Respiration
Guy D. Lester
The transition from the fluid-filled lung of the fetus to an organ that is responsible for efficient gas exchange is both rapid and complicated. The process can be complicated by a number of factors, including prematurity or dysmaturity; aspiration of meconium or milk; and bacterial, viral, or fungal infection.
A highly compliant chest wall, an inefficient immune system, and failure to derive adequate antibody from colostrum (partial or total failure of passive transfer) are additive factors that predispose the neonate to respiratory problems.The detection of respiratory disease in the newborn foal can be difficult. Thoracic auscultation can be highly misleading. Minute ventilation (frequency ? tidal volume) is increased in the healthy neonate, resulting in easily heard bronchovesicular sounds. There is no need to accentuate breath sounds with rebreathing techniques. During the first few hours after birth, fluid can normally be auscultated throughout both lung fields and within the trachea. End-inspiratory crackles are commonly heard over the dependent lung during and shortly after rising from lateral recumbency. This is presumably due to simple atelectasis. Foals with respiratory disease will frequently have abnormal lung sounds, such as crackles and wheezes, but neonates with even severe pulmonary disease will occasionally have little detectable abnormality during auscultation. Clinical signs that are often associated with pulmonary tract disease in older foals and adult horses are frequently lacking in the sick neonatal foal. Fetal foals develop and mature in a relatively hypoxic environment within the uterus and therefore are more likely to tolerate postnatal hypoxemia than older foals or adults. Cough is also uncommon, likely due to a postnatal delay in maturation of irritant receptors within airways and delayed onset of the laryngopharyngeal cough reflex.
This is clinically relevant in that aspiration of milk into the lower airway associated with force feeding can go undetected for several days. Of additional importance is that the respiratory rate and rhythm frequently do not accurately reflect arterial concentrations of oxygen or carbon dioxide. This is particularly relevant in foals that are showing signs suggestive of asphyxial injury, where rising arterial CO2 concentrations occur in response to hypoventilation and fail to cause an increase in minute ventilation. In these foals the primary drive for ventilation is arterial O2 rather than CO2.In the absence of arterial blood gas data or radiographic information, the clinician must rely on vague signs, such as restlessness and agitation, increased respiratory rate, or respiratory distress. Historical information may also aid in diagnosis. This should include an estimation of gestational age, recognition of any maternal problems (e.g., fever, dystocia, placentitis, or prepartum vaginal discharge), the presence or absence of meconium staining of amniotic fluid, and an assessment of colostral quality and quantity. Failure to make an early identification of pulmonary disease often results in unfavorable outcome, with chronic pneumonia resulting. Malformations, inflammation, or other abnormalities of the upper respiratory tract can cause clinical signs of respiratory distress, stridor, and dysphagia and result in lower respiratory tract problems as well. A number of nonrespiratory conditions also cause clinical signs that mimic respiratory disease.
The ideal diagnostic tools for investigation of neonatal respiratory disease include arterial blood gas (ABG) analysis and thoracic radiography. ABG analysis is the most sensitive clinical tool used to assess lung function. The sample is usually collected from the dorsal metatarsal artery, easily palpated in most foals on the lateral aspect of the third metatarsal bone. Alternative sites include the brachial artery, located at the level of the medial collateral ligament of the elbow joint, or the carotid artery, but hematoma formation is a common sequel to aspiration from this latter site.
The sample will remain useful for up to 90 minutes in a capped plastic syringe at room temperature.Interpretation of the ABG sample involves consideration of the amount of struggling and position of the foal during sample collection. Normal arterial blood gas values for neonates of different postnatal and gestational ages are presented in Table 17.4. Lateral recumbency can reduce the PaO2 by as much as 30 mm Hg. The sample needs to be handled appropriately, paying strict attention to avoidance of air contamination, which will artificially increase the PaO2 and decrease PaCO2. The inspired oxygen concentration must also be considered when analyzing ABG values. With supplemental oxygen, PaO2 is increased variably, depending on the inspired oxygen concentration (FIO2), the amount of pathology present (particularly the extent of right-to-left shunting), the respiratory rate and tidal volume of the foal, and if the oxygen is delivered by nasal insufflation. A flow rate of 10 L/min, delivered by nasal insufflation, increased the PaO2 to 298 ± 69 mm Hg in the normal, term newborn foal,331 roughly equivalent to an FIO2 of 1.0.337 In the induced premature foal, the PaO2 increased only to 111 ± 35 mm Hg.331 If the respiratory rate of a foal is rapid and shallow, the supplemental oxygen will be diluted by room air because of the large quantity of room air entering the upper respiratory tract, and the concentration of alveolar oxygen will probably be much less than 100%. The two most common respiratory-derived ABG derangements include hypoxemia with normocapnia or hypocapnia or hypoxemia with hypercapnia. It is important to distinguish acute from chronic hypercapnia. Acute hypercapnia is associated with a more substantial drop in blood pH and may lead to circulatory collapse and coma, particularly if accompanied by acute hypoxemia. Chronic exposure to elevated CO2 permits adaptation and more subtle clinical effects.
The change in pH is less dramatic primarily because of enhanced bicarbonate reabsorption in the proximal tubules of the kidney. This effect begins within 6 to 12 hours of exposure to increased concentrations of CO2 and is maximal by 3 to 4 days. Hypercapnia can be exacerbated by fever or the administration of carbohydrates or bicarbonate. The latter is often clinically relevant and highlights the danger of giving large amounts of sodium bicarbonate to foals with pulmonary disease.Interpretation of blood gas values of venous blood (Table 17.4) can be deceptive and should be restricted to evaluation of metabolic conditions (e.g., metabolic acidosis) and not pulmonary gas exchange. To avoid problems associated with regional blood sampling, peripheral venous blood should be taken from a free-flowing jugular vein because the metabolic status of the head is usually stable. To obtain a sample representative of the whole body, mixed venous blood is drawn from the right atrium. Determination of mixed venous blood oxygen saturation is a good test for assessing the overall adequacy of oxygen delivery to tissues because it reflects the balance between oxygen delivery and oxygen use.
Several factors need to be considered when evaluating foal thoracic films. Thoracic radiographs are routinely taken only in the standing or recumbent lateral position in foals, with dorsoventral positioning reserved for the anesthetized or depressed foal. In healthy foals, radiographs taken before 4 hours of age will reveal increased opacity associated with retention of fetal fluids.338 Thus interpretation can be limited because of positioning limitations. If the neonate has been in lateral recumbency for extended periods of time, atelectasis may result in diffuse or localized interstitial infiltrates that usually resolve once lung reexpansion occurs. It can be difficult to accurately distinguish bacterial pneumonia from atelectasis and pulmonary edema on the basis of radiographic appearance alone.
In these cases additional diagnostic aids (cultures, hematology, necropsy) should be used in conjunction with radiology to reach an accurate diagnosis. A false overinterpretation of disease is common due to motion artifact, caused by a combination of long exposure times, poor patient compliance, and high spontaneous ventilation rates. When the radiographic appearance of the lung fields is evaluated, the type of infiltrate (interstitial, nodular, alveolar, mixed); severity; and location (diffuse, perihilar, cranioventral, craniodorsal, caudodorsal, caudoventral) should be noted. Other soft tissue structures (including the heart, vessels, and diaphragm) and bones (ribs, vertebrae, long bones) should also be evaluated.Serial thoracic radiographs are useful in monitoring the progress of a respiratory condition. Radiographic changes may either follow or precede changes in clinical condition, and major changes can occur surprisingly rapidly (Fig. 17.12). Clinical signs of pneumonia frequently resolve much earlier than chest radiographs, and hemograms return to normal. Unfortunately, both ABG analysis and radiography are difficult to perform in field situations.
A study of healthy, sedated neonatal foals compared plain radiography with computed tomography (CT) concluded that CT studies were less subjective and had superior interobserver agreement than plain radiography.339
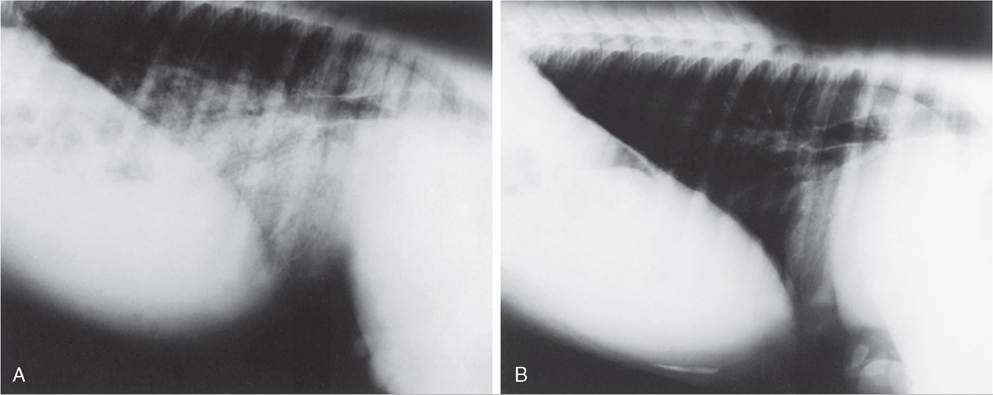
FIG. 17.12 Thoracic radiographs. A, Standing lateral thoracic radiograph of a 7-day-old Thoroughbred foal that experienced an acute onset of respiratory distress and cyanosis. Intubation and oxygen administration raised the PaO2 to only 48 mm Hg. Severe pulmonary interstitial pattern is present in the caudoventral lung fields, and the tentative diagnosis was bacterial pneumonia. With no change in antimicrobial therapy, the foal improved clinically.
B, Radiographs taken 3 days later revealed marked resolution of the pattern.
Ultrasonographic evaluation of the foal's thorax can yield useful information in a variety of disease processes, including pleural effusion, such as hemothorax or pleuritis, bronchopneumonia, or abscessation. It is also the preferred method for diagnosing rib fracture or dislocation, congenital heart disease, and thus is often a useful technique to differentiate cardiac and pulmonary causes of hypoxemia.
Specific Respiratory Conditions
Upper Respiratory Tract Disorders
Upper respiratory tract disorders are relatively uncommon in neonates. Conditions affecting pharyngeal and laryngeal function are important, as they predispose to aspiration pneumonia. Dyspneic neonates also have difficulty nursing and are subsequently likely to become malnourished. Congenital defects of the upper respiratory tract include collapsed trachea, stenotic nares, choanal atresia, epiglottal cyst, and guttural pouch tympany. There have also been reports of pharyngeal dysfunction as a cause of acute dyspnea, stridor, and dysphagia in neonatal foals. ’ ’ Endoscopic examination of the upper airways of these foals reveals a variety of abnormalities that include a flaccid, collapsed, and inflamed nasopharynx; intermittent or persistent dorsal displacement of the soft palate; or arytenoid paralysis (Fig. 17.13). Medical management with antiinflammatory drugs, enteral feeding via nasogastric tube, and broad-spectrum antibiotics (for any coexisting aspiration pneumonia) can result in permanent resolution of the problems within 1 to 14 days (mean of 5.5 days).231 The underlying basis of the condition is not known but may be related to birth asphyxia.
Impaired pharyngeal and laryngeal function may result from physical deformation or neuromuscular disorders. Pharyngeal and laryngeal injuries are often associated with improper application or use of damaged feeding tubes and oral medication equipment. Compression of the larynx by a retropharyngeal abscess or mass tends to cause inspiratory dyspnea, and aspiration pneumonia is a common sequela. Partial occlusion of the upper airway induces turbulent airflow and subsequently mucosal edema. Placement of a tracheostomy tube provides an alternate, sometimes life-saving, airway and rests the inflamed mucosa.
Nutritional myodegeneration, hyperkalemic periodic paralysis, and botulism may induce laryngeal paresis. Dysphagia and subsequent aspiration pneumonia is a common sequela of pharyngeal and laryngeal dysfunction associated with nutritional myodegeneration and botulism. Exercise- and excitement-induced respiratory stridor has been described in foals with hyperkalemic 342
periodic paralysis.342
Collapsed trachea is a rare congenital or acquired condition. It is most commonly reported in American Miniature Horses, although those affected typically develop signs as adults.343 Clinical signs include an intermittent honking cough, stridor, and dyspnea with mild exercise. There is no stenosis of the trachea but rather a dynamic dorsoventral collapse during inspiration. The caudal cervical and cranial thoracic sections of the trachea in the area of the thoracic inlet are most frequently affected. Acquired tracheal collapse is commonly associated with fractured ribs and compression of the trachea at the thoracic inlet by the subsequent bony callus.
Diagnosis of most upper airway disorders can usually be made with a combination of radiography and endoscopy. A 7-mm O.D. endoscope is usually small enough to pass through the ventral meatus of horse and pony foals weighing over 14 kg. An integral part of the diagnostic approach to the neonate with suspected upper airway obstruction is assessment of the lungs for aspiration pneumonia. If the primary upper respiratory problem is not corrected and normal nursing is allowed, the pneumonic process will likely persist and become chronic.
Respiratory Infection
Bacterial infection of the lower respiratory tract most commonly occurs during or shortly after birth, but it can also take place before parturition, through aspiration of contaminated amniotic fluid. This may take place in mares with bacterial placentitis. In the newborn foal pneumonia can result from direct aspiration or inhalation of bacteria or from the hematogenous spread of organisms in foals that are bacteremic. The most common bacterial organisms that have been associated with pulmonary disease in foals are identical to those that cause systemic sepsis. The most common isolates include Escherichia coli, Klebsiella pneumoniae, Pasturella spp., Actinobacillus spp., and Streptococci spp. Less common isolates include, but are not limited to, Salmonella spp., Enterobacter spp., Pseudomonas spp., Serratia marcesans, Staphylococcus spp., and Yersinia pseudotuberculosis.
The diagnosis of pneumonia involves identification of causative organism. Isolation of bacteria can be attempted from blood
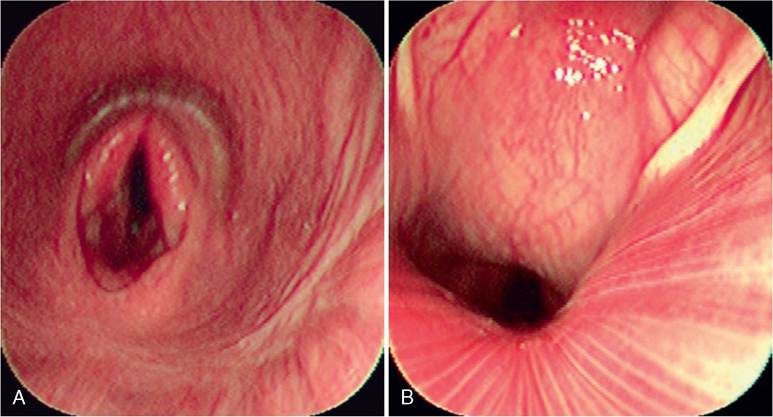
FIG. 17.13 Endoscopic images of a foal with dysphagia and stridor. A, Dorsal displacement of the soft palate. B, Collapse of nasopharynx associated with pharyngeal weakness.
culture or culture of amniotic fluid or placental tissue if in utero infection is suspected. Lower airway culture can be difficult, as a tracheal aspiration can be dangerous in a compromised neonate. An alternative method involves passage of a guarded swab through a nasotracheal tube into the lower airway. A complete blood count and measurement of an acute-phase protein, such as fibrinogen or serum amyloid A, may support a diagnosis of infection but will not be helpful in localization of infection to the respiratory tract. The treatment of bacterial lung disease involves a combination of respiratory support techniques and antibiotic therapy. The neonatal foal readily develops dependent atelectasis in lateral recumbency. Consequently, positioning in sternal rather than lateral recumbency results in improved ventilatory capacity and higher arterial oxygen tension. Broadspectrum antibiotic therapy should be commenced as soon as lung disease is suspected. The third-generation cephalosporins, such as ceftiofur, ceftazidime, ceftriaxone, or cefotaxime, have distinct advantages over aminoglycosides in the treatment of bacterial pneumonia. They have superior penetration into the lung and effective tissue concentrations are easily achieved by intravenous or intramuscular routes. Because premature discontinuation of antibiotic therapy has resulted in relapse in a number of cases, repeat radiographs, and hematology (complete blood cell count and plasma fibrinogen) are highly recommended before discontinuation of antibiotic therapy. A minimum course of therapy of 3 to 4 weeks' duration is not unusual in cases of severe pneumonia.
Several viruses can cause pneumonia in neonatal or young foals. These include equine herpesvirus type 1 (EHV-I) and type 4 (EHV-4), equine influenza, equine viral arteritis virus, and adenovirus.344-347 Neonatal pneumonia due to EHV-1 infection is frequently fatal, even in the face of aggressive supportive therapies such as antiviral medication and mechanical ventilation. Several factors appear common to EHV-1 infected foals, but none should be considered pathognomonic. These include leukopenia with neutropenia and lymphopenia, depletion of the myeloid cell lines on cytologic examination of bone marrow aspirates, and the presence of dilated retinal vessels and a red discoloration to the optic disc on fundic examination. Fatal bronchointerstitial pneumonia occurred in neonatal foals (aged 2 to 12 days) infected with equine influenza virus during the 2007 influenza outbreak in Australia.345,347 Infection with adenovirus can be a problem in any immunocompromised foal, especially Arabian foals with severe combined immunodeficiency (SCID) syndrome.
In utero infection with Histoplasma capsulatum can result in placentitis, abortion, or birth of an infected foal with multiple organ disease, including granulomatous pneumonia.348 An antemortem diagnosis can be difficult to establish but is aided by airway cytology where characteristic yeastlike organisms (3 to 5 μm in diameter) are seen within macrophages. Infection with Candida species (especially Candida albicans) is an infrequent complication in foals with chronic bacterial infection. Lengthy antimicrobial use is an apparent risk factor for infection, and many cases begin with oral candidiasis. The diagnosis is based on a history that often includes persistent low-grade fever, worsening respiratory disease or the development of synovitis, and isolation of the organism through blood culture. Successful treatment of neonatal candidiasis has been achieved with ketoconazole, amphotericin B, or fluconazole.
Meconium Aspiration Syndrome
In utero asphyxia or umbilical cord occlusion can result in fetal passage of meconium into amniotic fluid. Hypoxia induces a redistribution of blood flow away from the GIT, resulting in mesenteric vasoconstriction and secondary intestinal ischemia. Transient hyperperistalsis and anal sphincter relaxation occur thereby allowing passage of meconium. Meconium aspiration may occur before, during, or immediately after delivery as a result of fetal breathing or gasping. Meconium can produce a variety of clinical signs including mechanical airway obstruction and regional air trapping, chemical pneumonitis and alveolitis, alveolar edema, and displacement of surfactant.349 This reduces lung compliance and causes small airway obstruction and focal atelectasis. These events lead to increased pulmonary vascular and airway resistance and ventilation/ perfusion mismatching. Meconium may also enhance the growth of bacterial species within the respiratory tract resulting in secondary bacterial pneumonia. It can be difficult to differentiate meconium aspiration from bacterial pneumonia, especially if the birth was unattended.
If meconium has been aspirated into the pharynx, then gentle suctioning of the nasal and oral cavities is recommended. The ideal time to suction the airways is while the animal is still in the birth canal, before it has taken its first breath. If the foal shows signs of meconium aspiration below the vocal cords, nasotracheal intubation and careful, aseptic suctioning are recommended. Intranasal oxygen should be administered during suctioning. ABG analysis dictates what long-term respiratory and metabolic support is necessary. Mild to moderate hypoxemia can be treated with humidified intranasal oxygen (2 to 10 L/min). Severe hypoxemia with accompanying hypercapnia requires positive pressure ventilation and is associated within increased mortality. If surfactant displacement and secondary atelectasis are contributing to hypoxemia, continuous positive airway pressure (CPAP) alone may improve oxygenation while avoiding any unnecessary increase in peak airway pressure. Exogenous surfactant administration has been advocated to treat the surfactant dysfunction, although efficacy data are lacking. Systemic antibiotic therapy is recommended to prevent secondary bacterial pneumonia. Good airway hygiene and coupage are crucial.
A diagnosis of meconium aspiration is based on a history of meconium-contaminated amniotic fluid and a meconium- stained newborn. Radiographs typically show a ventrocranial distribution of pulmonary infiltrate characteristic of aspiration. Clear, yellow to brown fluid may drip from the nose.
Milk Aspiration
Aspiration of milk into the lower airway may occur as a complication to a wide range of conditions. Most foals that aspirate milk will also demonstrate nasal regurgitation of milk. Unfortunately, the decreased sensitivity of the upper and lower airway to foreign material may make diagnosis of milk aspiration difficult. Aspiration can occur in foals with cleft palate, persistent dorsal displacement of the soft palate (DDSP), botulism, neonatal encephalopathy, or generalized weakness due to sepsis or prematurity. Iatrogenic contamination of the airway can occur when bottle-feeding is forced or if the foal is too weak or sleepy to receive feeding. Substantial and sometimes fatal pneumonia can result from inappropriate placement of nasogastric tube.
The diagnosis of milk aspiration is supported by historical data (nasal regurgitation of milk), physical examination findings (abnormal lung and tracheal sounds), and laboratory data (inflammatory leukogram, elevated fibrinogen and/or serum amyloid A, arterial hypoxemia). Radiographic examination commonly reveals a heavy, perihilar and/or ventrally located interstitial density, with or without air bronchograms.
The treatment of milk aspiration involves long-term, broadspectrum antimicrobial therapy and prevention of further contamination of the airway. The underlying cause must be pursued diagnostically and treated. This may necessitate the use of further diagnostic tests, including endoscopy and plain and contrast radiography. Enteral feeding through a nasogastric or esophagostomy tube is indicated until the underlying problem has been resolved. Nasopharyngeal weakness will frequently resolve over time but may take weeks.
Pneumothorax, Hemothorax, or Uroperitoneum
Pneumothorax is usually an iatrogenic sequel of positive pressure ventilation of diseased lungs, but it may occur spontaneously as a result of birth trauma and rib fracture or from ruptured bullae within the lung parenchyma.350,351 During mechanical ventilation, uneven alveolar ventilation leads to alveolar rupture and dissection of air into the interstitium. The air moves along bronchioles and other lung structures to pleural surfaces, forming blebs that can rupture into the pleural space. The condition should be strongly suspected if the respiratory condition suddenly worsens while an animal is being ventilated. Clinical signs may include respiratory distress, cyanosis, hypotension, or subcutaneous emphysema. Although auscultation may reveal decreased breath sounds, it may be misleading because of the wide referral of breath sounds in foals. Radiographs are indicated to confirm the diagnosis, but, if radiology is unavailable or the animal is very distressed, a direct needle aspirate is both diagnostic and therapeutic.
Pneumothorax may be treated conservatively if no distress is associated with the air leak and the condition appears stable. Thoracic tube insertion is indicated with continuing air leak, if underlying pulmonary disease is causing respiratory distress, and in those patients receiving mechanical ventilation. A trocar catheter is sterilely introduced into the chest cavity, and the catheter is secured using a Chinese Finger Trap suture tech- nique.352 Suction is applied at -15 cm H2O until the tube has drained no air for 12 hours. The tube may then be placed under water seal for an additional 24 hours, and, if no air accumulates, the tube may be removed.
Hemothorax is occasionally noted in the large animal neonate. It has occurred secondary to unstable fractured ribs, with puncture of the lung parenchyma resulting in hemorrhage into the pleural space. Occasionally, a hemothorax may remain undiagnosed until clinical signs of anemia, hypovolemia, or shock appear in the young animal.
Accumulation of pleural fluid is a relatively common feature of moderate to severe uroperitoneum.353 The fluid may result from increased hydrostatic pressure from uroperitoneum- induced compression of the caudal vena cava or urine migration from the peritoneal cavity to the pleural cavity through lymphat- ics.353,354 In most foals the thoracic fluid is not recognized, but some foals develop tachypnea, tachycardia, hypercapnia, and hypoxemia. This signs can be exacerbated after removal of the abdominal fluid, potentially causing a “reexpansion pulmonary edema.”355
Transient Tachypnea in the Neonate
A syndrome observed in Clydesdale, Thoroughbred, and Arabian neonatal foals has been the combination of fever and tachypnea. The condition appears to be more frequent during hot, humid weather conditions. The pathogenesis of the condition is unknown, but it is speculated that it results from a transient problem in central or peripheral control of thermoregulation and/or respiratory rate and pattern. There is a syndrome in human infants termed transient tachypnea of the newborn (TTN) that is self-limiting and, in contrast to the foal syndrome, is generally attributed to failure to adequately clear the lungs of perinatal fluid after birth.356
Affected foals are usually of normal gestation and experience a normal birth. Most display normal activity for a variable period after birth, with a sudden onset of clinical signs. There are usually no signs of pulmonary abnormalities as assessed by thoracic radiographs or ABG analysis. Body temperature is variable between foals, ranging from 102° F to 108° F (39° C to 42.2° C). A poor response to antipyretics has been noted. The respiratory rate and breathing pattern often resemble panting (respiratory rate >80 beats/min). The condition usually resolves spontaneously within a few days to weeks.
Before transient tachypnea is diagnosed, it is important to rule out a pneumonic process or other pulmonary abnormality, other sources of infection, metabolic acidosis, and other causes of an increased respiratory rate. Hematology, lung radiographs, and ABGs should be within normal limits, and bacterial cultures should be negative.
Treatment is directed at controlling the body temperature; body clipping, alcohol baths, and being in a cool environment are the most effective methods. If infection cannot be entirely ruled out, antibiotic therapy should be used.
Treatment of Respiratory Distress
Oxygen therapy is an important component in the management of respiratory distress. The decision to institute oxygen therapy is ideally based on both clinical signs and blood gas analysis. Increased respiratory rate, labored respiration, increased intercostal and abdominal muscle activity, and restlessness are considered indications for a trial of oxygen therapy. A PaO2 less than 55 to 60 mm Hg in lateral recumbency is considered an objective indication for oxygen therapy. If blood gas analysis is not available, clinical signs indicating a favorable response to oxygen therapy include a decrease in effort of breathing, decrease in respiratory rate, and a more comfortable appearing foal. An absence of response may indicate a nonrespiratory origin of the clinical signs, severe lung pathology, a cardiac malformation, or inadequate inspired oxygen concentration.
The inspired oxygen concentration is most easily increased by nasal insufflation using a bias flow of humidified oxygen. Depending on the severity of disease and size of the individual, oxygen is initially delivered at a flow rate of about 5 L/min and the response is noted. The oxygen catheter tip should be advanced into the nasopharynx, and the opposite end should be secured to the nostril using tape or sutures. The actual oxygen concentration delivered to the alveoli depends on several factors, including the position of the tube and the depth and rate of breathing. Oxygen therapy should be directed at maintaining a PaO2 of 80 to 100 mm Hg, and the flow rate should be adjusted according to blood gas results. Oxygen therapy should be on a continuous basis, and weaning from support should be done gradually. Transtracheal oxygen delivery may be beneficial in larger foals; hypoxemic neonatal foals that have a rapid, shallow breathing pattern; or foals with severe pulmonary disease that are unresponsive to nasal insuf- flation.357 A percutaneous catheter system is placed using local anesthetic and secured to the skin. The distal location of the catheter bypasses a substantial volume of dead space and results in a higher alveolar oxygen concentration.
Oxygen therapy is not effective in correcting hypoventilation, and, if hypercapnia is progressive and accompanied by signs of increasing respiratory distress, some type of mechanical ventilatory support is usually indicated. This decision to provide mechanical ventilation must take into account several considerations, including the worth of the individual, the commitment of the owners, the facility and availability of personnel, and the type of disease process present. For additional information on mechanical ventilation the reader is directed to other reviews.358
Regardless of the level of respiratory support provided, the importance of meticulous respiratory supportive technique cannot be overemphasized. Maintenance in sternal position, frequent turning from side to side, regular coupage, and use of proper suction technique are all important components of respiratory support.