Ocular Surface Disorders
The Preocular Tear Film
The preocular tear film consists of lipid, aqueous, and mucin components (Samuleson 2013). The most superficial layer is a lipid secreted by the meibomian glands that acts to slow or prevent evaporation of the aqueous portion of the tear film.
The lipid portion promotes a stable, optical smooth layer of tears over the cornea. The aqueous component of tears is secreted by lacrimal glands of the orbit and nictitating membrane and accounts for most of the total tear volume. It consists of water, electrolytes, glucose, urea, surface-active polymers, glycoproteins, and tear proteins, including immunoglobulins and other factors involved in immune surveillance and antimicrobial efforts. The final layer of tears is mucin, which is produced by the goblet cells of the conjunctiva. This mucin keep the aqueous tear fluid attached to the corneal epithelium and fills in any irregularities of the corneal surface. A deficiency of any of these three components will result in clinical signs of dry eye.Keratoconjunctivitis sicca
Keratoconjunctivitis sicca (KCS) is unfortunately an all too common ocular disease in the dog and it is generally a lifelong condition requiring chronic and diligent therapy and monitoring (Figure 4.4). The incidence of KCS in dogs is great with roughly 1% of the general population affected (Giuliano 2013). Quantitative or “classic” KCS is characterized by a deficiency of the aqueous tear fluid which results in desiccation and inflammation of the conjunctiva and cornea. Ocular pain and progressive corneal disease, with subsequent reduction in vision, occur.
The reduction or absence of lacrimal secretions may result from a single disease process or a combination of conditions affecting the lacrimal glands. The most common etiology is an immune-mediated inflammation of the lacrimal glands which results in dysfunction and impaired production of the aqueous fraction of tears (Giuliano 2013; Kaswan, Martin, and Dawe 1985; Hendrix et al.
2011; Barachetti et al. 2015). A variety of other etiologies have been identified, however, including neurogenic causes, toxic changes within the glands due to drug or chemical exposure, and metabolic
Figure 4.4 Keratoconjunctivitis sicca in a West Highland White Terrier. Note the discoloration of the facial fur. This is common in many types of tear and ocular surface disorders. Also note the mucoid discharge present.
alterations (Giuliano 2013). Several breeds are disproportionately affected by acquired KCS, thus suggesting a genetic predisposition (Table 4.1). The diagnosis of KCS is made on the basis of typical clinical signs and decreased Schirmer tear test (STT) results. In the clinical setting, STT I readings in dogs are generally interpreted as follows: ≥ 15 mm/min = normal production; 11-14 mm/min = early or subclinical KCS; 6-10 mm/min = moderate or mild KCS; and ≤ 5 mm/min = severe KCS (Table 4.2). Acute onset KCS is occasionally seen, wherein an eye becomes acutely and severely painful and usually exhibits axial corneal ulceration (Figure 4.5). If not addressed promptly, these cases may develop suppurative inflammation which exacerbates the progressive nature of the corneal disease with stromal malacia, descemetocele formation, and iris prolapse. Fortunately, in most cases, the onset of KCS is more gradual, with increasing severity over a period of several weeks (Giuliano 2013). These eyes initially present for redness and appear inflamed, with intermittent mucoid or mucopurulent discharge (Figure 4.6). As the severity and chronicity of the KCS increases, the ocular surface becomes lackluster, the conjunctiva becomes progressively more hyperemic, and persistent tenacious mucopurulent ocular discharge develops. The keratitis, which progresses if left untreated, is usually characterized by extensive corneal vascularization and pigmentation (Figure 4.7 and Figure 4.8).
This corneal opacification can lead to vision deficits or loss.Treatment of quantitative dry eye has two primary goals: 1) stimulate the patient to produce organic tears and 2) supplement the patient with topical lubricants (artificial tear preparations). Additionally, depending upon the presence and severity of other clinical signs, topical anti-inflammatory medications, usually corticosteroids, may be necessary to control initial or intermittent surface inflammation. Topical antibiotics maybe necessary to control secondary bacterial conjunctivitis. Dry eye is the foremost reason for bacterial conjunctivitis to develop. It is rare for primary bacterial conjunctivitis to occur in small animals without an antecedent condition. The use of a mucolytic agent may facilitate administration of other topical medications and may make cleaning and removal of the mucoid discharge easier.
Since most cases of KCS are immune- mediated in origin, the most commonly employed tear stimulating drugs are the immunomodulating agents, cyclosporine (0.2-2.0%) and tacrolimus (0.02-1.0%), both of which work by targeting T-helper cells and decreasing the inflammatory response
Table 4.1 Breed predisposition to chronic ocular disease.
| KCS | Zonular Instability | Primary Glaucoma |
| Cavalier King Charles Spaniel | Jack/Parsons Russell Terrier | American and English Cocker Spaniels |
| English Bulldog | Fox Terriers | Bassett Hound |
| Lhasa Apso | Sealyham Terrier | Chow Chow |
| Shih Tzu | Miniature Bull Terrier | Shar-Pei |
| Pug | Tibetan Terrier | Boston Terrier |
| West Highland White Terrier | Shar-Pei | Norwegian Elkhound |
| Bloodhound | Border Collie | Siberian Husky |
| American Cocker Spaniel | German Shepherd | Beagle |
| Pekingese | Lancashire Heelers | Miniature and Toy Poodles |
| Boston Terrier | Italian Greyhound | Samoyed |
| Miniature Schnauzer | Chinese Crested Dog | Cairn Terrier |
| Samoyed | Shih Tzu Australian Cattle Dog Akita Jack Russell Terrier Bichon Frise Fox Terriers Border Collie Lhasa Apso Pekingese Bouvier des Flandres Brittany Spaniel Dalmatian English and Welsh Springer Spaniels Italian Greyhound Dachshund Chihuahua |
within the lacrimal glands (Giuliano 2013; Kaswan, Martin, and Dawe 1985; Hendrix et al.
2011; Barachetti et al. 2015). They also have a separate lacrimogenic effect separate from their anti-inflammatory effects that is not as yet well understood. The choice of drug to initiate therapy with is generally a matter of clinician preference. If, however, therapy with cyclosporine fails to resolve clinical signs and return STT values to the normal range, it is worth trying tacrolimus, as there is a subset of animals that does not respond to cyclosporine but will respond to this alternative. With the exception of the 0.2% commercially available ointment preparation of cyclosporine, both drugs must be compounded for topical use. Recently, biodegradable slow release cyclosporine episcleral implants have become available (Barachetti et al. 2015). These are helpful both in refractory cases and those that have an underwhelming response to therapy due to poor compliance. A small percentage of patients develop neurogenicTable 4.2 Interpretation of STT I values and treatment recommendations.
| STT I value | Diagnosis | Treatment options |
| ≥15 mm/minute | Normal | |
| 11-14 mm/minute | Early or subclinical KCS | Cyclosporine 0.2-1.0% q12-24 h or Tacrolimus 0.02% q12-24 h and Artificial Tears q8-12 h |
| 6-10 mm/minute | Mild to moderate KCS | Cyclosporine 1.0-2.0% q12h or Tacrolimus 0.02-.03% q12h and Artificial Tears q4-6 h +/- Dexamethasone 0.01% q8-24 h +/- Acetycysteine 5.0% q8-12 h |
| ≤5 mm/minute | Severe KCS | Cyclosporine 1.0-2.0% q8-12 h and/or Tacrolimus 0.03%-1.0% q8-12 h and Artificial Tears q2-6 h +/- Dexamethasone 0.01% q8-24 h +/- Acetycysteine 5.0% q6-12 h +/- Pilocarpine (if neurologic origin is suspected) +/- Episcleral CsA implants +/- Parotid duct transposition +/- Buccal mucosal graft |

Figure 4.5 A deep stromal corneal ulcer that has resulted from dry eye.
The axial location is typical for ulcers that develop from exposure and KCS.
Figure 4.6 Mild to moderate KCS with early corneal changes and mucoid discharge.
KCS, wherein the innervation to the lacrimal glands is disrupted (Giuliano 2013). If the KCS has developed due to a neurogenic insult, the addition of pilocarpine may be helpful to supplement the absent neurotransmitter and stimulate aqueous tear production from the glands. It may be given orally (1-2 drops of the 2% topical preparation per 10 kg body weight PO in the food q12h, increasing in one drop intervals if no improvement is noted until clinical signs of hypersalivation, vomiting, or diarrhea occur; or a dilute preparation (0.1%) given topically q12h).
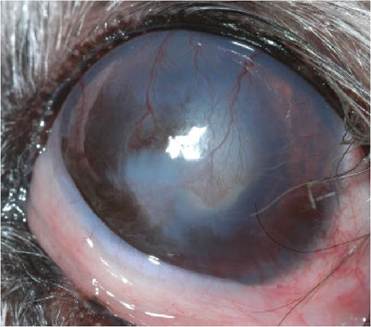
Figure 4.7 Keratitis in a Shih Tzu secondary to moderate dry eye. Note the corneal vascularization and superficial pigmentation.

Figure 4.8 Severe KCS with extensive corneal pigmentation and fibrosis in a Chinese Crested Dog.
If the KCS fails to respond to medical therapy, surgical options exist. Parotid duct transposition wherein the salivary duct is repositioned into the ventral conjunctival fornix will supply the ocular surface with lubrication, however, it may be associated with undesirable consequences such as excessive “epiphora,” facial dermatitis and mineral accumulation on the cornea or eyelids (Giuliano 2013). It can dramatically improve patient comfort, however. Recently, the use of buccal mucosal grafts has been advocated to improve patient comfort. In this procedure, a free graft of mucosa from the oral cavity is sutured into the conjunctival fornix. It is believed that the transplantation of glandular tissue from the mouth to the eye provides something in the way of additional lubrication, although the STT values remain unchanged.
Some report a dramatic improvement in patient comfort.Qualitative Tear Deficiencies (Qualitative Dry Eye)
If either the lipid produced by eyelid meibomian glands or the mucin produced by conjunctival goblet cells components of the tear film are absent or decreased in quantity, clinical signs of KCS will develop even if STT measurements are within the normal range (Giuliano 2013). This is known as qualitative dry eye. This condition most often occurs secondary to disruption or inflammation of the target tissues that produce either the mucin or lipid fractions of the tears. Chronic conjunctivitis or chronic blepharitis or meibomianitis will result in a reduction of mucin and lipid, respectively. When the tear quality is impaired, aqueous tears will evaporate too quickly and will not be able to stay distributed evenly and adequately across the ocular surface, essentially creating a functional dry eye. The diagnosis is confirmed with either of the vital dyes, rose Bengal or Lissamine green, which localize to areas of the cornea where the mucin fraction is insufficient. Additionally, the tear film break-up time will help determine if the tear film is unstable and evaporating too quickly (Giuliano 2013). When fluorescein stain is applied to the ocular surface in high concentrations, it will saturate the tear film. After blinking to evenly distribute the dye, the patient's eyelids are held open manually (to prevent blinking) and the time is counted in seconds until the homogenous green color on the ocular surface begins to develop dark splotches, indicating areas where the tear film has “broken up,” or become unstable and started to evaporate or dissipate. If this break up occurs before 10 seconds of elapsed time, the tear film is described as unstable and of poor quality.
Treatment is aimed at improving the quality and amount of mucin and/or lipid and supplementing with artificial tears, essentially the same approach used in quantitative dry eye. Medical treatment with cyclosporine or tacrolimus will in most cases normalize or improve tear lipids and mucin and result in an improvement of clinical signs. Artificial tears will bridge the gap while tear quality is on the mend. Compounding the immunomodulators in an oily base will help with clinical signs. The addition of essential fatty acids to the diet is thought by some to be helpful in improving tear quality.
Conjunctivitis
Conjunctivitis can be a particularly frustrating condition when it becomes chronic. Conjunctival hyperemia, chemosis and discharge ranging in character from clear and serous to mucoid or mucopurulent are the most common clinical signs seen (Figures 4.9 and 4.10). With chronicity, the patient may develop conjunctival follicles which are semitransparent, bubble-like aggregates of lymphoid tissue, the result of chronic antigenic stimulation (Figure 4.11). The most common etiologies for chronic conjunctivitis in dogs are tear film abnormalities (see earlier discussion) and allergies. A thorough ocular examination with evaluation of the quantity and quality of the tear film is necessary to determine the etiology. Allergic conjunctivitis is a rule-out

Figure 4.9 Allergic conjunctivitis in a mixed breed dog. Note the conjunctival hyperemia and chemosis.
diagnosis that is made if the tear film is sufficient and there are no other signs or indications of ocular or systemic disease (Pena and Leiva 2008; Bistner 1994; Peiffer 1980; Lourenqo- Martins et al. 2011). Treatment of allergic conjunctivitis is best achieved with identification and removal of the offending antigen. If this is not possible, symptomatic treatment with the least amount of drug necessary to control clinical signs will be necessary. Topical corticosteroids, cyclosporine, or antihistamines may be considered (Lourenqo-Martins et al. 2011). It may be challenging to find the right “cocktail” of empiric medications for some individual patients. Topical lubricants (artificial tears) may be helpful for short-term comfort.
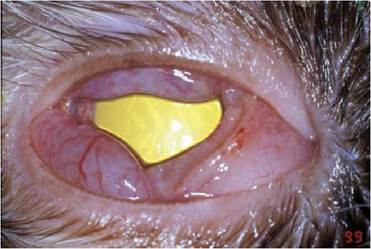
Figure 4.10 Herpetic keratitis is a cat with profound conjunctival chemosis and hyperemia.

Figure 4.11 Chronic conjunctivitis in this Labrador Retriever has resulted in follicle formation.
Conjunctivitis in cats is most often initiated by an infectious agent. Feline herpesvirus-1 (FHV-I) is the most common infectious agent responsible for conjunctivitis in cats (Peiffer 1980; Malik et al. 2009). Chlamydophila felis and mycoplasmal organisms are also implicated, but less often. When cats develop chronic conjunctivitis, it may be difficult to implicate FHV-1 because the classic respiratory signs associated with primary infections are usually absent. However, since the virus establishes itself and develops latency, it may contribute to active conjunctivitis and keratitis at any time, particularly during periods of stress. In some cats, the immune system will mount a response to the presence of viral antigen and cause ocular surface inflammation without the cytolytic contributions of viral replication. Additionally, FHV-1 may initiate the development of KCS in cats, so clinical chronic conjunctivitis in cats may be due to a multitude of related problems (Giuliano 2013). The establishment of causation is difficult to prove considering most cats have been exposed to FHV-1 and many become carriers and can shed virus without clinical signs. The presence of the virus detected via indirect fluorescent antibody staining or PCR will not necessarily be diagnostic (Sjodahl-Essen et al. 2008). Neither will conjunctival cytology be helpful in diagnosing FHV-1, however, it may be helpful for diagnosing chlamydophilal (cytoplasmic inclusions), mycoplasmal (organisms seen), or eosinophilic conjunctivitis (eosinophils, mast cells), all of which may occur as concurrent conditions or co-infections with FHV-1. Treatment can be very frustrating to both cats and their owners. Generally, if an infectious agent is suspected, a course of antimicrobial agents is recommended. If chlamydophilal or mycoplasmal organisms are present or suspected, a course of topical (oxytetracycline, chloramphenicol or erythromycin q6h for 2-3 weeks) and/or systemic tetracyclines or macrolides (doxycycline 5mg∕kg PO q12h or azithromycin 5mg∕kg PO q24h) may be helpful, but may not be effective at eliminating a carrier state. Herpetic keratoconjunctivitis is somewhat more difficult to control. The minimal amount of medical intervention should be employed. Often, particularly in mild cases, topical lubricants may be sufficient to help minimize discomfort until the flare-up subsides on its own. A short course of systemic non-steroidal therapy (meloxicam 0.1 mg/kg PO q24h or robenacoxib 1 mg/kg PO for 3 days) may be helpful initially as well. In severe or refractory cases, or those in which there is also corneal involvement, anti-viral therapy may be indicated. Antiviral therapy with topical agents will limit the extent of systemic side effects, but may be challenging due to the fact that effective drugs are not commercially available and must be produced by a compounding pharmacy (cidofo- vir 0.5% q12h or idoxuridine 0.1% q4h) (Figure 4.12). If topical agents aren't successful in decreasing the severity of clinical signs or if there are systemic signs or dermatologic involvement, systemic antiviral may be used (famciclovir 10-90 mg/kg q24h) (Sjodahl- Essen et al. 2008). Antivirals are usually given until clinical signs resolve and then are discontinued, rather than tapered in frequency. A few cats require chronic administration, rather than interval therapy during an active bout, and these cats should be monitored regularly with complete blood counts and serum chemistries to determine if any bone marrow or renal toxicity is developing.
Cats will also develop non-infectious conjunctivitis. Eosinophilic conjunctivitis, with or without keratitis, typically presents with the classic signs of conjunctivitis (hyperemia, chemoisis, and discharge) but may also exhibit raised, irregular, or roughened lesions resembling granulation tissue in the bulbar, palpebral or nictitans conjunctiva or on the cornea (Allgower, Schaffer, and Stockhaus 2001) (Figure 4.13). Cytology of these lesions reveals the presence of eosinophils and mast cells. Tear production may be decreased in these cats secondary to obstruction of lacrimal ductules by the

Figure 4.12 Severe herpetic Dlepharokeratoconjunctivitis in an eldery feline.

Figure 4.13 Eosinophilic keratoconjunctivitis conjunctivitis in a cat.

Figure 4.14 Lipogranulomatous conjunctivitis in a cat.
conjunctival swelling. Treatment is aimed at decreasing the inflammatory response and usually requires an extended course of treatment with a very slow taper of frequency. Lipogranulomatous conjunctivitis is an unusual form of conjunctivitis occurring in older cats as non-ulcerated white nodules in the palpebral conjunctiva (Kerlin and Dubielzig 1997) (Figure 4.14). Histopathology of the lesions describes macrophages and multinucleated giant cells filled with lipid. Surgical excision of the nodules may be curative, otherwise chronic therapy with corticosteroids is necessary to minimize the inflammation and improve patient comfort.