Corneal Disease
Corneal Ulcers
Most chronic cases of corneal ulceration are in actuality cases of refractory or recurrent ulceration due to some other form of chronic ophthalmic disease, such as KCS, corneal degeneration, or chronic intraocular disease that disrupts the integrity of the cornea.
Please see other sections of this chapter for a discussion of the diagnosis and treatment of these other conditions. Treatment for these secondary corneal ulcers should always occur concurrently to treatment for the underlying condition, ifpossible, or at least in recognition of the impact the underlying etiology has on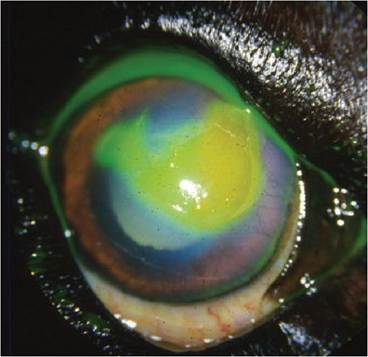
Figure 4.15 Refractory, or indolent ulcer, in a dog. Not the loose lip of epithelium and the fluorescein that has seeped underneath this non-adherent tissue.
the wound healing potential of the cornea. Therapy for a corneal ulcer should aim to 1) sterilize the wound bed (i.e., treat an infection if present, prevent an infection if not), 2) address the concurrent anterior uveitis present, 3) stop or prevent further breakdown of corneal collagen, 4) provide analgesia, and 5) provide structural stabilization if the ulcer is deep or perforating.
Many cases of refractory or indolent ulcers develop due to a defect or degeneration in corneal epithelial cell adhesion and/or the anterior stroma and are quite common in older dogs (Bentley and Murphy 2004; Gosling, Labelle, and Breaux 2013; Nevile et al. 2015; Sansom and Blunden 2010; da Silva et al. 2011; Michau et al. 2003) (Figure 4.15). In addition to the goals of therapy outlined above, these cases require mechanical debridement to remove any abnormal tissue from the ocular surface and to encourage reattachment of the overlying epithelium. Several forms of debridement are possible. Simple debridement of any non-adherent or “lipped” epithelial tissue can and should be performed with a dry, sterile, cotton-tipped applicator.
After application of a topical anesthetic agent, such as proparacaine or tetracaine, the cotton-tipped
Figure 4.16 Diamond burr debridement of a refractory superficial corneal ulcer in a dog.
applicator should be used in a circular motion to peel away the loose epithelium from the margins of the wound. If this is insufficient to encourage re-epithelialization, more aggressive debridement with either a diamond burr or a small gauge needle (grid keratotomy or multiple punctate keratot- omy) may be necessary. A diamond burr will polish the exposed stroma and create an improved area for epithelial attachment (da Silva et al. 2011) (Figure 4.16). Keratotomies disrupt the exposed stroma or any membranes that have formed atop it to allow epithelial adhesion. None of these procedures should be performed on corneal ulcers that are not superficial due the risk of progression of the wound and perforation. Diamond burr debridement is also useful to remove superficial mineral deposits from the exposed stroma in cases of corneal degeneration or band keratopathy (Nevile et al. 2015; Sansom and Blunden 2010).
The addition of a bandage contact lens may improve the comfort of a patient with a superficial ulcer, especially if some adnexal irritation, such as trichiasis, entropion, or an adjacent eyelid mass, is exacerbating the problem, and facilitate reepithelialization (Gosling, Labelle, and Breaux 2013).
Keratitis
Corneal inflammation regardless of etiology has a very similar set of clinical signs, typically corneal vascularization, pigmentation, and occasional cellular infiltrate. Most of the immune-mediated forms of keratitis, including chronic superficial keratitis, also known as pannus, eosinophilic keratitis, pigmentary keratitis, and KCS are chronic conditions that require longstanding therapy to slow or prevent progression of the corneal lesions and maintenance of corneal clarity (Andrew 2008) (Figure 4.17).
The mainstay therapy for immune-mediated keratitis is topical antiinflammatory medication, either an immunomodulator such as cyclosporine or tacrolimus, or a steroidal or non-steroidal anti-inflammatory. Often steroids and either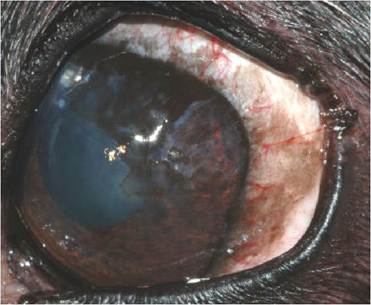
Figure 4.17 Chronic superficial keratitis, or pannus, in a Greyhound.
cyclosporine or tacrolimus are used in concert to control the inflammation through different mechanisms. This often achieves better control than sequential therapy. Steroids are generally more potent and will work faster to control clinical signs, while the immunomodulators have a slower onset of action but are safer for long-term control and generally have fewer untoward side effects. Limiting exposure to UV radiation may decrease the severity or slow the progression of some forms of keratitis, particularly chronic superficial keratitis in German Shepherd Dogs and Greyhounds (Figure 4.18).
A deeper form of keratitis affecting the corneal endothelium presents with corneal edema and sometimes keratitic precipitates on the endothelial surface (Andrew 2008). This condition often becomes chronic since damage to the corneal endothelium is usually irreversible due to the limited regenerative potential of the endothelium. Immunomodulators do not penetrate the cornea well, so topical steroids are generally the preferred treatment. Topical hyperosmotic agents, such as 5% sodium chloride solution or ointment, may facilitate removal of excess fluid in the corneal stroma and are particularly helpful if fluid has coalesced into bullae within the anterior stroma or the epithelium. Bullae rupture will result in corneal ulceration, which is painful and necessitates the discontinuation of topical steroid therapy. Corneal ulcers that accompany endotheliitis or endothelial degeneration are often refractory or slow to healing.

Figure 4.18 Goggles may limit exposure to UV radiation.
They may also be helpful for protecting the eyes of visually impaired animals that may be injured or at risk.Corneal Degenerations
Corneal degenerations are secondary pathologic changes. They may occur in the epithelium and anterior stroma or in the endothelium. The specific cell type affected determines the form and clinical signs that develop (Samuleson 2013). Once the process of corneal degeneration begins, it is generally not curable, but may be manageable. Degenerations may be unilateral or bilateral, but are often asymmetric when bilateral. Epithelial disruption with subsequent ulceration and vascularization is common.
In the superficial form, lipids, cholesterol, calcium, or a combination thereof are deposited in the anterior stroma secondary to inflammation, vascularization, and tissue weakness. The age-related form of this condition is common in aged dogs and can lead to chronic pain and recurrent and refractory corneal ulcerations (Figure 4.19). The form that occurs secondary to chronic ocular inflammation resembles band keratopathy

Figure 4.19 Corneal degeneration in an aged dog. Some of the corneal stroma and deposits have slough leaving a deep stromal corneal ulcer. Note the white, crystalline opacities surrounding the defect and the corneal vascularization.
wherein mineral deposits accumulate in the subepithelial space or in the anterior stroma and prevent proper adhesion of the corneal epithelium. The gritty and irregular deposits may cause the epithelium to erode. The rough feeling of the underlying deposits is terribly uncomfortable to the patient as the eyelids rub over the surface with every blink. Routine medical therapy for an ulcer should be begun along with the addition of a chelating agent, usually some form of EDTA, to try to remove some of the deposits or at least decrease their accumulation. The ulcers that develop are often refractory to healing and repeated manual debridement is often necessary to facilitate epithelial adhesion.
Cotton tipped applicator debridement followed by diamond burr keratectomy can be most beneficial to the healing process (Gosling, Labelle, and Breaux 2013; Nevile et al. 2015; Sansom and Blunden 2010; da Silva et al. 2011). However, if epithelialization and adhesion is not achieved after several attempts, lamellar keratectomy may be necessary to facilitate healing and improve comfort. However, it should not be performed repeatedly because the stroma may not regenerate to full thickness in aged and diseased corneas.The corneal degenerations secondary to endothelial disease present with corneal edema, usually starting from the temporal aspect of the cornea. They occur most frequently in the Boston Terrier, Dachshund, and Chihuahua breeds (Figure 4.20, Figure 4.21, and Figure 4.22). The disease progresses until complete edema, occasionally complicated with recurrent corneal bullae formation, and visual impairment to blindness occurs. Medical therapy with topical osmotic agents (5% NaCl) is helpful but does not clear the cornea completely and will become less effective at managing corneal bullae as the disease progresses. Surgical treatment is more definitive, but not curative. It may include thermokeratoplasty wherein the superficial corneal stroma is cauterized with thermal energy to coagulate the corneal collagen and decrease potential space between the lamellae for fluid accumulation,

Figure 4.20 Corneal endothelial degeneration in a Chihuahua. In this breed, the condition is inherited. Note the mid-range pupil. Pupil size and responsiveness may help differentiate endothelial disease from glaucoma, which is one of the differentials for corneal edema.

Figure 4.21 Corneal endothelial degeneration in a Bassett Hound. Note the corneal vascularization present that was the response to a long-standing superficial corneal ulcer. Microbullae form within the stroma and epithelium when significant corneal edema is present which may rupture resulting in ulceration that may be slow or refractory to healing.
superficial keratectomy with Gunderson conjunctival pedicle grafts or full-thickness keratoplasty (Michau et al. 2003)
(Figure 4.23). Keratoplasties are essentially corneal transplants which replace the disease endothelium with viable endothelial cells from a healthy donor eye. Endothelial degeneration predisposes the patient to refractory and recurrent ulcerations as bullae form from the accumulation of edema fluid in the corneal stroma then rupture through the epithelium.