Diarrhea in Neonatal Foals
Guy D. Lester
Diarrhea occurs frequently in foals of all ages and represents one of the most common medical conditions requiring veterinary intervention. The approach to diagnosis can be difficult, and establishment of a definitive diagnosis in a field setting is uncommon.
The veterinarian must therefore consider a number of factors in order to construct a list of most likely causes. These factors include the ages of the affected animals, numbers of foals affected, volume and character of the feces, and duration of signs. There are some limited diagnostic tests that can be used to rule in or out many of the common causes of foal diarrhea.In some foals, diarrheal diseases are associated with signs of colic. The abdominal pain can be severe and can mimic that seen in foals with strangulating intestinal lesions making case management difficult. Colicky signs frequently precede the onset of diarrhea. Passage of a nasogastric tube is equally important in colicky foals as it is in adults. Foals with intestinal ileus or inflammatory diseases of the small intestine will commonly produce large volumes of gastric fluid on reflux. The control of pain is required in order to reduce the chances of injury and to facilitate evaluation. Intramuscular butorphanol can be helpful in providing pain relief in foals with colitis. α2-Adrenergic agonists should be used with caution in neonates due to their depressive effect on the cardiopulmonary system. If they are to be used, then start with lower doses or consider combining with butorphanol. Nonsteroidal antiinflammatory drugs should be avoided until a diagnosis is established. Neonatal foals generally tolerate flunixin well but require a slightly larger dose rate but reduced frequency when compared with older animals.
There are many causes of diarrhea in young foals including bacteria and bacterial toxins, viruses, nutrition, parasites, and antibiotic usage.142 Normal physiologic adaptive processes can also produce diarrhea in most foals.
The intestinal microbiota of newborn foals is described as “complex” as early as 24 hours of age.359 The flora develops over the first weeks of life such that by 60 days of age it resembles that of an adult.Bacteria
Escherichia coli is the most important mediator of systemic sepsis in newborn foals but is not a common primary cause of diarrhea in this age group. The organism is common in normal horse feces and is frequently isolated from animals with diarrhea,360 but in the absence of typing the role of E. coli is highly questionable. There are rare reports implicating an association between E. coli and diarrhea in foals. Enterotoxigenic E. coli was isolated from a 3-day-old diarrheic foal.361 The isolate was of the 0101 serotype, was LT-like toxin positive, but negative for STa. Earlier inoculation studies indicated that F4 (formerly K88)- positive E. coli was not likely to cause diarrhea in foals, although may have a synergistic role in foals infected with other potential pathogens, such as rotavirus.362
Intestinal disease mediated by Clostridial toxins occurs in foals worldwide. The toxins are most commonly derived from biotypes A and C of Clostridium perfringens or from Clostridium difficile. Classical intestinal clostridiosis of foals is caused by C. perfringens biotype C and is characterized by colic, rapid dehydration, cardiovascular collapse, and hemorrhagic diarrhea. The disease occurs most commonly in foals younger than 10 days of age; often younger than 36 hours of age. It is associated with a high mortality, and outcomes are rarely influenced by treatment.363 Death may occur rapidly and occasionally before any diarrhea has been passed. Biotype C produces both α and β toxins along with variable amounts of enterotoxin. Cases can occur sporadically or as outbreaks and, on some farms, occur annually presumably associated with carriage in specific mares. Biotype A of C. perfringens has become well recognized as a specific cause of foal diarrhea over the past decade.
Biotype A produces α toxin and enterotoxin and is associated with a slightly lower mortality rate than biotype C. Affected foals are more likely to respond to directed or supportive care. The development of clinical signs is rapid, and diarrhea may or may not contain blood; in the author's experience, passage of bloody diarrhea is common but usually transient. Reported risk factors for C. perfringens diarrhea in neonatal foals in Colorado include breed (stock horse type), birth on dirt, sand, or gravel, housing in stalls or on dry lots during the first 3 days of life, and maternal feeding practices. Feeding a low-grain diet prepartum was associated with a decreased risk of neonatal disease.363 Hematologic findings are consistent with toxemia. This includes hemoconcentration; an initial leucopenia, characterized by a neutropenia with a left shift to immature forms and toxicity; and a lymphopenia. Chronic cases may develop a rebound leucocytosis and hyperfibrinogenemia. Altered coagulation may be evident clinically through prolonged bleeding or spontaneous hemorrhage, or through a propensity to develop thrombosis.A definitive diagnosis of C. perfringens diarrhea is rarely established in practice. The diagnosis is usually based on signalment, clinical features, and outcome, rather than detection of specific clostridial toxins. Positive fecal culture is strongly supportive, noting that healthy foals may shed low numbers of C. perfringens. Identification of toxin is ideal but is limited due to availability of appropriate commercial assays. Fecal enterotoxin detection assays are available but lack sensitivity, particularly with biotype C isolates. Biotyping of C. perfringens '1 C 1 11'1' 1 1'
isolates after culture can be achieved using polymerase chain reaction (PCR) analysis for toxin gene sequences. This may be helpful in increasing the accuracy of the diagnosis but again falls short in establishing a definitive cause. Fecal Gram stain is easy to perform and may support an early clinical suspicion of disease if there are abundant numbers of large gram-positive organisms or spores present.
C. difficile can produce an identical clinical syndrome to C. perfringens, although it appears to be more variable with respect to fecal blood. The two pathogens were isolated together in several foals with fatal hemorrhagic diarrhea.364 C. difficile also occurs as sporadic cases or as clusters or outbreaks. Identical strains can be recovered in mare-foal pairs, indicating cross- infection.365 It is important to recognize that clostridial infection can produce a severe inflammatory syndrome that is restricted to the small intestine and may not cause diarrhea. Affected foals can present with signs that mimic strangulating small bowel disease, including severe abdominal pain, gastric reflux, and sanguineous peritoneal fluid. Two principal toxins can be liberated from C. difficile: an enterotoxin (toxin A) and a cytotoxin (toxin B). Both nontoxigenic and toxigenic strains exist and can only be differentiated after culture using molecular techniques. Consequently, commercial toxin tests (available for both toxin A and B) are recommended in addition to fecal culture to establish a diagnosis. As with C. perfringens cases, a fecal Gram stain can also increase suspicion. Hematologic changes associated with C. difficile infection can mimic those associated with C. perfringens disease.
Most cases of clostridial enterocolitis require aggressive medical intervention, irrespective of clostridial type. Antimicrobial therapy should be both specific and broad spectrum. Targeted antimicrobial treatment typically includes both metronidazole and penicillin. The majority of affected foals will require, at a minimum, intravenous crystalloid solutions. Some will also benefit from plasma or synthetic colloids and inotrope and vasopressor therapy. Additional therapies include C. perfringens biotype C and D antitoxin, di-tri-octahedral smectite clay, and lactase enzyme replacement.366,367 The use of C. perfringens antitoxin and toxoid is off-label and not without some risk.
Pretreatment with antihistamines has been suggested before antitoxin.366 Prevention of clostridial enterocolitis centers on hygienic housing practices and avoidance of overfeeding of late-pregnant mares. Affected foals and their mares should be isolated, and strict protocols instituted to limit cross contamination. Administration of C. perfringens type C and D toxoid to pregnant mares has been used with anecdotal success on farms with recurrent problems with C. perfringens biotype C. The use of prophylactic metronidazole is highly controversial but understandable on properties with a high disease prevalence. Some isolates of C. difficile are reportedly resistant to metronidazole,366 and although this appears to be dependent on geographic location the widespread prophylactic use could promote resistance. Prophylactic use of probiotic preparations are commonly recommended, but there are conflicting efficacy data.368-371Bacteroides fragilis is a gram-negative anaerobic rod and occurs in both enterotoxigenic and nonenterotoxigenic forms. Enterotoxigenic strains of B. fragilis have been incriminated with diarrhea in several species, including lambs, calves, pigs, humans, and foals.372 Enterotoxigenic B. fragilis was isolated from young foals (aged 2 to 60 days) with diarrhea.373 Half of these foals had other potential pathogens detected, including Salmonella or rotavirus. In a study reviewing 20 isolates of B. fragilis from hospitalized foals with diarrhea, only 4 had the 372
enterotoxin gene.372 Ihe most common isolate from foal feces was a nonenterotoxigenic strain casting doubt as to clinical relevance.
Enterococcus (Group D Streptococcus) durans has also been implicated as a cause of diarrhea in foals.374 Similarly, Aeromonas hydrophila was isolated more commonly from foals with diarrhea than control animals, suggesting a potential role in foal diarrhea.375 Rhodococcus equi is an important cause of pulmonary disease in foals.
Although abdominal involvement appears common, the relevance of R. equi as a significant primary enteric pathogen, in terms of number of animals affected, is likely small. An intestinal syndrome has been directly attributed to R. equi that involves necrosis of the small intestinal Peyer’s patches and multifocal thickening and necrosis of the cecum and large intestine.376 The changes include multiple areas of intestinal ulceration with an associated mesenteric lymphadenopathy. The diagnosis of R. equi ulcerative colitis is difficult for a variety of reasons. In contrast to Salmonella infection, where recovery of the organism from the feces has significance, the recovery of R. equi is common in asymptomatic animals. Up to 100% of foals older than 2 weeks of age may shed large numbers of the bacteria.35Salmonella infection of neonatal foals is also associated with high mortality. As with clostridial infection, cases can occur sporadically or as part of an outbreak. Mares provide the most important source of Salmonella to newborn foals, but it is rare that both mare and foal will develop clinical disease. Clinical signs can become apparent by 24 hours of age but are more common in older foals. The severity of signs is related to virulence of the serotype involved, inoculation dose, and level of host immunity. In contrast to adult infections, detectable bacteremia occurs commonly in affected foals. Consequently, foals that may survive the initial intestinal or systemic disease remain at risk for secondary complications that include osteomyelitis, synovitis, meningitis, uveitis, hepatitis, or pyelonephritis. In some foals these complications may not become clinically apparent until days or weeks after resolution of enteric disease. Therefore appropriate and sustained broadspectrum antibiotic therapy is important in known affected foals. The selection of antibiotic should be based on known sensitivity patterns understanding that in vitro sensitivity may not accurately translate into clinical efficacy due to the intracellular location of Salmonella. For example, the limited distribution of aminoglycosides can lead to therapeutic failure despite often promising in vitro sensitivity.
Viruses
Rotavirus is the most common cause of infectious diarrhea in foals. There are seven known groups of rotavirus (A through G) and many different serotypes within each group. Group A is the primary cause of rotaviral diarrhea in foals with G3 the most common serotype.377 Rotaviruses have the ability to change their surface proteins over time, and this rearrangement of gene segments takes place during coinfections with other strains. This leaves the possibility for many variations of the virus.
Transmission may be direct from animal to animal or indirect through fomites. Disease occurs after a short incubation period. Experimentally, this period may be as brief as 48 hours.378 Rotavirus replicates within the intestine and invades the lining of the proximal small intestine causing villous cell death and a resultant loss of absorptive area. Diarrhea may result from several mechanisms: (1) a loss of absorptive capacity coupled with a decrease in lactase production can lead to an osmotic load of undigested lactose delivered to an immature hindgut; (2) a compensatory crypt cell proliferation may cause an increase in intestinal secretion; and (3) the virus produces an enterotoxin that causes or contributes to the development of diarrhea. The putative viral enterotoxin and cytotoxin, NSP4, is a nonstruc- tural glycoprotein of rotavirus that is released from virus-infected enterocytes.379 NSP4 is a noncompetitive inhibitor of the Na-glucose symporter and also enhances intestinal chloride secretion.
Disease can be seen between 2 and 160 days of age but is most common in foals younger than 60 days. Indeed, most clinical infections probably occur between 5 and 35 days of age. The presence and severity of diarrhea are highly dependent on the degree of hindgut maturation. Consequently, infection in foals younger than 2 weeks of age may result in lifethreatening watery diarrhea, whereas infected older foals may have minimal or no diarrhea due to effective colonic compensation of osmotic and fluid loads. Diarrhea when present is often watery but nonfetid in odor.
There is serologic evidence that broodmares may have an important role in propagation of the virus within a herd. Infections can occur as isolated cases or as outbreaks following periods of overcrowding and stress. Shedding after infection is usually complete by 10 days after the cessation of clinical signs but may occur intermittently for up to 9 months.380 The virus can persist in the environment for up to 9 months, and disinfection usually necessitates the use of substituted phenolic compounds.
The diagnosis of rotaviral diarrhea is based on an appropriate signalment, clinical signs, and detection of the virus in feces. Tests include electron microscopy, commercial immunoassays (enzyme-linked immunosorbent assay [ELISA] or latex agglutination), and PCR. Several diagnostic companies and university laboratories have developed comprehensive equine diarrhea PCR panels that include rotavirus. Virus is shed in large concentration early on during infection. Central to the management of affected foals is maintenance of hydration through enteral and/or intravenous fluid therapy.
Prevention involves good hygiene and reduction in crowding. Vaccination of mares during pregnancy has yielded variable results in terms of efficacy., !here is some evidence to suggest that vaccination may at a minimum delay the onset of disease, thereby reducing both the severity and duration of diarrhea.
Coronavirus can cause diarrhea in foals during the neonatal period. It was originally thought to be an uncommon but severe cause of diarrhea.383,384 Survey data using real-time PCR analysis indicated a high rate of carriage in both healthy and diarrheic foals.385 Antemortem diagnosis can also be made using electron microscopy, serology, or commercial fecal-capture ELISA. As with rotaviral infection, shedding is greatest in the early stages of disease.
Parasites
Strongyloides westerii is a common parasite of foals, with early infection of the foal occurring through mare's milk. Experimental studies have indicated that higher numbers of infective larvae than are found in milk are needed to produce diarrhea.386 Furthermore, foals with high egg counts are often asymptomatic.
Cryptosporidium parvum is not considered to be an important pathogen of foals in terms of numbers of animals diseased, although it can be a problem in specific locations.387 On the basis of epidemiologic studies, the parasite appears to be concentrated in some breeding operations.388 Foals diseased with Cryptosporidium shed enormous numbers of infective oocysts into the environment. The parasite is considered to be coccidian-like but differs from coccidia in terms of size (4 to 6 μm diameter compared with 23 to 34 μm for other coccidia), host specificity (not host specific), pathogenesis (only invades epithelium), and drug sensitivity (resistant to many drugs). Infection is by the fecal-oral route. The oocysts can survive in the soil or water for months. They do not require a period of sporulation outside of the host to become infective. In a study of asymptomatic foals, between 15% and 31% of foals were shedding Cryptosporidium, and that shedding began between 4 and 19 weeks of age and persisted no more than 14 weeks.389 All shedding had ceased by weaning and was not identified in adult horses. The diagnosis is usually made through microscopic examination of the feces. Acid fast or Ziehl-Neelsen stains are required to detect oocysts. Immunofluorescence assays and flow cytometry techniques have also been described. C. parvum infection may be seen with concurrent enteric or systemic infections. The disease is generally self-limiting in immunocompetent animals. Historically, the pharmacologic control of Cryptosporidium has been difficult, but paromomycin, nitazoxanide, or azithromycin may be efficacious. The organism is potentially zoonotic, and transmission from foals to humans is reported.390
Giardia may be found in normal foals with infection rates reported from 17% to 35%.389 Giardia is present in all age groups, and it is believed foals acquire infection from nursing mares. Concurrent infection with Cryptosporidium and Giardia may be observed. Disease should be suspected if large numbers of parasites are seen on fecal analysis. Affected animals should respond within a few days to treatment with metronidazole; failure to respond should alert to other pathogens.
Nutritional Causes
Nutritional causes of diarrhea include overingestion of milk (as might occur when the mare and foal are separated and rejoined) or overfeeding orphaned or sick foals. Overwhelming the ability of the small intestine to digest and absorb results in presentation of milk to the colon, where it is fermented and produces osmotically active sugars and acids. In a controlled study of foals younger than 5 days of age, an elemental isotonic diet produced diarrhea in healthy foals when fed as the sole source of nutrition. Older foals fed a similar diet apparently did not develop diarrhea.391 Orphan foals and foals fed commercial mare milk replacer may experience diarrhea associated with these diets. Foals that are fed raw cow's milk frequently experience diarrhea and failure to thrive. Cow milk replacer uncommonly causes diarrhea but remains a less than ideal replacement. In contrast, foals fed goat's milk grow well and rarely develop diarrhea, although they may develop a metabolic alkalosis of minimal to no clinical significance.
Transient lactase deficiency has been proposed in foals. An oral lactose tolerance test is conducted after a 4-hour fast. Foals are administered 1 g/kg of body weight of a 20% solution of lactose powder and observing an increase of plasma glucose of 35 mg/dL (1.9 mmol/L) by 90 minutes.392 Agents such as rotavirus that damage epithelial cells may cause prolongation of the diarrhea because of temporary lactase deficiency.
Foal Heat Diarrhea
Diarrhea developing during days 5 to 14 of life has been termed “foal heat diarrhea” because of the time relationship to the occurrence of postfoaling estrous in the mare. Diarrhea has developed in foals in this age group that have been raised separated from the dam on a consistent diet and isolated from pathogens, so it does not appear to be causally related to estrous. The most likely cause of foal heat diarrhea is the establishment of normal flora in the hindgut. Foal heat diarrhea is typically preceded by coprophagy 2 to 3 days before the onset of diarrhea. Classical foal heat diarrheas are mild and require no specific therapy. Continued diarrhea, fever, or depression with signs of reduced sucking activity on the mare should raise concern
of other etiologic agents with appropriate diagnostic testing and treatment.
Treatment and Prognosis
The three main components of therapy of diarrhea in the neonatal foal consist of (1) fluid therapy (either oral or intravenous), (2) intestinal protectants/adsorbents, and (3) antibiotics if indicated to treat suspected bacteremia or clostridiosis. Sodium-containing isotonic intravenous fluids are an important component of diarrhea therapy in the compromised neonate. Potassium is lost in severe diarrhea and, if hyperkalemia is not present, should be supplemented by adding 15 to 20 mEq/L of KCl to fluids. Foals that are not nursing normally may have hypoglycemia and may need glucose-containing fluids. Acid base correction by volume expansion and replacement of bicarbonate can be lifesaving and should be monitored frequently when significant intestinal fluid losses occur.
Ideally milk should not be withheld from foals with diarrhea. The clear exceptions are foals with colic and those with bloody diarrhea. The foal can be muzzled for 8 to 12 hours while the mare is milked out, and the foal provided oral fluids through stomach tube or a bottle if a suck reflex is present. Although labels of electrolyte replacers do not always specify for use in foals, many preparations used in calves have been used in foals. Most of these preparations provide insufficient energy and should be used for short intervals of no more than 24 to 36 hours unless parenteral nutrition of some type is provided to maintain blood glucose levels.
Intestinal protectants may be all that are required in uncomplicated cases or may be used in conjunction with other therapies. Bismuth subsalicylate, kaolin or pectin, and activated charcoal have been used for this purpose. Suggested advantages of bismuth subsalicylate are its neutralization of bacterial toxins and antisecretory effect through its local antiprostaglandin activity. DTO smectite clay is also commonly used in the management of diarrhea.
Systemic antibiotics should be used in the neonate with diarrhea that may have systemic sepsis or compromised immunity. Blood cultures should be obtained before initiation of antimicrobial therapy. Antibiotics with a spectrum against gram-negative and gram-positive organisms should be used. In general terms, renal toxicity associated with aminoglycoside use is uncommon in clinical practice. The clear exception is the foal that is dehydrated, most commonly due to ongoing losses through diarrhea. Consequently, the monitoring of renal function is indicated when using potentially nephrotoxic drugs.
Plasma therapy for hypoproteinemia associated with failure of passive transfer or protein-losing enteropathy is useful to maintain plasma oncotic pressure and expected protein binding of medications. Diarrheic foals with albumin levels below 20 g/L or total plasma protein levels less than 42 g/L may benefit from plasma therapy.
Prevention and Control
Prevention is best accomplished by minimizing density of populations of horses, separating of age groups, providing appropriate sanitation and hygiene, and obtaining adequate colostrum of good quality (see Chapter 53). The risk of neonates developing diarrhea in a hospital environment is increased with the use of histamine type 2 receptor antagonists or omeprazole.134
Distended and/or Painful Abdomen
Evaluation of the colicky newborn or older foal often presents a diagnostic challenge. As with adults, differentiation between surgical and nonsurgical abdominal diseases is often the primary focus in any evaluation of abdominal pain in foals. Rectal palpation, one of the most important diagnostic aids used in the assessment of adult animals with colic, is limited to digital palpation in foals for obvious reasons. This size limitation does, however, allow other diagnostic modalities to be used effectively, such as US and plain and contrast radiography.
The most commonly used analgesics in colicky neonatal foals include flunixin and butorphanol. Xylazine can be used, but care is needed in sick foals as the drug is associated with significant hypotension. Another important procedure is to pass a nasogastric tube and check for gastric fluid accumulation, a critical aspect of examination of the adult horse with colic but often overlooked in neonatal foals.
The decision to select certain diagnostic tests is based on a number of historical and physical examination findings. The duration and severity of signs, together with evaluation of response to chemical analgesia, will often dictate surgical versus nonsurgical management. Severe, unrelenting pain that is poorly or unresponsive to analgesics is often unto itself a valid criterion for surgical exploration. The decision to explore the abdominal cavity in the newborn should not be taken lightly, as this age group appears more susceptible to the consequences of adhesion formation postoperatively.393 A thorough physical examination is key as many gastrointestinal diseases in young foals can occur either as a secondary manifestation to other diseases (e.g., sepsis or prematurity) or in coexistence with other disorders that could impact adversely on either short- or long-term survival.
The evaluation of a colicky foal can often be guided initially by the presence or absence of gross abdominal distention. In young foals, this can be monitored by repeated use of a measuring tape around the abdomen. The position of the tape can be maintained in a constant site by clipping a small mark over the dorsum. The most frequent cause of an enlarged abdomen is gas accumulation within the intestinal lumen, most commonly the cecum and/or large colon. It may be important to determine if the gas is maintained within the intestinal tract or if it is free within the peritoneal cavity. This is particularly true in foals with clinical and/or hematologic evidence of sepsis or toxemia. Free peritoneal gas can be detected by US examination or, more easily, by plain radiography. This can occur secondarily to abdominal rupture or by inadvertent puncture or laceration of the bowel during attempted abdominal fluid collection.
Newborn foals with uroperitoneum can present with abdominal distention and low-grade pain. Differentiation between gas and fluid can generally be made by careful physical examination and confirmed by US examination. Typically, a large amount of free peritoneal fluid is noted and a free-floating empty bladder is clearly seen caudal to the umbilicus. If maintained on a milk diet, most neonates with uroperitoneum will develop the classical electrolyte derangements: hyponatremia, hypochloremia, and hyperkalemia. Foals that develop uroperitoneum during treatment of other diseases (e.g., necrotic urachus in a foal with systemic sepsis) may not develop the classical changes if maintained principally on replacement solutions intravenously.
An US examination of the foal abdomen is best done with the foal in a standing position. The ventral abdomen is clipped, and a coupling gel is applied in a liberal manner. A linear or sector probe with a frequency range between 5 and 7.5 MHz is the most common probe type used for routine scanning. In older foals and adults, a lower frequency probe is needed to provide deeper penetration into the abdomen. In newborn foals every abdominal US should include examination of all umbilical structures, including both arteries, vein, urachus, and urinary bladder. The intestines should be evaluated for wall thickness (should be 340 days) are at greater risk. Large intestinal volvulus occurs infrequently in newborn and young foals and, as with catastrophic small intestinal lesions, should result in a period of violent abdominal pain. However, signs of severe pain may not be evident in some foals with other concurrent diseases, such as overwhelming sepsis or hypoxic-ischemic encephalomyelopathy. Contrast radiography using barium sulphate is helpful in defining problems related to gastric-emptying, small intestinal obstructive diseases and, when administered as an enema, can be helpful in identifying impactions or congenital abnormalities, such as atresia coli.

FIG. 17.14 Abdominal radiograph (lateral recumbency) of a 7-hour-old foal with atresia ani, showing meconium retention in a gas-filled large colon.
When given as an enema, up to 20 mL/kg of a 30% wt/vol suspension may be administered through a 24-French Foley catheter with an inflated cuff. Although not reported, rectal or colonic rupture could complicate the technique, particularly if the mucosa is inflamed and friable. For an upper gastrointestinal series, typically 5 mL/kg of barium sulfate is administered via a nasogastric tube and films are taken at times 0, 5, 15, 30, 150, and 270 minutes. An upper gastrointestinal contrast study should be avoided in foals with spontaneous gastric reflux or in foals with known small intestinal distention, as gastric rupture or aspiration of the contrast material could occur.
Congenital anomalies should be considered in all colicky newborn foals. Common abnormalities include atresia coli, atresia recti, and atresia ani. Plain radiography and digital examination of the anus and rectum will identify many of these foals. Contrast radiography may further identify others, hopefully avoiding the expense of exploratory celiotomy. White foals born to overo-overo or overo-tovero matings are at risk for intestinal agangliosis with or without atresia or stricture formation, so-called lethal white foals (Fig. 17.16). A careful digital examination in a young foal can provide key information including assessing patency of the anus and rectum. Fecal consistency can also be evaluated.
Peritoneal fluid evaluation is a useful adjunct to the diagnostic work-up of some foals with abdominal pain. The incidence and severity of complications associated with this procedure in foals are greater than that in adults. Therefore, fluid collection should not be routine but reserved for cases where

FIG. 17.15 Normal standing radiograph in a neonatal foal. Note the prominent fluid line in the stomach and presence of gas in various portions of the intestinal tract.

FIG. 17.16 A lethal white foal with colic at 18 hours of age.
the distinction between surgical and medical diseases is not clear. Complications can be minimized by identifying pockets of fluid using US and by using a blunt instrument, such as a bovine teat cannula. Hypodermic needles can cause laceration if the foal moves suddenly during the procedure but are safe and efficient where a large amount of fluid is present. The technique should be avoided, if possible, in conditions with extensive accumulation of large intestinal gas.
Specific Conditions
Meconium Impaction
Meconium impaction is the most common cause of the colic in the newborn foal. This condition is more common in colts due to the narrow pelvic canal. Many foals show some degree of straining and discomfort while passing meconium, but in most instances it is passed uneventfully by 24 to 48 hours of age. The meconium most commonly becomes impacted in the rectum or small colon. The clinical signs associated with meconium impaction in the otherwise normal foal include repeated attempts to defecate, straining with the back arched, swishing of the tail, and restlessness. Nursing stimulates defecation through an oral-rectal reflex, so signs of discomfort may appear shortly after each milk meal. If left untreated, meconium impactions lead to varying degrees of abdominal distention. The foal's abdomen becomes gas distended with tympany detected over the paralumbar fossa. Digital examination often reveals a rectum packed with hard fecal balls. Occasionally, the impaction is located more proximally (large or small colon) and radiography or ultrasonography is required for diagnosis.
Low doses of analgesics such as flunixin meglumine (0.25 to 1.0 mg/kg IV) and butorphanol (0.01 to 0.1 mg/kg IV) may be required to prevent self-trauma during colicky episodes. Xylazine may exacerbate gut stasis and can cause respiratory depression and should be used with caution in newborn foals. A gravity enema with mild soap and warm water or a commercial enema usually results in prompt evacuation of the meconium. Refractory meconium impactions may respond to 4% acetylcysteine retention enemas. The supplies and procedure for a retention enema are as follows: Mix together 150 mL water, 6 g of acetylcysteine powder, and 20 g of sodium bicarbonate (baking soda). Alternatively, commercial acetylcysteine solution (acetylcysteine [Mucomyst] solution, 100 or 200 mg/mL) can be used. Insert a well-lubricated 12- or 14-French, cuffed Foley urinary catheter into the rectum and inflate the cuff. Slowly infuse 120 to 180 mL of the retention enema solution. Plug the end of the catheter. Tape the catheter loosely to the foal's tail. Leave in place a minimum of 15 minutes and then deflate the cuff and remove the catheter. This procedure can be repeated several times. Care must be taken to avoid traumatizing the rectal mucosa by stiff tubing or multiple enemas with harsh detergents. Clinical signs associated with meconium impaction in the compromised foal may be absent. In asphyxiated or premature individuals that are receiving little or no enteral feeding, meconium may remain in the large colon for days, gradually forming into hard concretions that are diagnosed by palpation or radiographs or at postmortem examination. In these cases the routine administration of an enema is often ineffective in mobilizing the impaction because it is high in the large colon. Additional therapy includes IV fluids, oral fluids, and laxatives (60 to 120 mL of mineral oil with 0.5 to 1 oz of psyllium, 60 to 120 mL of Milk of Magnesia). If the gas distention becomes severe, transcutaneous bowel trocariza- tion can be pursued. The author avoids the use of DSS as an oral cathartic because it can cause excessive irritation resulting in diarrhea and colic. Analgesics may also be helpful in controlling the neonate's discomfort and to reduce the risk of selftrauma. Although most meconium impactions can be successfully treated with aggressive medical therapy, those few foals that are refractory to treatment or display uncontrollable pain are candidates for surgical intervention.
Uroperitoneum
Uroperitoneum is a relatively common cause of abdominal distention and depression in the neonatal foal. The condition predominates in males but may occur in females as well. Uroperitoneum may be congenital or acquired. The congenital form occurs due to failure of the dorsal wall of the bladder to close during development. The most common cause of uroperitoneum is a ruptured urinary bladder, but other sites in the urinary tract may also leak, including the ureters, urachus, and urethra. Most cases of ruptured bladders are presumed to occur during parturition because of external pressure on a distended bladder. This form occurs most commonly in colts. Uroperitoneum can also occur secondary to ischemic necrosis or infection of the urinary bladder or urachus in the compromised foal. Critically ill, recumbent foals may rupture their bladders while being lifted and turned with a full bladder or from chronic overdistention associated with their generalized disease state. Foals with botulism may also rupture their bladder secondary to bladder atony and chronic overdistention. Older foals of either sex may experience bladder rupture secondary to focal infection of the umbilical arteries and/or urachus, or ischemic necrosis of the apex of the bladder.
Clinical signs of uroperitoneum are rarely noticed before 48 to 72 hours of age, particularly if the foal is not being watched closely. The first signs may be urinary incontinence or frequent attempts to urinate, with only small amounts voided. Sometimes, particularly in those animals that rupture sometime after birth, there is a history of a period of normal urination, which at some point stopped or became abnormal. Loss of suckle, mild colic, and increasing abdominal distention are usually accompanied by worsening depression and increasing heart and respiratory rate. If the condition is allowed to persist, foals become increasingly weak and dyspneic and may present in cardiovascular collapse. Fillies with ruptured ureters have been reported to have a characteristic protruding perineum, presumably as a result of retroperitoneal accumulation of fluid.394
Laboratory findings commonly associated with uroperitoneum are elevated serum creatinine and blood urea nitrogen, hyperkalemia, hyponatremia, hypochloremia, and metabolic acidosis. These changes are probably a result of the normal diet of the foal (milk being relatively high in potassium [25 mEq/L] and low in sodium [12 mEq/L]) and the third spacing of urine in the peritoneal cavity. With urine potassium concentration relatively higher than serum and urine sodium concentration lower than serum levels, the net effect of partial equilibration of serum with peritoneal fluid across a semiperme- able membrane is hyponatremia and hyperkalemia, along with an inability to excrete the waste products of metabolism. Hyperkalemia may be severe enough to induce potentially fatal bradyarrhythmias. In hospitalized foals that developed uroperitoneum as a secondary complication, these typical electrolyte abnormalities are not consistently observed. Because most of those foals were receiving replacement intravenous fluids (high in sodium, low in potassium) and very little milk, it was theorized that intake has a great influence on the electrolyte abnormalities associated with uroperitoneum.395 On the other hand, the electrolyte abnormalities typically associated with uroperitoneum are not pathognomonic for that disorder. Foals with renal failure, blocked urethra, white muscle disease, and enteritis have shown the same electrolyte changes.
A diagnosis of uroperitoneum often can be made quickly using transabdominal US and a 5- or 7.5-MHz transducer to visualize large volumes of free, nonechogenic fluid within the abdomen and a small, irregularly shaped, collapsed bladder. Abdominocentesis usually produces a free flow of peritoneal fluid that contains a low cell count, low specific gravity, and at least twice the creatinine concentration of peripheral blood. If the creatinine is the same in both serum and peritoneal fluid, other explanations for the clinical signs should be investigated. The WBC count, total protein, and cytology of the fluid should also be determined. Most uncomplicated cases of ruptured bladders have fairly normal values for peritoneal fluid. In some cases, however, an increased WBC count and total protein and the presence of bacteria may suggest peritonitis. This may be a result of the urine in the abdomen, but more commonly there is a primary ongoing infectious problem (necrotic urachus or bladder, enteritis) and the prognosis becomes worse. If laboratory facilities are not available, new methylene blue can be injected into the bladder using a urinary catheter, and a few minutes later a sample of peritoneal fluid should have a blue discoloration if a ruptured bladder is present. However, this technique may not detect other causes of uroperitoneum such as a ruptured ureter or distal urachus. Positive contrast cystography using a 10% solution of water soluble media may be helpful in detecting the location of the urinary tract leakage. The ability to obtain urine on catheterization of the urinary bladder does not rule out uroperitoneum. Hematology and blood cultures should be performed to detect primary or secondary sepsis.
Treatment of uroperitoneum is surgical repair. However, the foal with uroperitoneum should not be rushed to surgery without first carefully stabilizing it. Serum electrolytes and blood gases should be run to determine the extent of hyperkalemia, hyponatremia, and acidosis present. Although the total amount of water in the body is usually grossly increased by the peritoneal accumulation of urine, effective circulating volume may be drastically reduced. If the eyeballs are sunken and pulse quality and capillary refill time are poor, aggressive fluid therapy is indicated to support the circulation. This is best performed by concurrently removing as much fluid as possible from the abdomen with a teat cannula, 14G catheter, or peritoneal dialysis catheter to avoid worsening fluid overload and respiratory distress. The fluids of choice to treat the typical electrolyte alterations associated with uroperitoneum are saline, dextrose, and possibly sodium bicarbonate solutions, depending on the degree of acidosis present. In most instances continuous dextrose infusion is effective in decreasing the serum potassium level to an acceptable level, but values should be rechecked before anesthesia is induced. Insulin and dextrose may also be used to treat hyperkalemia, but the patient must be monitored for hypoglycemia. One suggested regimen is regular insulin at 0.1 to 0.2 U/kg subcutaneously or intravenously accompanied by a continuous IV dextrose infusion (4 to 8 mg/kg/min). Some individuals also have pleural fluid accumulation and atelectasis secondary to the abdominal distention, so oxygenation and ventilation during and after surgery should be closely monitored. Broad-spectrum antibiotics should be started immediately after samples are taken for culture if infection is suspected.
The prognosis for uncomplicated ruptured urinary bladders is usually good (>80% survival), provided the animal is stabilized before anesthesia. The presence of concurrent septicemia carries with it a considerably poorer prognosis.395 In one retrospective study among foals with uroperitoneum, 100% of those foals with a negative sepsis score lived and only 57% of foals with a positive septic score survived.396
Gas or Fluid Accumulation in the Gastrointestinai Tract: Ileus
Abdominal distention and colic secondary to excessive gas and/ or fluid accumulation in all or a portion of the gastrointestinal tract are common complications in the compromised neonate undergoing intensive care. The exact mechanisms responsible for the presumably altered GI motility are not well defined. Ileus is associated with the absence of intestinal sounds, abdominal distention, and intolerance of oral feeds characterized by gastric reflux. Auscultation of reduced gastrointestinal borborygmi does not always correlate with the degree of intestinal compromise and decreased motility. Transabdominal ultrasonography helps identify absence of intestinal motility and the location and degree of intestinal distention. Ileus and the attending abdominal distention can cause severe colic and can induce respiratory distress in a weak or premature foal with preexisting pulmonary compromise.
Metabolic and infectious causes of ileus in the foal include hypokalemia, hypocalcemia, hypoxic-ischemic bowel injury, bowel obstruction, peritonitis, enterocolitis, and endotoxemia. Hypokalemia is associated with anorexia, diarrhea, and renal loss. Hypocalcemia is associated with prematurity, decreased dietary intake, excessive bicarbonate administration, diuretic therapy, and those conditions such as asphyxia, toxemia, and sepsis that stimulate release of cortisol and catecholamines. Peripartum hypoxia results in a preferential decrease in blood flow to the gut and kidneys. Poor perfusion of the intestines leads to varying degrees of mucosal damage and decreased motility. Severely damaged bowel requires a period of gut rest to allow healing to occur before restarting oral feeds. Premature resumption of enteral feeding is associated with colic, maldigestion, diarrhea (often bloody), and translocation of intraluminal bacteria across damaged bowel wall into the bloodstream. Some of the more common causes of bowel distention in the neonate include meconium retention, intussusception, ascarid impaction, and small intestinal volvulus. Peritonitis may be associated with intraabdominal abscessation, severe enteritis or gastroduodenal ulcer disease, and generalized septicemia. The most common causes of enteritis in foals include rotavirus, Clostridia sp., Salmonella sp., and dietary changes. Endotoxemia is usually part of generalized septicemia. Chronic bowel distention, regardless of the cause, further impedes return of normal gut motility. In the foal, aerophagia, particularly in the struggling or hypoxic neonate, often results in gas distention that is not easily removed through a nasogastric tube, since gas tends to move quickly through the GI tract. Abdominal distention is also commonly observed during mechanical ventilation in the foal and as a result of overfeeding in the calf. Foals with botulism are often intolerant of enteral feeding, probably because of altered gastrointestinal motility. Use of certain milk replacers can result in bloat, colic, and diarrhea, even in the apparently healthy orphan neonate. Discontinuation of or a decrease in the amount of enteral feeding and, if possible, increased activity of the patient usually results in resolution of the problem.
Abdominal radiographs reveal gas-distended loops of small or large intestine and may identify bowel obstruction. Sonographic examination permits evaluation of bowel wall thickness, peritoneal fluid volume and echogenicity, gut patency, intramural gas accumulation, location and degree of intestinal distention, and presence or absence of motility. An abdominal sonogram should be performed to rule out the presence of an intussusception or other obstructive lesion before initiating any prokinetic therapy.
Management of ileus includes nasogastric decompression, cessation or reduced volume and frequency of enteral feeds if gastric reflux is present, parenteral alimentation if enteral feeding cannot be maintained at a rate of at least 10% of BW/day, enema administration to relieve distal meconium or fecal retention, correction of any underlying electrolyte abnormalities, exercise for ambulatory foals, and judicious use of prokinetic agents. The gut atrophies without enteral feeding. Prokinetic drugs should not be used when bowel obstruction or compromised bowel integrity is suspected. Prokinetic agents that have been used include metoclopramide, bethanechol, and erythromycin. There have been anecdotal reports of small intestinal intussusception after prokinetic use in neonatal foals.
Necrotizing Enterocolitis
Necrotizing enterocolitis (NEC) is a syndrome of acute intestinal necrosis that has been described in human infants and other species, including equine neonates.397 The causes of NEC are not well defined, but predisposing factors include ischemic or hypoxic gut injury, the presence of intraluminal bacteria, and enteral feeding. Following gastrointestinal ischemia, mucosal cell metabolism diminishes and the protective mucous layer is lost. This allows enzymes to break down the mucosal barrier, and intraluminal bacteria can then invade and multiply within the bowel wall. Enteral feeding provides substrate for the bacteria. Abdominal signs include progressive abdominal distention, colic, ileus, and ascites. The condition may appear as a fulminant, rapidly progressive disease or progress at a much slower pace.227
Clinical signs associated with gut injury include ileus, gastric reflux, colic, lethargy, abdominal distention, and diarrhea. Reflux and feces may be positive for blood. Generalized sepsis often accompanies NEC. NEC should be distinguished from intestinal ileus secondary to other neonatal diseases, other surgical GI lesions, bacterial or viral enterocolitis, and intolerance to a milk diet. Ultrasonography may reveal intramural gas accumulation (Fig. 17.17). If intestinal perforation has occurred, pneumoperitoneum and septic peritonitis may also be noted., Intestinal perforation is associated with a hopeless prognosis.
Hemoperitoneum
Hemoperitoneum is a relatively uncommon cause of abdominal distention in the large animal neonate. The most common structures responsible for the hemorrhage are the umbilical vessels and rupture of the liver or spleen secondary to trauma. Occasionally, other structures, such as a ruptured granulosa cell tumor, may bleed.290 Depending on the cause and severity of the hemorrhage, clinical signs relating to hypovolemia and anemia may be mild or severe and appear shortly after birth or in the older foal. Diagnosis of hemoperitoneum is based on the retrieval of free-flowing blood on peritoneal tap and the detection of free fluid in the abdomen. Ultrasound examination may be of benefit in detecting the source of the bleeding. Of critical importance, regardless of the source of the hemorrhage, is prevention of hypovolemic shock, and intensive patient monitoring and intervention is often indicated. Whole blood replacement may be necessary. If an internally bleeding animal with an unstable cardiovascular system is rushed to surgery
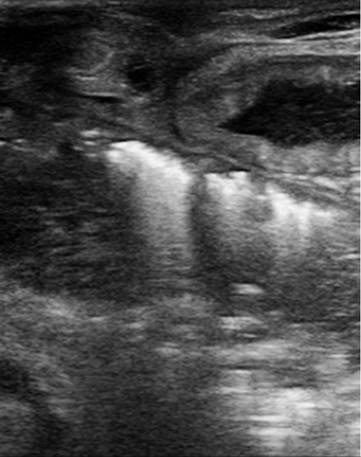
FIG. 17.17 An ultrasound image demonstrating gas in the intestinal wall of a foal with necrotizing enterocolitis.
without prior stabilization, profound shock may occur and a poor outcome usually results.
Umbilical Problems
The umbilicus contains a single umbilical vein, two umbilical arteries, the urachus, and vitelline vein remnant.398 Guidelines for routine care of the umbilicus after birth are discussed in Chapter 16. The most common postnatal problem of the umbilicus is patency of the urachus. The urachus is the anatomic connection between the bladder and allantoic sac. During gestation the predominant flow of urine is through the urachus, but as gestation proceeds some urine will enter amniotic sac via the urethra. The urachus is closed at the time that the cord is broken. Excessive coiling of the umbilical cord during gestation may result in partial obstruction of the urachus with overdistention of the structure, thereby interfering with the normal process of involution when the cord is torn after birth. This is estimated to occur in around 6% of normal foals.399 The structure may fail to close or reopen for a number of reasons, including cutting of the cord rather than tearing, infection, excessive handling, or weakness of the supporting abdominal musculature. The condition is a common complication in sick neonatal foals, particularly those that are mostly recumbent. Affected foals will typically dribble or stream urine from the umbilicus during urination. There may be excessive straining observed. Physical examination may reveal a moist umbilical stump. In a small number of foals a rent in the urachus occurs as it moves through the subcutaneous tissues, resulting in local swelling, that may be marked. If the tear in the urachus occurs intraabdominally, there will be uroperitoneum and in rare cases omentum may herniate externally through the urachal tear. Ultrasound is recommended, and a fluid-filled urachus is consistent with patency. The umbilical arteries and vein should be assessed for infection as an open urachus is a common finding in foals with umbilical remnant infections.400
Therapy for an uncomplicated patent urachus typically consists of conservative management, involving monitoring and frequent disinfection. Cauterization of the urachus using silver nitrate sticks or injection with procaine penicillin was once popular but appears to be used infrequently in recent times. Resection of the structure may be indicated if patency persists beyond 3 weeks of age.
When the umbilicus is enlarged and draining purulent material, infection is easily diagnosed. Many neonates may have a completely normal-appearing external umbilicus but have internal infection of the urachus, umbilical arteries, or vein. Ultrasound is the key tool to diagnose internal abnormalities of the umbilical structures. The umbilical area of neonates younger than 20 days of age with fever of unknown origin should be scanned, as well as any foal with suspected bone or joint infection. A description of normal US findings is described in Chapter 16.
The traditional approach was to surgically remove abnormal umbilical remnants if there were abnormalities detected on US or if the external umbilicus was enlarged and/or draining purulent material. The basis for this was to remove the potential for bacteremia with seeding of other structures, such as bone or joints. There is morbidity and cost associated with simple surgical removal, and there is little evidence that surgical excision is superior to long-term therapy with antimicrobial drugs. More recently, many clinicians favor long-term antimicrobial treatment with oral therapy, such as trimethoprim-sulfa combinations or minocycline. In this approach it is important to monitor responses to therapy using frequent US examinations. Surgical removal would be indicated if the internal appearance worsens in the face of medical treatment.