Physiology
The liver has an enormous reserve capacity and removal of up to 70% of the normal liver can be sustained without any clinical effect. The liver also has a huge regenerative capacity following the loss of hepatocytes.
Liver cells can divide more than 40 times, so that the organ theoretically has the capacity to completely renew itself a number of times. However, when diseased, the regenerative capacity decreases and, at the same time, there is a tendency to produce more non-functional matrix (i.e., hepatic fibrosis). Hepatic growth and regeneration are regulated by growth factors of which hepatocyte growth factor (HGF) is the most important one. HGF is produced in the fat-storing cells (also known as Ito or stellate cells) upon stimulation by stimulation factors, such as insulin-like growth factor (IGF), insulin, and others, that reach the liver with the portal blood supply. Therefore, the supply of portal blood is essential for maintaining hepatic functional mass and regeneration. In turn, animals with congenital portosystemic shunts experience a reduced hepatic growth resulting in an undersized and hypofunctional liver, which usually grows to its nor-mal size and weight within two weeks after surgical ligation of the shunt. Another feature making the liver highly flexible in facing changing demands is the fact that its metabolic and transport processes follow the Michaelis-Menten kinetic curve. These processes are therefore capable of adapting to changing substrate concentrations; however, they are also saturable and adaptation is, thus, not unlimited. The liver plays a key role in many metabolic processes and in homeostasis. In general, the organ detects the metabolic requirements of the extrahepatic tissues and responds by metabolic adaptation.
The plasma concentrations of glucose and many proteins are regulated by the liver, and may be reduced in patients with hepatic dysfunction.
In order to be able to be transported through the vascular system, triglycerides from adipose tissue or intestinal chylomicrons are converted into lipoproteins by the liver. Other metabolic functions of the liver include the biotransformation of endogenous products varying from ammonia to steroid hormones and the removal of exogenous toxic products (e. g., toxic chemicals and endotoxins from intestinal bacteria). A number of toxic substances are directly excreted by the liver (e.g., heavy metals), while others are modified by the liver and then released into the circulation in a form that can be excreted by the kidneys (e.g., uric acid is converted to allantoin, ammonia to urea, and steroids are transformed and conjugated). Large molecules with molecular masses above 300 Da are preferentially excreted into the bile after being conjugated to make them more hydrophilic. Another important metabolic function of the liver is the production of primary bile acids from cholesterol (Figure 7.3).Apart from all these metabolic functions, the liver also has the capacity to store many substances for future use; examples are glycogen, metal ions, and vitamins. The liver is also capable of producing red blood cells, a function which is physiologically present during embryonic life. Hepatic extramedullary hematopoiesis may be regained and is often found in patients with anemia.
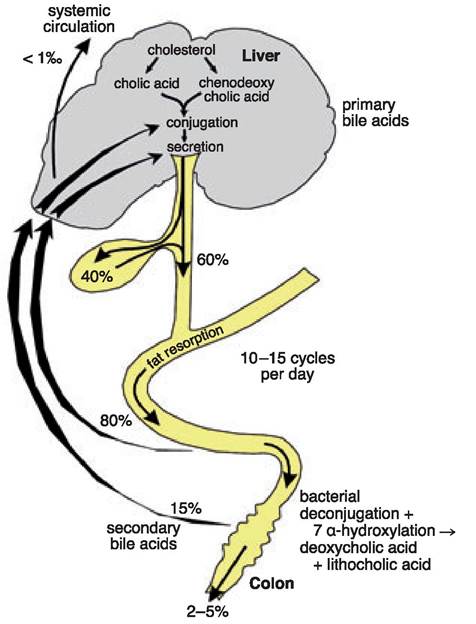
Figure 7.3:
Bile acid metabolism and enterohepatic circulation. Hepatocytes produce bile acids from cholesterol. These primary bile acids are conjugated by the liver and then secreted in the bile. Approximately 40% of primary bile acids get stored in the gall bladder, while 60% reach the small intestine directly. Eighty percent of primary bile acids get re-absorbed in the ileum, while the rest is deconjugated and hydroxylated to secondary bile acids in the large bowel. The majority of these secondary bile acids are reabsorbed, while a small portion is lost in the feces.
The enormous functional reserve, the exceptional regenerative capacity, and the metabolic flexibility of the liver are responsible for the fact that many liver diseases only cause clinical symptoms when the disease has become chronic and a large portion of its functional and regenerative reserves have been lost.
Acute or subacute diseases are often subclinical or only result in mild clinical signs that can easily be overlooked.Another factor is that the liver is intrinsically involved in the function of many extrahepatic tissues, so that hepatic dysfunction often leads to clinical signs that indicate dysfunction of other organs. Finally, clinical signs encountered in patients with liver disease are commonly nonspecific. Therefore, hepatic diseases are often associated with clinical signs that do not immediately point to the liver, but to a general dysfunction of vital organs. Also, in most cases, it is not possible to differentiate clinically between different causes of liver disease. However, there is some sublobular specialization of hepatocytes which may aid in diagnosis that is summarized in Table 7.1.
7.3