Diagnostic approach to patients with suspected liver disease
A definitive diagnosis of a disease of the liver, biliary tract, or portal vein usually requires a multi-step approach. The clinical symptoms, which may occur in patients with these diseases, are often nonspecific.
A history of symptoms potentially related to hepatic diseases is followed by physical examination, laboratory evaluation, ultrasonography, cytology, histological evaluation of liver biopsies, scintigraphy, or liver function testing.7.3.1 Prevalence of liver disease
The recognition of hepatic disorders on the basis of history and physical examination is often difficult, because the symptoms are usually nonspecific.6-8 This nonspecific presentation of patients with liver disease makes accurate statements about prevalence difficult. Liver and biliary tract diseases have been reported to have an incidence of approximately 1-2% of all clinical cases presented to referral practice.9-12 However, well-documented figures for a first line clinical population are not available. Also, there are breed-specific diseases that need to be taken into account separately. We have investigated the prevalence of inherited portosystemic shunts in several breeds such as the Irish Wolfhound and the Cairn Terrier in the Netherlands and found a prevalence of 4% and 2%, respectively.9,13,14 In general, the prevalence of portosystemic shunts in commonly affected breeds (around 30 breeds) has been estimated to be around 1-4% of puppies born. Hepatitis is another example of a liver disease, which may be hereditary or be affected by inherited risk factors. The Bedlington Terrier used to have a very high prevalence of copper-associated hepatitis (20-50% of the population) until a mutation in the Murr1 gene was discovered and subclinically diseased animals and carriers could be identified with a DNA test.
Copper- associated hepatitis also frequently occurs in Labrador Retrievers (estimated prevalence around 10-15%) and Doberman Pinschers (estimated prevalence around 5%) (see 7.5.1.4). Therefore, it is important to keep breed predispositions in mind when a list of differential diagnoses is being constructed for a specific patient.7.3.2 Symptoms associated with liver diseases6
Because of the lack of specific clinical signs for liver disease, a few factors need to be considered that may help with the interpretation of clinical findings in patients with suspected liver disease. The liver plays an essential role in many metabolic processes. Disturbances in liver function may affect the function of other organ systems, which may point to a disease process of that organ rather than to the liver. Examples of this are hepatic encephalopathy, which may point to a central nervous system disease, or polydipsia, which may point to an endocrine or renal disease. The liver is also often secondarily involved in diseases of other organ systems, so that the same symptoms and abnormal laboratory findings can occur as with primary liver disease. One example is vomiting, which is a frequent symptom in patients with primary liver disease, but at the same time is also a clinical sign in patients with primary GI disorders that could also result in secondary (reactive) hepatitis. In both scenarios, the clinical symptoms are identical and blood biochemical tests would indicate the presence of liver disease, although the primary disease process may not be hepatic in origin. Another example is polyuria and polydipsia, symptoms that are frequently observed in many patients with chronic primary liver disease, but also in patients with several endocrine and paraneoplastic diseases in which the liver is secondarily involved (e. g., Cushing’s disease, diabetes mellitus, malignant lymphoma). In all these diseases, the plasma hepatic enzyme activities and serum bile acid concentrations are often increased.
The following symptoms can be observed in different combinations in a variety of liver diseases: apathy, listlessness, reduced appetite, vomiting, weight loss, polydipsia, diarrhea, reduced endurance, ascites, neurological signs, icterus, acholic feces, increased bleeding tendency, painful micturition, frequent micturition, or abdominal pain. Apathy or listlessness is very frequent, as are reduced appetite or vomiting, which may be an indication of nausea. Weight loss occurs frequently in patients with chronic disease. Polydipsia has been reported with a prevalence of 50-60% in patients with chronic liver disease, including cholestatic diseases and portosystemic shunts. Diarrhea occurs infrequently in dogs and cats with liver disease and is usually not a major problem in patients with primary liver disease. As such, dogs and cats presenting only with diarrhea usually do not have primary liver disease as the underlying cause. Ascites occurs only infrequently and only in patients with an extreme loss of hepatic function. Neurological signs (i.e., ataxia and compulsive walking) occur frequently, especially in patients with portosystemic shunting. Such signs of hepatoencephalopathy usually wax and wane. Icterus is infrequent and more than 90% of dogs with liver disease have a normal serum bilirubin concentration. However, cats with hepatopathies have jaundice more frequently. Abnormally lightly colored (i.e., acholic) feces also occur very infrequently and are only seen in patients with bile duct obstruction. Also, an increased bleeding tendency is very infrequent. However, subclinical abnormalities of the coagulation cascade are more frequent. Painful, frequent micturition is also observed infrequently and is only seen in dogs with portosystemic shunts that cannot metabolize uric acid and ammonia, and in turn develop ammonium urate urolithiasis. Abdominal pain is very rare, but is sometimes seen in patients with cholecystitis.
It is important to note that the entire spectrum of symptoms may be observed in different combinations in most hepatobiliary diseases, but that it is usually not possible to relate the symptoms to a specific liver disease.
Any combination of the above symptoms should lead to evaluation of the patient for possible liver and /or biliary disease.7.3.3 Physical examination6-8
The most relevant parts of the physical examination are the evaluation of the mucous membranes and sclera, and an abdominal palpation. While mucous membranes are normal in most patients with liver disease, abnormalities may include jaundice, pallor, or spontaneous bleeding. Reduced erythrocyte survival time (increased hemolysis) is very common in patients with hepatobiliary disease. In combination with reduced erythropoietic activity as a consequence of chronic disease in general, the finding of a slight anemia and somewhat pale mucous membranes is very common in patients with chronic hepatobiliary disease. When the mucous membranes are very pale (Htc usually < 15-20%), the underlying cause of the disease is usually hemolytic anemia with secondary hypoxic liver damage. In such cases, a careful search for an underlying cause of the hemolysis is indicated and further evaluation of the liver is not necessary. However, in patients with icterus and moderately pale mucous membranes (Htc > 20%), the primary cause is nearly always hepatic disease and further diagnostic tests should focus on the liver and the biliary system.
Hepatomegaly may be palpable upon abdominal examination, depending on the degree of the enlargement, the depth of the thorax, and the concavity of the diaphragm. Hepatomegaly is uncommon in dogs with liver disease, which more often causes an abnormally small liver in this species. However, hepatomegaly does occur in patients with primary hepatic tumors and diseases with secondary hepatic involvement, such as venous congestion, fatty liver (i.e., secondary to diabetes mellitus), glycogen accumulation (i.e., secondary to hyperadrenocorti- cism), amyloidosis, lymphosarcoma, or metastatic tumors. In contrast to dogs, cats with hepatobiliary disease often have hepatomegaly. However, when hepatomegaly is present, examination of the circulation is indicated to exclude primary cardiac disease.
Abdominal palpation may also reveal splenomegaly in the case of portal hypertension, but this is also rather nonspecific and not always present in patients with portal hypertension. Ascites may be present and serve as an indication for chronic liver disease with portal hypertension and a reduced capacity to synthesize albumin. Of course, there are many other causes of ascites but an evaluation of serum hepatic enzyme activities, serum bile acids concentrations, and serum albumin concentration is indicated to prove or exclude hepatic involvement.
In most patients with a disease of the hepatobiliary system, the physical examination reveals only nonspecific findings; therefore, a basic laboratory investigation is usually necessary to prove or exclude hepatobiliary disease.
7.3.4 Diagnostic tests for liver disease
A detailed discussion of diagnostic tests for the diagnosis of hepatic disease can be found in chapter 1.4.3. The liver has many different metabolic functions and consists of hepatocytes, the biliary system, Kupffer cells, fat-storing stellate cells, and an arterial and venous blood supply. Although the liver is often considered a homogeneous organ and one tends to speak of hepatic function, there is no single test that adequately identifies hepatic disease or its underlying cause. There are, however, many different tests available by which the presence and nature of liver diseases can be evaluated.15 Thus, the best approach for diagnosing hepatobiliary diseases is to use screening tests (see 1.4.3) to evaluate hepatobiliary damage and function. If such screening tests indicate the presence of hepatobiliary disease, the diagnosis is made by further diagnostic modalities such as imaging (see 1.3), cytology (see 1.7), and /or histological examination of a liver biopsy (see 1.8). Once a diagnosis has been made, it may be helpful to evaluate specific hepatic functions in order to determine the stage of the disease, which may be important for establishing the prognosis or choosing the most appropriate therapy for a given patient.
It is important to note that some hepatobiliary diseases are characterized by subtle changes in serum enzyme activities, but are associated with severe functional disturbances, while others are associated with severe changes in the serum enzyme activities, yet are not associated with significant hepatic dysfunction. Because of the large reserve capacity of the liver, detection of global hepatic functional impairment by conventional means is not possible until there is at least a 55% loss of hepatic mass. Parameters on a biochemistry profile that are routinely used for assessment of hepatic function include serum and plasma concentrations of albumin, ammonia,16,17 urea nitrogen, bilirubin, bile acids,18-20 cholesterol, and glucose. These tests can be used to assess the hepatic capacity to synthesize proteins, detoxify protein degradation products, excrete organic anions and other substances, or maintain eugly- cemia.
The results of a laboratory evaluation reflect a single point in time in a spectrum of dynamic changes. If the test results are equivocal and the clinical signs are vague, sequential evaluation may be necessary to allow time for the disease to be fully expressed. If the liver is only secondarily involved (such is the case in nonspecific reactive hepatitis), the hepatic changes and concomitant blood test results may normalize within three to four weeks, which makes this a good time span to repeat measurements in the case of equivocal test results as primary hepatic diseases will usually become more apparent, whereas nonspecific changes usually disappear.
By using a combination of history, physical examination findings, and the results of screening and hepatobiliary-specific laboratory tests, the clinician should be able to classify the disorder as active or quiescent; characterize the pattern of hepatobiliary disease as primarily hepatocellular, primarily biliary, or mixed hepatobiliary; and estimate the degree of hepatobiliary dysfunction. It is also important to note that results from a serum biochemical profile do not identify the underlying disease process and it is nearly always necessary to collect liver biopsies to reach a definitive diagnosis. In the case of a vascular anomaly (such as inherited portosystemic shunts), specific biochemical tests and ultrasonography and /or scintigraphy are required to arrive at a definitive diagnosis.
7.3.5 Liver biopsy
7.3.5.1 General considerations
As mentioned previously, for many primary hepatobiliary diseases in cats and dogs, a hepatic biopsy is needed to establish a definitive diagnosis and determine a prognosis.1 In some cases, bile culture is also imperative. Biopsy is indicated 1) to determine the underlying cause of abnormal results of tests of hepatic function and pathology, especially if they persist for longer than one month; 2) to determine the cause of hepatomegaly; 3) to determine hepatic involvement in a systemic illness; 4) to stage a neoplastic disease of the liver; 5) to objectively assess response to therapy in patients with hepatobiliary disease; or 6) to evaluate the progression of a previously diagnosed disease that is not specifically treatable.
Several approaches for the collection of a liver biopsy are available and the choice is dictated by both patient and operator considerations.1,21,22 All cats and dogs undergoing hepatic biopsy should be fasted for at least 12 hours, regardless of the approach selected. In general, percutaneous needle core biopsy or aspiration (for cytological analysis) of a single cavitary or solid lesion that is highly likely to be a non-lymphoid cancer is avoided unless the owner is unwilling to permit surgery for complete resection. Fine-needle aspiration for cytological analysis is advisable if multiple nodules are noted or if the owner is opposed to treatment of a neoplastic disease even if only a single lesion can be identified. Metastatic cancer may have a similar ultrasonographic appearance to benign hyperplasia or regenerative nodules. Unfortunately, the overall agreement of findings of cytological and histopathological diagnosis was only 44% in one study when evaluating neoplastic lesions of the liver. In patients with an especially small and /or firm fibrotic liver, it can sometimes be difficult to obtain a biopsy specimen by use of a percutaneous needle and this method often results in the collection of small and fragmented specimens that are difficult to interpret. In such cases, a true- cut biopsy usually produces diagnostic samples. The gun device usually leads to sharp, unfragmented slices even in the case of a firm, fibrotic liver. Also, the speed of the device prevents the liver from floating away from the tip of the needle. There is a reported correlation of site, as was found in one study of human pa- tients.25 However, the collection of a liver biopsy should be delayed if there is clinical evidence of bleeding or marked abnormalities in the coagulation parameters. Because animals with complete extrahepatic bile duct obstruction (EBDO) may be vitamin K deficient, as manifested by a prolongation of both OSPT and APTT, treatment with vitamin K1 (5 mg subcutaneously once or twice a day) is indicated for one to two days before biopsy collection. Repeating the OSPT and APTT 24 hours after the administration of vitamin K1 should
demonstrate normal or near-normal results. However, in modern practice, EBDO is mostly an ultrasonographic diagnosis, and a liver biopsy is not required in most of these cases. Some animals with liver disease may have high serum concentrations ofproteins induced by vitamin K antagonism (PIVKA), which could suggest potential bleeding tendencies. If there has been a minimal improvement in the coagulation parameters after vitamin K1 administration, fresh frozen plasma should be administered before the collection of a biopsy. If bleeding is determined to be excessive during biopsy collection or after a biopsy has been collected and if bleeding cannot be controlled locally with direct pressure or application of pro-coagulatory substances, fresh whole blood should be given.
7.3.5.2 Biopsy techniques1'26'27
7.3.5.2.1 True-cut biopsy needle
True-cut biopsy needles have an inner needle with a 2-cm long indentation, which is advanced into the hepatic parenchyma, so that the hepatic tissue is pushed into the indentation. Thereafter, the outer sleeve with its cutting edge is advanced over the inner needle, so that the tissue is sliced off, after which the entire instrument is withdrawn. True-cut needles have a sharp tip, which can easily penetrate other structures, and should therefore only be used under ultrasoundguidance or direct visualization, such as during surgery. True-cut needles can be manual, semi-automatic, or for use with a biopsy-gun. The use of semi-automatic needles is advised for cats. The biopsy gun is expensive, but single-use gun needles are cheap. Thus, a biopsy gun is recommended for centers where biopsies are collected frequently. An advantage of the biopsy gun is that the process is very quick and a small firm fibrotic liver that moves relatively freely in a fluid-filled abdominal cavity can be easily biopsied. As mentioned above, true-cut needles should only be used under ultrasound guid- ance.1,28,29 However, certain true-cut gun devices have such a strong spring driving the needle that the sudden pressure pulse in the liver parenchyma may cause fatal shock in cats; this has not been observed in dogs. It is extremely important, therefore, to verify that a proper device is being used.
7.3.5.2.2 The Menghini aspiration needle1
This type of needle has a tip with a blunt angle, which can penetrate soft tissues, such as the liver, but not the stomach or the intestines. The tip of the needle is used to “palpate” the tissues in order to locate the liver. This needle is usually used blindly, without ultrasound guidance. It does not permit the sampling of focal lesions and is only useful to detect diffuse liver disease, when ultrasound is not available. For populationbased studies of a large series of cases, the Menghini technique has many advantages. Interested readers are referred to the WSAVA Standards for Clinical and Histological Diagnosis of Canine and Feline Liver diseases for further information.1,30
7.3.5.2.3 Fine needle aspiratioι 31-34
Fine-needle aspiration is performed with a 20-22 gauge needle. The aspirate is transferred onto a glass slide and dried before staining with one of several stains, such as May-Grunwald-Giemsa or Diff Quick stain (Harleco, Gibbstown, NJ). Fine-needle aspiration is usually performed under ultrasound guidance in order to sample cells from a focal lesion. However, blind samples can be taken in the area of the 10th intercostal space at the level of the rib to rib-cartilage junction. Hepatic cytology is not suitable for the evaluation of the histological structure of the liver, which is important for the diagnosis of the vast majority of hepatic diseases. However, it is very useful for the detection of tumor cells or hepatic lipidosis. There is no need to test the coagulation status of the patient before a fine-needle aspiration of the liver.
7.3.5.3 Surgical wedge biopsy35
Surgical biopsies may provide larger samples than needle or forceps biopsies. In order to avoid taking a sample from an area of nonspecific subcapsular fibrosis, it is important to take wedge samples that are preferably 2 cm deep. In human medicine, multiple deep needle biopsies are considered superior over wedge biopsies, which are more superficial. Percutaneous biopsy techniques should be used in dogs and cats with hepatomegaly and ultrasonographic evidence of diffuse, uniform hepatic parenchymal disease. A fine needle aspirate of the liver for cytological evaluation is often obtained first because evidence for certain disorders such as vacuolar hepatopathy (i.e., hepatic lipidosis or steroid hepatopathy) and lymphoid neoplasia can be presumptively identified by this method.
If the operator is experienced with the biopsy procedure, there is little time involved and only sedation and local anesthesia of the skin and abdominal wall are required in some dogs. The liver itself is not painful upon puncture with large-core needles. However, in cats it is advisable to perform the procedure under general anesthesia.
Visualized percutaneous needle biopsy, either with the aid of ultrasound or modified laparoscopic equipment,36 allows the selection of the best site or sites and direct or indirect inspection after the biopsy has been collected. In an animal with suspected diffuse or multifocal hepatobiliary disease, multiple biopsy specimens can and should be obtained, which, in general, is considered safe. General anesthesia is required for use of a modified laparoscope. However, ultrasound-guided true-cut needle biopsies are easier to perform and deliver comparable results in most cases.
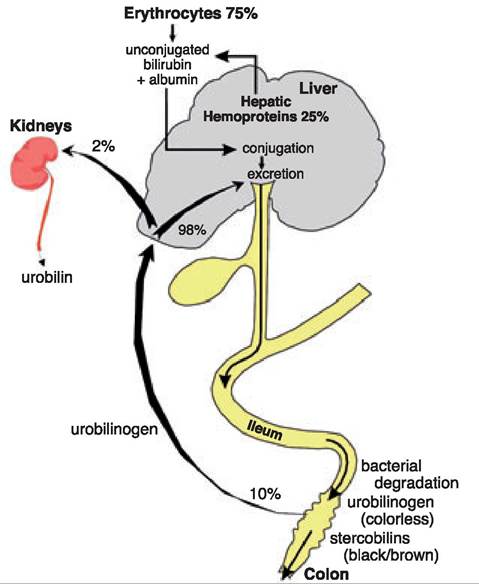
Figure 7.4:
Metabolism of bilirubin. This schematic drawing shows the physiological metabolism of bilirubin. Approximately 75% of unconjugated bilirubin stems from the heme of erythrocytes, while approximately 25% come from hepatic hemoproteins. Bilirubin is conjugated in the hepatocytes and excreted with the bile. In the intestinal lumen, conjugated bilirubin is degraded by bacteria to urobilinogen and stercobilins. Approximately 10% of the urobilinogen is absorbed in the colon, of which 2% is excreted through the kidneys.
As for percutaneous biopsy techniques, liver and /or bile specimens for microbiological culture are aseptically collected first. Then, impression smears for cytological analysis are made by gently touching a specimen to a slide before placing it in fixative. Excess blood is removed by blotting the sample on gauze before the impressions are made. Abnormal populations of cells (e. g., mast cells, lymphoblasts) are readily detectable using rapid stain systems such as Diff Quik. For routine processing and histopathological examination, hepatic tissue specimens are submerged in 10% buffered formalin. Quick fixation is essential and is only possible if the samples are not too thick; therefore, surgical samples should be cut into 2-3 mm thick slices. Samples for copper histochemical staining or tissue quantification are harvested and fixed or preserved according to the specifications of the pathology laboratory selected to do the assays. Other special stains for infectious agents, or fibrous tissue, amyloid, glycogen, or other metabolic products are available and their use must be discussed with the attending pathologist before the tissue specimen is obtained.
7.3.5.4 Gall bladder aspiration
The gall bladder can be safely aspirated under ultrasound guidance using a fine-needle aspiration technique. There is no need to approach the gall bladder transhepatically and any approach is considered safe. Sampling of bile for cytology and culture is especially important in cats, in which infectious cholangitis is one of the most frequent chronic hepatobiliary disorders.
7.4