Diseases of the Sinuses
Gretchen P. Grissett
Sinusitis
■ Definition and Etiology The paranasal sinuses of ruminants consist of the following sinuses: sphenoid, lacrimal, conchal, palatine, frontal, and maxillary.15 The maxillary sinus lies on the upper jawline and contains the roots of the premolar and molar teeth.
The frontal sinus consists of a rostral and caudal compartment, with the caudal being the largest and expanding into the horn core. In sheep and in goats, the frontal sinus consists of a medial and lateral compartment, with the lateral compartment being analogous to cattle's caudal compartment.15 Despite the potential for infection in any sinus, the maxillary and frontal sinuses are the ones of most clinical15
significance.15
Frontal sinusitis most commonly occurs secondary to a dehorning procedure that entered the sinus. Other common causes include traumatic fracture or injury of the horn, horn tipping, bone sequestrum secondary to dehorning, facial fracture,16 or O. ovis infection in sheep (in goats less commonly). Bucking bulls were more likely to present with horn and sinus disorders than nonbucking bulls in one study.17 Maxillary sinusitis most commonly results from an infected tooth root. Other causes of maxillary or frontal sinusitis include extension of actinomycosis or neoplasia, hematogenous extension of respiratory pathogen,18 sinus cysts,19 and lymphosarcoma.20 One study evaluated the paranasal sinus microbial flora of clinically normal cattle and cattle presented for portmortem examination, finding that 83.5% of the study individuals did not contain detectable microbes. The organisms isolated from the paranasal sinuses in this study included bovine respiratory disease pathogens Haemolytica, Trueperella pyogenes, Pasteurella multocida, Bibersteinia trehalosi, and parainfluenza virus type 3 (PIV-3).18
■ Clinical Signs and Differential Diagnosis Acute or chronic sinusitis can result following dehorning.
Generally only one sinus is affected. Clinical signs associated with acute sinusitis include lethargy, inappetence, pyrexia (39.4° to 41.1° C), unilateral or bilateral mucopurulent discharge, head pressing, and head tilt. Typically, purulent discharge and/or foul-smelling crusting is present at the cornual portion of the sinus. With chronic sinusitis, clinical signs can occur weeks to months after dehorning. Chronic frontal sinusitis can also occur unrelated to dehorning. One study found 4 of the 12 individuals presented for chronic frontal sinusitis had horns, had no record of dehorning, or were dehorned as calves without entering the sinus, but 3 of the 4 did have a recent history of respiratory disease.21 Clinical signs potentially associated with chronicity include the aforementioned signs, as well as intermittent or consistent pyrexia, stridor, alterations in airflow (typically unilateral), halitosis, reluctance to move, abnormal posture, extended head and neck, partially closed eyes with tendency to rest the head on stationary objects as a sign of pain, frontal bone distortion, exophthalmos, and intolerance of head manipulation. Neurologic signs may result if extension causes impingement or infection of the central nervous system with possible sequelae, including intracranial abscess and septic meningitis.21Maxillary sinusitis is uncommon. Clinical signs include facial swelling and possible deformation over the affected sinus, unilateral mucopurulent discharge, and occasionally decreased appetite secondary to pain during mastication.16 Maxillary sinusitis is usually associated with a tooth root infection. However, in one report a cow with maxillary sinusitis unassociated with a tooth root fracture or infection was successfully treated. Bacteria cultures were negative, and the etiology was idiopathic.22 Differential diagnoses for sinusitis include facial fractures, actinomycosis, actinobacillosis, retrobulbar abscess, lymphosarcoma, nasal or sinus neoplasia, and sinus cysts.
■ Diagnosis Typically, diagnosis can be reached based on history and clinical signs. Certainly, a history of recent dehorning or chronic nasal discharge (especially unilateral) should create a high suspicion of sinusitis. Percussion of the affected sinus may reveal a dull, full resonance and may be painful to the individual. A hyperresonant sound may occur if gas is present under severely thinned bone. Radiographs reveal fluid in the sinuses and may reveal lysis and/or deviations of bony septa (Fig. 31.62). In cases of maxillary sinusitis, radiography will determine if dental disease is involved. In addition, radiography will diagnose presence of facial fractures, masses, and actinomycosis. Endoscopy can assist with localization and etiology of the clinical signs. In one report endoscopy was used to confirm maxillary sinusitis by visualizing purulent drainage from the ostia of the nasomaxillary opening, as well as visualizing the sinus after sinus trephination to rule out
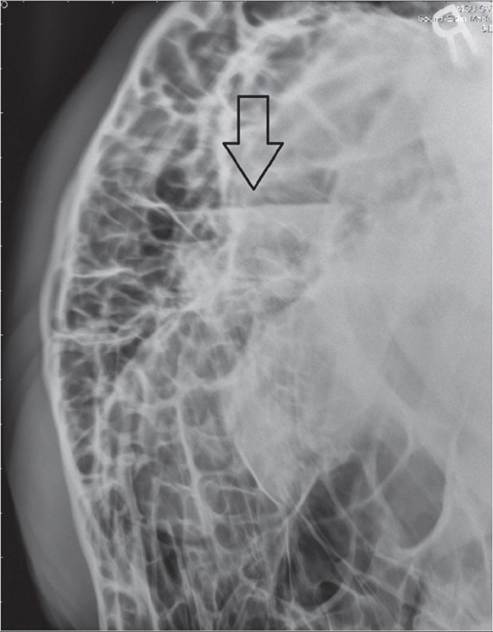
FIG. 31.62 Right lateral radiograph with a horizontal fluid line (arrow) in the right frontal sinus of a mature Brahman bull with sinusitis secondary to horn tipping. (Courtesy Dr Gretchen Grissett, Mississippi State University, Starkville, Miss.)
diagnoses such as sinonasal cyst or neoplasia. CT gives the most precise localization and definition, especially with regard to cysts, masses, and dental disease.23 Sinocentesis can be performed for culture and cytologic examination.19 For sino- centesis, a Steinmann pin is used to create a hole into the sinus to facilitate fluid aspiration.19 A culture and sensitivity of the fluid should be performed to direct antibiotic selection. T pyogenes is isolated most commonly with dehorning-associated sinusitis.21 P. multocida is most commonly isolated in individuals with sinusitis not associated with dehorning.21 However, a multitude of other agents have been reported, including Proteus, Pseudomonas, E.
coli, Moraxella spp., Aerococcus viridans, Bacillus spp., Fusobacterium spp., Prevotella spp., Porphyromonas levii, and Bacteriodes spp.17,21 A CBC and serum biochemical profile is often variable and offers minimal assistance with definitive diagnosis.■ Treatment and Prognosis Establishing drainage and sinus lavage are the treatment goals for sinusitis. For acute sinusitis associated with dehorning, conservative management can be used by thorough cleansing; debridement; removal of sequestered, devitalized bone; and lavage of the cornual wounds. If cornual drainage is inadequate, placement of a 4-mm Steinmann pin into the caudal frontal sinus is another conservative technique for treatment of acute sinusitis.16 After local anesthesia and a stab incision, a hand chuck or drill is used to create the hole into the affected sinus with the Steinmann pin. Polyethylene tubing (Foley catheter, fluid administration set) is used for daily sinus lavage.
For chronic cases, access to the paranasal sinuses is achieved with trephination or bone flap over the affected sinuses.16 Trephination is ideal because it can be performed standing with sedation and local anesthesia under field conditions, whereas a bone flap requires general anesthesia. Unfortunately, a bone flap may be necessary in cases with pyogranulomatous inflammation that would be insufficiently lavaged with trephination alone. In addition, the numerous septa of the frontal sinus and high location of the nasomaxillary opening in the maxillary sinus may necessitate a bone flap to allot adequate access and drainage.15 Sinusotomy locations for trephination include the dorsal frontal sinus, postorbital diverticulum, rostral frontal sinus, turbinate portion of the frontal sinus, and the maxillary sinus (Fig. 31.63).
Frontal sinusotomy sites are based on known anatomic landmarks and modified as needed to accommodate frontal bone distortion and dehorning wounds.21 The individual should be restrained appropriately in a chute and sedated.
The sinusotomy location is 3 to 4 cm from midline intersecting a line drawn between the caudal aspect of the orbits. The proposed site should be surgically prepared and instilled with 2% lidocaine HCl for local anesthesia. A full-thickness circular area of skin large enough to accommodate the trephine (approximately 2 cm in diameter) extending to the periosteum should be excised. A Galt trephine should then be used to remove a section of bone to access the sinus. After entering the sinus, samples should be obtained for culture and cytology. If draining tracts are present, a second sinusotomy can be performed at the cornual portion of the sinus. The postorbital diverticulum is accessed approximately 4 cm caudal to the dorsal rim of the orbit just above the temporal crest of the frontal bone.24,25 The rostral frontal sinus is entered just caudal to a line drawn between the center of the orbits and just off midline, with the turbinate portion of the frontal sinus entered just rostral to this line and to either side of midline. The numerous septae in the frontal sinus can often make drainage difficult, especially with postoribital diverticulum involved, meaning that one trephination can be insufficient. Often two trephination sites are required for an ingress and egress lavage system. For sheep and goats, the frontal sinus is even more compartmentalized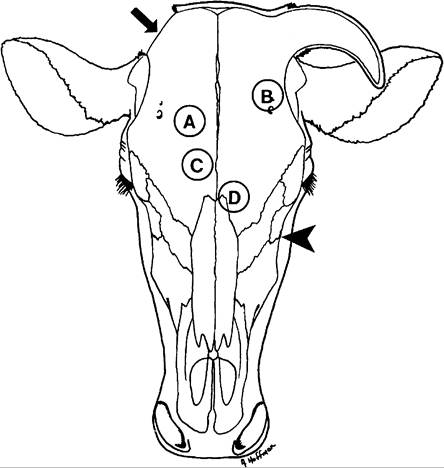
FIG. 31.63 Trephine sites for sinusotomy. A, Dorsal frontal sinus.
B, Postorbital diverticulum. C, Rostral frontal sinus. D, Turbinate portion of frontal sinus. The maxillary sinus is trephined ventral to a line from the infraorbital foramen to the medial canthus (arrowhead). If draining tracts are present at the poll, an additional sinusotomy can be made in the cornual portion of the frontal sinus (arrow).
than cattle, making effective drainage very difficult. In addition, sheep and goats have a thin calvarium, meaning that chronic sinusitis leads to meningitis more easily than in the bovine patient.
Therefore early, aggressive treatment in sheep and goats is essential, including consideration of a bone flap procedure and two trephination sites. Preferred trephination sites are rostral to the horn or medial to the middle of the orbital rim, avoiding risk of injury to the frontal vein.15The maxillary sinus is accessed by drawing a line from the medial canthus to the infraorbital foramen. The trephine is positioned just ventral to this line, lining up just dorsal and caudal to the facial tuberosity.22 If an infected tooth cannot be removed orally, the sinusotomy site should be positioned over the affected tooth to allow axial alignment and repulsion of the tooth.25 In immature animals, the tooth roots are longer and occupy much of the maxillary sinus. Therefore care should be taken and the trephine site should be positioned higher to avoid the tooth roots.16 If a tooth is repelled, a roll of gauze or methyl methacrylate plug should be used to pack the alveolar socket to prevent feed material entering the side. If rolled gauze is used, the gauze can be passed from the socket, into the sinus, and out the trephine hole and secured to the individual's face. The packing should be changed with each lavage. Since the maxillary sinus has fewer septae than the frontal sinus, typically one sinusotomy site is sufficient for drainage and lavage. With chronic maxillary sinusitis, damage to the lacrimal and infraorbital canals and infraorbital nerve is possible.15,23
Drains can be placed in communicating trephination sites to prevent premature closure and facilitate lavage and drainage of the affected sinus. Sinus lavage should occur once to twice daily with saline, dilute povidone-iodine, or dilute chlorhexidine solution. One study evaluated sinus lavage solutions and found that individuals treated with the 5% diluted povidone-iodine solution had better clinical resolution that the individuals lavaged with saline alone.26 A stent bandage can be used to cover the trephination sites to prevent debris and environmental contamination entering the sinus until sufficient granulation has occurred.16 Parenteral antibiotics and NSAIDs are indicated in individuals with systemic signs. Flunixin meglumine (1.1 mg/ kg IV q24h) is recommended for individuals in the acute phase of the disease course and those that are perioperative. For individuals with chronic sinusitis treatment, meloxicam (0.5 to 1 mg/kg PO q48h) is recommended for protracted treatment. Since sinusitis caused by dehorning is most commonly associated with T. pyogenes, penicillin G procaine (22,000 U/kg IM q12h, or 44,000 U/kg IM q24h) is the empirical antibiotic choice.21 P. multocida is most commonly isolated in frontal sinusitis not associated with dehorning.21 Penicillin may be effective against some P multocida isolates, but oxytetracycline (11 mg/kg IV q24h for 5 days, or 20 mg/kg SC long-acting oxytetracycline q72h) can be administered with nondehorning-related sinusitis. Florfenicol (40 mg/kg SC q96h) is also a reasonable choice, as it has bacteriostatic activity against both T. pyogenes and P. multocida. Antimicrobial therapy should always be modified to culture and sensitivity results when available. Prognosis is good for individuals early in the disease course, usually resolving in 7 to 14 days with appropriate therapy and systemic antibiotics. For chronic cases the prognosis is fair to guarded, with weeks of aggressive therapy required for a successful outcome. Individuals with neurologic signs typically have a grave prognosis, and humane euthanasia should be considered.
■ Prevention and Control The best prevention for frontal sinusitis in ruminants is dehorning as neonates prior to communication of the horn with the frontal sinus. Ideally, dehorning occurs with electrocautery (dehorning iron) or a Barnes dehorner prior to communication with the frontal sinus. For mature cattle, a surgical (cosmetic) dehorn using aseptic technique is recommended. A cosmetic dehorn allows primary skin closure, minimizing environmental contamination and expediting healing time.27 If a surgical dehorn is not performed, avoid dehorning during fly season or windy or rainy conditions to help prevent mydriasis and sinusitis. Disbudding of sheep and goats should occur in the first week of life due to the rapid growth of horns. For mature sheep and goats, cosmetic dehorning can also be performed, minimizing the risk of sinusitis and expediting healing time.28 Without cosmetic dehorning, dehorning of mature sheep and goats requires intensive bandage management and 4 to 6 weeks for healing by second intention.29