Diseases of the Pharynx, Larynx, and Trachea
Amelia R. Woolums
Pharyngeal Trauma, Abscesses, Cellulitis, and Granulomas
■ Definition and Etiology Pharyngeal trauma may result in hematomas, foreign body granulomas, cellulitis, or abscesses.
Trauma usually results from careless use of balling guns, dose syringes, paste-type anthelmintics or calcium preparations, specula, and stomach tubes. Rough, stemmy feeds (especially when chopped), grass awns, briars, and foreign objects (e.g., nails, baling wire) may also cause punctures. Migrating foreign objects or medications (e.g., mineral oil, anthelmintics) may cause pharyngeal granulomas. Hematomas and puncture wounds often result in abscess formation. Diffuse cellulitis may also result. Common bacteria involved include Arcanobacterium pyogenes, Actinobacillus spp., Pasteurella spp., Bordetella spp., Fusobacterium necrophorum, and Streptococcus spp. In cases of particularly virulent bacterial invasion, the condition can become rapidly fatal. C. pseudotuberculosis (caseous lymphadenitis) may localize in the pharyngeal nodes of sheep and especially goats. Caseous lymphadenitis is discussed later in this chapter and also in relation to the hemolymphatic system in Chapter 37.■ Clinical Signs and Differential Diagnosis Signs of pharyngeal trauma vary with the severity of the resulting reaction (e.g., peracute cellulitis versus chronic abscess or granuloma). Prominent signs include inspiratory dyspnea with stertorous inspiratory sounds and a prolonged inspiratory phase; extended head and neck; ptyalism, which is often profuse; quidding; evident pain on swallowing or reluctance to swallow solid feed but willingness to drink liquids; prolonged chewing of boluses; regurgitation of food or saliva through the nostrils caused by pharyngeal paresis; mucopurulent to bloody nasal discharge and fetid odors, usually bilateral; cough; bloat; and visible or palpable swelling in the pharyngeal area.
Megaesophagus has been reported subsequent to pharyngeal trauma. Palpation of the pharynx may increase the stertor and cause pain. In severe cases, systemic signs of fever, anorexia, depression, dehydration, and forestomach stasis may be present. Aspiration pneumonia may be a secondary complication.Differential diagnoses include pharyngeal tumors; lymphosarcoma; sialoliths; rabies; botulism; actinobacillosis; necrotic laryngitis; laryngeal abscesses, trauma, edema, or paralysis; and laryngeal tumors.
■ Diagnosis A thorough manual examination of the oropharynx or a visual examination with an adequate speculum and light source usually confirms the diagnosis of a pharyngeal swelling and often reveals a puncture that is discharging pus. Cases in which the infection is diffuse can be more difficult to recognize, and endoscopy or radiography can be particularly helpful. Restraining the jaws with a McCallum speculum allows a guarded needle attached to a length of tubing and a syringe to be inserted into the swelling for aspiration of any swelling identified. This helps differentiate localized abscesses from granulomas, hematomas, cellulitis, and tumors; allows culture and sensitivity determinations on abscesses; and may aid in cytologic diagnosis of granulomas or tumors. Radiographs may reveal foreign bodies (Fig. 31.64) or air densities (Fig. 31.65) in the pharyngeal tissues. The CBC usually reflects an inflammatory process, with a neutrophilic leukocytosis and a left shift, or a neutrophil-lymphocyte reversal. Dehydration is frequently evident. If the animal is unable to swallow, large
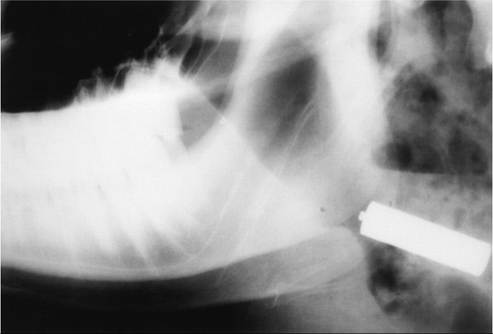
FIG. 31.64 Radiograph of the pharyngeal area of a cow. Note the magnet located in the retropharyngeal tissue.
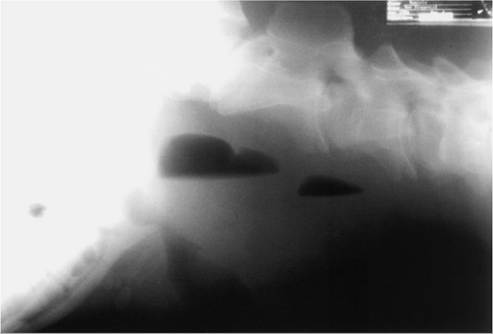
FIG. 31.65 Radiograph of the pharyngeal area of a cow. Note the air densities in the tissue, suggestive of abscess formation.
amounts of bicarbonate may be lost through the saliva, which may lead to evidence of metabolic acidosis on blood gas analysis or serum biochemical profile.
■ Treatment and Prognosis Discrete pharyngeal abscesses are usually best drained into the pharynx. Whenever possible the procedure should be done on the standing animal without sedation to preserve the cough reflex and prevent aspiration. A good oral speculum and excellent restraint are needed. The head should be kept lowered. A guarded blade such as a hook blade from a fetotomy set is introduced into the pharynx, and the abscess is lanced. The cavity is flushed with a mild antiseptic such as 0.2% povidone-iodine in saline solution, again taking care to prevent aspiration. Other options include drainage to the exterior, drainage and flushing with a large-gauge needle and tubing, and extirpation.2 Removal of a bacterial granuloma from the pharynx of a cow via electrocautery has been described.4 Systemic antibiotics are administered in accordance with culture and sensitivity results, or in their absence, procaine penicillin G (22,000 to 44,000 U/kg IM q12-24h) or tetracycline (11 mg/kg IV or SC daily, or 20 mg/kg of long-acting oxytetracycline SC q72h) are used. NSAIDs (flunixin meglumine, 1.1 to 2.2 mg/ kg IV daily or divided twice daily) help relieve pain, swelling, and stertor. In animals with severe, persistent dyspnea, tracheostomy may be necessary. Granulomas and diffuse cellulitis are likewise treated medically with appropriate antimicrobials and antiinflammatory drugs. Supportive therapy such as IV fluids or feeding through a rumenostomy site may be necessary if the animal refuses to eat or drink. The prognosis for most pharyngeal abscesses, hematomas, cellulitis, and granulomas is usually good with appropriate therapy.
Dorsal Displacement of the Soft Palate
Although rare, dorsal displacement of the soft palate has been reported in cattle.30 Respiratory noise is apparent on inspiration and expiration but is loudest on inspiration.
Diagnosis can be made by endoscopic examination. Treatment is similar to that used in horses and can include conservative therapy, which consists of antiinflammatory drug therapy and rest, or the condition can be surgically corrected.Necrotic Laryngitis (Calf Diphtheria, Laryngeal Necrobacillosis) contact ulcers probably provide a damaged mucosal surface, which then allows invasion of the cartilage by F. necrophorum, which is the proximate cause of the lesions. Alternatively, Histophilus somni may be the primary agent inducing a perilaryngeal vasculitis, with F necrophorum representing a secondary bacterial invader.
The disease is most common where cattle are housed in dirty or crowded conditions and in feedlots. Most feedlot cases occur in animals on feed for longer than 30 days. The incidence is sporadic. Cases occur year round, but there appears to be a higher incidence in fall and winter. The disease has a worldwide distribution.
■ Clinical Signs and Differential Diagnosis The problem occurs most commonly in calves from 3 to 18 months of age, up to about 24 months. It is characterized by an acute onset of a moist, painful cough, which the animal may attempt to suppress because of pain. Frequently a severe inspiratory dyspnea with a loud guttural stertor and open-mouth breathing with the head and neck extended are observed. The animal may salivate, make frequent painful swallowing movements, and stand and sip water continually. Signs of systemic disease, including anorexia, depression, fever (as high as 106° F [41.1° C]), and hyperemic mucous membranes, are present. There is often a bilateral nasal discharge and a fetid odor to the breath. The larynx may be visibly or palpably swollen, and palpation may elicit a cough, cause pain, and markedly increase the dyspnea and stertor. If untreated, many calves will die in 2 to 7 days as a result of systemic effects of bacterial toxins and upper airway obstruction. Recovered cases may have a chronic roaring respiration and a harsh, dry cough because of the misshapen larynx.
Aspiration pneumonia and chronic “poor doers” are common sequelae. Differential diagnoses include pharyngeal trauma (abscess, cellulitis), severe viral laryngitis (e.g., IBR), actinobacillosis, and laryngeal edema, abscesses, trauma, paralysis, and tumors.■ Diagnosis The diagnosis is usually made presumptively based on clinical signs alone. A laryngoscopic or endoscopic examination can help confirm the diagnosis, but care must be taken to prevent further stress and respiratory embarrassment. Acute cases show changes in the CBC consistent with any acute septic condition: leukopenia caused by neutropenia with a left shift. In chronic or ongoing cases, leukocytosis with neutrophilia, monocytosis, and hyperfibrinogenemia may be present.
Pathophysiology F. necrophorum normally does not penetrate intact mucous membranes. Laryngeal contact ulcers are thought to provide the portal of entry for F. necrophorum, which is ubiquitous. Laryngeal contact ulcers are also very common in slaughter cattle and are speculated to be caused by the following combination of factors: (1) an acute mucositis from mixed upper respiratory infections; (2) reflex coughing and swallowing, which accelerate the rate of laryngeal closure; and (3) resulting erosion of the swollen membranes over the vocal processes and medial angles of the arytenoid cartilages. Necrotic laryngitis can alter pulmonary function such that the growth rate is impeded and also predisposes to secondary bacterial pneumonia.
■ Necropsy Lesions The lesions are typically located over the vocal processes and medial angles of the arytenoid cartilages. Acute lesions consist of marked edema, hyperemia, and swelling of the mucous membrane around a necrotic ulcer, with accumulated exudate. The lesions spread along the vocal processes and vocal folds and may extend into the cricoarytenoideus dorsalis muscles. In chronic cases the lesions consist of a focus of necrotic cartilage surrounded by purulent exudate, which may be inspissated.
The tract opening may be surrounded by granulation tissue and may drain pus. The arytenoid cartilage may be rotated into the lumen or may contain mucosal cavities lined with thin, hyperemic epithelium.■ Treatment, Prognosis, Prevention, and Control Oxytetracycline (11 mg/kg IV or SC q24h, or 20 mg/kg of long-acting oxytetracycline SC q72h), procaine penicillin G (22,000 to 44,000 U/kg IM q12-24h), or florfenicol (20 mg/ kg IM q48h or 40 mg/kg SC q96h) are appropriate. NSAIDs (flunixin meglumine, 1.1 to 2.2 mg/kg IV once daily or divided twice daily) may reduce swelling, inflammation, and fever. Cases with severe respiratory distress may benefit from one or two doses of steroids (dexamethasone, 0.05 to 0.2 mg/kg IV or IM once or twice), but repeated doses of steroids are not recommended. A tracheostomy may be necessary in severe cases to relieve dyspnea and rest the larynx. Good nursing and supportive care are also important, including shelter, adequate ventilation, easy access to feed and water, and oral or IV fluids if needed. The prognosis is guarded; even when the condition is detected early and treated vigorously, cattle sometimes relapse. When extensive cartilage necrosis occurs, a fatal outcome or chronic ill-thrift is expected. There are no specific control measures. The proposed pathogenesis would suggest that measures to control other respiratory diseases may reduce the incidence of necrotic laryngitis.
Laryngeal Papillomatosis
Papillomas of the larynx have been reported in feedlot cattle. They are caused by a papovavirus, which is thought to enter laryngeal contact ulcers (see the previous Necrotic Laryngitis section). Characteristic signs of laryngeal papillomatosis are stertorous respiration and cough. Differential diagnoses include necrotic laryngitis, pharyngeal trauma, abscess, or granuloma; actinobacillosis; and laryngeal abscesses, trauma, edema, paralysis, and tumors. The lesions are sessile to pedunculated, yellow, frondlike, 1- to 10-mm growths over the vocal processes of the arytenoid cartilages.Treatment usually is not indicated but involves surgical removal. Measures to decrease other respiratory infections and thereby decrease contact ulcers may lower the incidence of papillomas.
Laryngeal Abscesses
The prognosis for recovery is considered guarded unless the condition is detected in the earliest stages and treated vigorously; however, one affected heifer lived for at least 1 year and was bred successfully after permanent surgical tracheostomy for chronic arytenoid abscessation.32
Other Laryngeal Obstructions (Laryngeal Trauma, Edema, Paralysis, and Foreign Objects)
Other laryngeal obstructions are all sporadic and may manifest with similar signs. Trauma to the larynx may result from roping or injury in restraint devices. Inappropriate placement of an endotracheal tube can potentially damage the larynx. The respiratory system is the main target organ for anaphylaxis in ruminants, and laryngeal edema can be a prominent component of this syndrome. Inhalation of smoke or other noxious gases also may cause laryngeal edema. Laryngeal hemiplegia has been reported in association with Sarcocystis species infection of the muscles of the larynx and pharynx in a ram.33 Foreign objects more commonly lodge in the pharynx, but sharp objects and food materials may be aspirated and lodge in the larynx. Signs common to these laryngeal obstructions include inspiratory dyspnea, prolongation of the inspiratory phase, mouth breathing, stertor, cyanosis, salivation, and extension of the head and neck. Palpation of the larynx may reveal swelling and may exaggerate the dyspnea and stertor. Differential diagnoses include necrotic laryngitis, laryngeal abscesses, severe viral laryngitis, actinobacillosis, and tumors. Endoscopy and radiology are required in most cases to differentiate these conditions. Hematologic analysis may give some indication of the presence of bacterial infection; a stress leukogram may also be seen. Tracheostomy is indicated in all severe cases. Surgical correction of laryngeal obstruction by tracheolaryn- gostomy has been described in cattle.34
Laryngeal trauma and paralysis may resolve spontaneously or may require reconstructive surgery. The therapy of anaphylaxis is discussed in the Anaphylaxis section later in this chapter. Foreign objects should be removed surgically or endoscopically. NSAIDs (flunixin meglumine, 1.1 to 2.2 mg/ kg IV daily or divided twice daily) may help reduce swelling, edema, and respiratory embarrassment in all forms of obstruction.
Tracheal Collapse and Stenosis
■ Definition and Etiology Tracheal collapse or stenosis is infrequently reported in cattle and goats.35 The cause is usually unknown, but the problem may result from cranial thoracic trauma, roping, tracheostomies, or possibly congenital defects. In cattle the majority of reports have described tracheal collapse in calves in which signs were usually first evident at several weeks of age. The majority of these cases also involved the thoracic trachea (Fig. 31.66), suggesting a congenital lesion. However, in most calves with tracheal collapse the condition has been a result of dystocia at birth, especially breech presentations, which suggests a traumatic cause. In contrast to reports in cattle, tracheal collapse has been reported in a mature goat that showed no previous signs of respiratory abnormality.36
Tracheal collapse has also been reported in Texel-cross lambs with inherited chondrodysplasia37; affected lambs were normal at birth but developed exercise intolerance as early as 1 week of age. Severely affected lambs developed fatal respiratory compromise when exercised. Tracheal stenosis can also occur in lambs born to ewes that ingest Veratrum californicum root and rhizome material at days 31 through 33 of gestation.38

FIG. 31.66 Radiograph demonstrating collapse of the thoracic trachea in a calf.
■ Clinical Signs and Differential Diagnosis Clinical signs of tracheal collapse may include fever, tachycardia, tachypnea, cyanosis, and mucosal hyperemia with vessel engorgement, but affected animals may have normal vital signs and are otherwise alert and in good condition. Dyspnea is usually induced or exacerbated by excitement or exercise or may be severe at rest. Stertorous respiration is usually evident, is frequently worse on inspiration, and can often be localized to the trachea on auscultation. The inspiratory phase is prolonged, and a “honking” cough is characteristic, especially with intrathoracic collapse. Palpation may reveal or induce the collapse when the cervical trachea is involved. Tracheal palpation or elevation of the head may increase the stertor or induce the honking cough. In some cases there may be other evidence of trauma (fractured ribs, sternebrae), and in some animals pneumonia may be present. There is no response to antibiotics, steroids, or tracheostomy.
Texel-cross lambs with tracheal collapse resulting from inherited chondrodysplasia also exhibited retarded growth, forelimb varus, and reluctance to walk. Severity of signs varied among affected individuals; some died or were euthanized within weeks because of respiratory compromise, whereas others survived to breeding age.37 Animals that survived for several months often developed arthritis characterized by severe erosive lesions of the articular cartilage of major joints, including the shoulder, hip, and stifle. Lambs with congenital tracheal stenosis resulting from maternal ingestion of V. californicum died within 5 minutes of birth after signs of severe respiratory distress.38
Other possible disorders with signs similar to those seen in animals with tracheal collapse or stenosis are tracheal foreign bodies, tracheal actinobacillosis, neoplasms, bronchopneumonia, necrotic laryngitis, and extratracheal compressive lesions (e.g., abscesses, tuberculosis, hematomas).
■ Diagnosis Any deviation of the hemogram from normal is probably a reflection of associated pneumonia or stress. Endoscopy and radiography are the most helpful ancillary aids. Care must be taken when restraining, sedating, and passing the endoscope in these animals; oxygen should be available. In cattle with idiopathic tracheal collapse, radiography and endoscopy usually reveal a dorsoventral flattening, most typically in the caudal cervical and cranial thoracic trachea, although lateral collapse and collapse in other locations (cranial cervical, intrathoracic) are occasionally encountered.
■ Pathophysiology Proposed causes of tracheal collapse in other species include congenital malformations, genetic or nutritionally induced weakness of cartilage, deficient innervation of the trachealis muscles, trauma, ischemic lesions from endotracheal tube cuffs, and primary pulmonary disease. No histologic differences were noted in tracheal rings from collapsed and normal segments when this has been assessed. As previously mentioned, most calves with tracheal collapse have a history of dystocia at birth. During delivery, compression of the chest wall with fracture of the first pair of ribs may cause injury at the thoracic inlet. However, signs of tracheal collapse are not immediately evident at birth but develop over time.
Lambs with tracheal collapse associated with inherited chondrodysplasia had clinical signs most similar to a condition in humans that results from a mutation in the diastrophic dysplasia sulphate transporter gene,39 but the causative mutation in sheep has not yet been reported. Preliminary data indicated that the chondrodysplasia was inherited via a recessive mode of inheritance.37 Tracheal stenosis in lambs born to ewes fed V. californicum was presumed to be caused by cyclopamine, a steroidal alkaloid that is the toxic principle in highest concentration in V californicum. It was notable that lambs developed tracheal stenosis when ewes were fed V. californicum at 31 to 33 days of gestation, whereas craniofacial defects typically recognized in lambs born to exposed dams are seen when the ewe ingests the toxic plant by day 14 of gestation.38
■ Necropsy Lesions At necropsy, affected animals may have either a laterally or dorsally compressed trachea; typically several centimeters of the trachea are affected. Necropsy of sheep with inherited chondrodysplasia reveals a trachea that is flaccid, flattened, and sometimes irregularly kinked. Tracheal rings are markedly thickened, and the lumen is narrow, possibly extremely so. Diffuse pulmonary congestion and edema, with epidcardial ecchymoses, may occur as a result of terminal anoxia and respiratory distress. Other lesions include exaggerated convex curvature of the ribs, anglular limb deformities, and erosive arthritis with exposure of the subchondral bone in one or more joints. Histologically, hyaline cartilage in affected organs is hypercellular and disorganized, with foci of apparent chondrolysis. Chondrocytes are larger than normal, although shrunken, apparently necrotic chondrocytes are also seen. Necropsy of lambs with congenital tracheal stenosis resulting from maternal ingestion of V. californicum reveals pronounced lateral flattening of the trachea. Tracheal rings are reduced in number, with abnormal size and shape and irregular spacing. Histologically, the cartilage rings in affected lambs were flattened and thin and had a thinner zone of proliferating chondrocytes on their outer surface compared with normal age-matched controls.
■ Treatment and Prognosis Mild cases may respond to confinement sufficiently to be fed out for slaughter. A number of surgical treatments have been proposed in other species, including anastomosis, bisection of tracheal rings, internal and external prostheses, and plication of the dorsal membrane. External prostheses have been used successfully in calves,35 adult cattle, and a goat.40 A favorable prognosis for surgical correction is estimated at approximately 30%.23 A detailed description of surgical repair in calves by external prostheses has been published.23 Successful management of lambs with congenital tracheal collapse or stenosis has not been reported, although mildly affected lambs with congenital chondrodysplasia survived into adulthood. Because of the apparent genetic basis for the disease, breeding of affected animals should not be recommended.
Tracheal Foreign Bodies and Masses and salivation. Differential diagnoses should include pharyngeal trauma; necrotic laryngitis; laryngeal abscesses, trauma, edema, or paralysis; tracheal collapse; and extratracheal compressive lesions. Endoscopy and radiology are important aids to diagnosis. Care must be exercised in restraint and in passage of the endoscope. Some small objects may be retrieved by a snare passed through an endoscope; others may require tracheostomy. When possible, the tracheostomy should be performed below the object. The actinomycotic masses are soft, pedunculated lesions with a granular surface containing small yellow foci.
Tracheal Edema Syndrome of Feedlot Cattle
Tracheal edema syndrome has also been referred to as tracheal stenosis in feedlot cattle. In this condition extensive edema and hemorrhage in the dorsal wall of the trachea result in coughing, dyspnea, and stertor, which has given rise to the term honker cattle.42 Tracheal edema syndrome occurs in two forms, characterized by either acute dyspnea or a chronic cough. It is not known whether the two forms are related. Although the syndrome has been recognized for years, no controlled research has been undertaken to determine the cause or risk factors of this syndrome, and the cause is unknown. Theories regarding possible causes include infections with upper respiratory viruses or bacteria such as P. multocida or H. somni, trauma to the trachea from feedbunks, passive congestion and edema from excessive fat accumulation in the thoracic inlet, hypersensitivity reactions, and mycotoxins.
The acute dyspnea syndrome occurs mainly in heavy feedlot cattle in the latter two thirds of the feeding period and is most common in Southern Plains feedlots. It is sporadic and more common in summer, possibly because of exacerbation by hot weather. At one extreme, sudden deaths without the onset of noticeable clinical signs have been reported, and at the other extreme subclinical disease was evidenced by lesions in animals at slaughter that did not have clinical signs. Other factors that increase respirations also may cause signs to appear. Signs include an acute onset of dyspnea and loud guttural inspiratory sounds that can be localized to the lower trachea. Open-mouth breathing, extension of the head and neck, and cyanosis, leading to recumbency and death by asphyxiation, are present. Differential diagnoses for this form include pharyngeal trauma or abscess; necrotic laryngitis; IBR; laryngeal abscess, tumor, foreign object, edema, or paralysis; tracheal foreign object, mass, or collapse; and AIP.
The chronic form occurs in lighter cattle (135 to 400 kg [300 to 900 lb]) and is more common in western plains feedlots. It is also sporadic but less seasonal. Affected animals may have a history of IBR or pneumonia. The main sign is a continuous, frequent, deep, hacking, nonproductive cough. The animal may be unthrifty but is otherwise normal in appearance. The main differential diagnoses are necrotic laryngitis or mild, chronic suppurative pneumonia. Endoscopy and visualization of the lesions subsequently described aid in the diagnosis. Necropsy of the acute form reveals an edematous thickening of the submucosa and mucosa of the dorsal trachea (Color Plate 31.1), as much as 5 cm thick and extending 20 to 30 cm from the midcervical area to the thoracic inlet or tracheal bifurcation. There is also extensive mucosal, submucosal, and peritracheal edema and/or hemorrhage, possibly related at least in part to agonal breathing. There may be no other lesions of the airway or lungs, or abnormalities (e.g., pulmonary edema, bronchitis, interlobular edema and emphysema, alveolar hemorrhage) may be seen. Lesions in the chronic form consist of hyperemia of the mucosa of the caudal third of the trachea, with a thin layer of mucopurulent exudate. The mucosa may have a cobblestone appearance or even large, fiberlike projections and polyps. No effective treatment exists for the chronic form. Corticosteroids (dexamethasone, 0.05 to 0.2 mg/kg IM or IV; prednisolone, 1 to 2.2 mg/kg IM or IV daily) are recommended for the acute form, as are such practices as preventing stress, providing shade, and cooling with water sprays and fans. Opinions are divided regarding the value of antimicrobial therapy. However, because animals with tracheal edema syndrome may be difficult to distinguish clinically from animals with conditions that could respond to antimicrobials (such as necrotic laryngitis), antimicrobials are often administered. Because withdrawal times associated with antimicrobial administration could delay shipment of affected animals to slaughter, drugs with a short withdrawal time should be used if salvage is an option. Tracheostomy may not be helpful if placed proximal to the obstruction, and relief of dyspnea via tracheostomy may require insertion of an endotracheal tube to the tracheal bifurcation. Oxygen administration could be beneficial if available. Recovered patients tend to relapse and should be salvaged.