceration, and/or atonicity (Figure 2-43). These changes are nonspecific and cannot be considered as definitive evidence of pancreatic disease.