Disorders of the Peritoneum in Horses
Tiffany L. Hall
■ Peritonitis in Horses
Anatomy and Physiology
The peritoneum consists of a single layer of mesothelial squamous cells covering the peritoneal cavity and abdominal organs.
These cells rest on a thin basal lamina attached to a layer of loose connective tissue, which allows a variable degree of motion. The peritoneum is coated with a thin serous film that serves to minimize friction and facilitate free movement between abdominal viscera. In males the peritoneum forms a closed sac, whereas in females it communicates with the external environment via the fallopian tubes.The peritoneum is divided into the visceral peritoneum and the parietal peritoneum. The visceral peritoneum, which encloses the intraperitoneal organs and forms the omentum and mesenteries, is supplied by the splanchnic vasculature and is innervated by the visceral autonomic nervous system. The parietal peritoneum lines the abdominal walls, pelvis, and diaphragm and receives its blood supply via branches of the lower intercostal, lumbar, and iliac arteries, which drain via veins into the caudal vena cava. Irritation of the parietal peritoneum gives rise to afferent stimuli that are perceived as somatic pain, which is transmitted by the intercostal and phrenic nerves and may manifest as splinting of the abdomen and a reluctance to move. In contrast, there are no pain receptors in the visceral peritoneum.
Peritoneal fluid is constantly being produced and absorbed through the passive diffusion of fluid and solutes across the semipermeable peritoneum. Transperitoneal fluid movement is increased during peritoneal inflammation and may cause a rapid, massive transudation of fluid into the peritoneal cavity that can lead to hypotension and shock.1
The peritoneal lymphatic channels, particularly the diaphragmatic lymphatic channels, play a major role in the removal of fluid and solutes from the peritoneal cavity, emptying primarily into the thoracic duct and providing the first line of defense against peritoneal contamination.
Cellular defenses are provided by peritoneal macrophages, mast cells, mesothelial cells, and activated peritoneal T cells. Peritoneal macrophages have antimicrobial activity as a result of their complement receptors, phagocytic ability, cellular recruitment, and T-cell-mediated immune responses. Peritoneal mesothelial cells are an abundant source of plasminogen activator, which is responsible for normal fibrinolytic activity on peritoneal surfaces.1■ Pothogenesis Peritonitis is inflammation of the peritoneum that results from a number of infectious and noninfec- tious causes. It is classified as primary or secondary, acute or chronic, and localized or diffuse. Common causes of peritonitis in horses are listed in Box 32.2. Primary peritonitis is uncommon in adult horses but may be diagnosed in foals with sepsis or young horses infected with Streptococcus equi. More commonly,
■ BOX 32.2
Causes of Peritonitis in Horses Gastrointestinal
Intestinal perforation Rectal tear
Intestinal ischemia
Proximal enteritis
Colitis
Intestinal parasites
Intestinal neoplasia Actinobacillus equuli infection
Iatrogenic
Celiotomy Enterocentesis
Chemical irritation (lavage solutions) Colpotomy/castration
Foals
Bladder rupture/uroabdomen Umbilical/urachal infection
Septicemia Necrotizing enterocolitis Rhodococcus equi infection
Extragastrointestinal
Neoplasia of abdominal organs Hemorrhage of abdominal organs Abscessation of abdominal organs
Streptococcus equi Streptococcus Zooepidemicus Corynebacterium pseudotuberculosis
Hepatic disorders Cholelithiasis Hepatitis Liver lobe torsion
Nephritis Pancreatitis Cystitis
Urolithiasis Endometritis Uterine/vaginal tears Scirrhous cord Systemic amyloidosis Viral infection
Influenza
Equine viral arteritis Equine infectious anemia
peritonitis is secondary to translocation of bacteria from the gastrointestinal tract, occurs after urogenital trauma, or results from other inflammatory conditions.
A subset of infectious peritonitis with a unique presentation and associated with Actinobacillus equuli has been described and is discussed at the end of this section.Retrospective studies concluded that a cause of peritonitis is often not identified (as was the case in 50 of 65 horses and in 19 of 55 horses).2,3 In both groups, cases of confirmed gastrointestinal rupture were excluded from analysis, and horses that had undergone abdominal surgery were excluded from one study. The conditions most commonly associated with peritonitis in these studies included recent abdominal surgery (18 of 55), postpartum complications (22 of 120), suspected cyathostomiasis (4 of 65), infiltrative bowel diseases (3 of 65), and internal abscesses (3 of 65).2,3
The local response of the peritoneum to insult is similar regardless of the cause. Initially, peritoneal mast cells and macrophages release histamine and serotonin, which results in vasodilation and increased vascular permeability with transudation of fibrinogen-rich plasma into the peritoneal cavity. The release of TNF-alpha and IL-1 stimulates neutrophil chemotaxis and degranulation, and the inflammatory response is promoted by the release of platelet-activating factor, prostaglandins, and leukotrienes. Damage to mesothelial cells results in release of tissue thromboplastin and decreased levels of plasminogen activator, which are conducive to fibrin formation and deposition.4 Fibrin functions to confine bacteria and seal the peritoneal defect; however, if the immune system fails to clear the bacteria and foreign debris, the inflammation continues, and fibrin production results in abscess and adhesion formation.
■ Clinical Features Clinical signs of peritonitis vary and depend on the cause and duration of the peritonitis. Localized infections often have limited systemic symptoms, whereas diffuse peritonitis can elicit generalized signs of endotoxemia and sepsis. Horses with peracute peritonitis caused by intestinal rupture show signs of acute, severe sepsis and cardiovascular collapse with tachycardia, tachypnea, sweating, varying degrees of abdominal discomfort, and death within hours.
According to two retrospective studies, the most common presenting clinical signs for peritonitis include colic, depression/ lethargy, tachycardia, tachypnea, pyrexia, and altered mucous membrane character.2,3 Much of the clinical presentation in acute colic reflects the degree of systemic inflammation and hypovolemia caused by third spacing. Colic symptoms may be related to inflammation of the parietal peritoneum and are characterized by guarding or splinting of the abdomen and a reluctance to move or defecate.5 Sympathetic stimulation, hemoconcentration, or serosal surface trauma may decrease gastrointestinal motility, leading to ileus, which may result in gastric fluid accumulation and small intestine distention, thereby intensifying the abdominal pain. In addition, gastrointestinal impactions commonly develop as fluid is reabsorbed from the cecum and large colon in an attempt to replace intravascular fluid deficits resulting from extravasation of fluid into the peritoneal cavity. Chronic peritonitis generally manifests with more insidious signs, including lethargy, inappetance, and weight loss.
Rectal examination may identify either roughened peritoneal surfaces or an abnormally empty abdomen in cases of intestinal rupture. The bowel may become distended in association with the presence of adhesions or ileus. Abdominal masses, abscesses, or enlarged mesenteric lymph nodes are occasionally palpable; however, in many cases, no abnormalities are identified on rectal palpation. Animals with a recent history of foaling or castration should undergo urogenital examination to rule out vaginal, cervical, and uterine tears in mares or infected castration sites in males.
■ Diagnosis
ULTRASONOGRAPHY. Ancillary diagnostic testing such as transabdominal and transrectal ultrasonography aid in diagnosis of peritonitis and identification of the source. The clinical utility of ultrasonography greatly depends on the quality of equipment and the experience of the practitioner; identification of abnormalities in cases of peritonitis ranges from 50% to 90%.2,3 The most common finding on transabdominal ultrasonography is an increase in volume or altered echogenicity of peritoneal fluid.
Other findings can include intraabdominal abscesses, lymphadenopathy, or dilation of the small intestine with or without increased intestinal wall thickness. Fibrinous strands or fibrin adhesions may also be identified by ultrasonography (Fig. 32.74) and a site for abdominocentesis selected. Perirectal masses may be observed on transrectal ultrasonography, particularly in cases associated with vaginal tears.Hematologyand BIOCHEMISTRY. Alterations in laboratory values vary widely, depending on the cause and duration of peritonitis. Hematologic abnormalities seen in acute, severe peritonitis include elevated PCV secondary to transudation of fluid into the peritoneal cavity and severe neutropenia in association with endotoxemia and systemic inflammation. Initially, plasma protein levels increase, which reflects the degree of hypovolemia; in chronic cases, however, hypoproteinemia may be present. Peripheral cell counts can exhibit leukopenia or leukocytosis, and a left shift with more than 5% immature neutrophils is observed in approximately 40% of patients.3 Hyperfibrinogenemia is a common finding; fibrogen levels ranged from 490 to 1120 mg/dL in a review of 65 cases.2 Peritonitis of longer duration and internal abscesses may manifest with a normal or increased systemic neutrophil count, monocytosis, and elevated plasma protein levels, fibrinogen levels, or a combination of these.6 In addition, peripheral and peritoneal levels of serum amyloid A may be greatly increased in cases of peritonitis.
Alterations in serum chemistry and blood gas values reflect the patient's cardiovascular status at the time of presentation, in association with the degree of systemic inflammation. Prerenal azotemia, hypokalemia, hyponatremia, and hypochloremia may be present, as may acidosis and an increase in unmeasured anions, such as lactate, as the patient's condition declines. Other
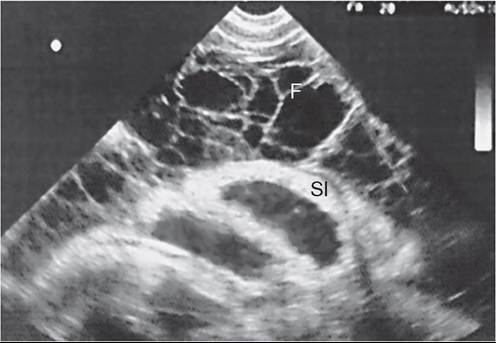
FIG.
32.74 Abdominal ultrasound image in an adult horse with chronic peritonitis, showing web of fibrin (F) surrounding anechoic fluid. The small intestinal wall (SI) is thickened. (Courtesy Dr. David Schmitz, Texas A&M University.)changes in serum chemistry values could indicate an underlying condition in a specific organ system.
AbdominocentESIS. Peritoneal fluid analysis confirms the diagnosis of peritonitis, although the cause may remain unknown. Expected values for peritoneal fluid in normal horses, as well as in horses that have undergone abdominal exploratory surgery and castration and in postpartum mares, are listed in Table 32.9.7-10 The cytologic appearance of the leukocytes and mesothelial cells should be normal, although activated mesothelial cells with vacuolation are not an unusual observation in normal horses.
Evaluation of fluid character and quantity can aid in developing and prioritizing a differential list. Turbid, cloudy fluid indicates an increased cell count. Serosanguineous fluid indicates an increase in erythrocytes or free hemoglobin that may be caused by intestinal degeneration with transmural erythrocyte leakage, splenic puncture during abdominocentesis, abdominal viscera laceration, or skin contamination. Green fluid results from enterocentesis or intestinal rupture, and brown fluid is associated with late-stage tissue necrosis. The quantity of fluid varies among horses and can be increased in acute, diffuse peritonitis, or fluid may be absent in low-grade and localized peritonitis. The presence of large quantities of dilute, colorless fluid should alert the clinician to the possibility of ascites or uroperitoneum.
Cytologic examination of the peritoneal fluid should include Wright-Giemsa and Gram stains. Peritoneal fluid cell structure is an important diagnostic aid and can be evaluated wth the Wright-Giemsa stain. Neutrophils are evaluated for degenerative changes such as nuclear swelling and cytoplasmic vacuolation, which indicates activation associated with the presence of bacterial toxins. Identification of exfoliative cells from neoplasms, such as melanoma, is rare but diagnostic and aids in directing therapy and prognosis.11 The Gram stain is used to identify bacteria and guide initial antimicrobial therapy until culture and sensitivity results become available.
Peritoneal fluid parameters consistent with peritonitis vary widely, depending on the disease process. Cytologic findings consistent with peritonitis include increases in total nucleated cell counts and protein with the predominance of degenerative neutrophils and intracellular bacteria. Nucleated cell counts ranged from 5800 to 350,000 cells∕μL, and protein levels were as high as 8 g/dL, in one study,2 but nucleated cell counts as high as 800,000 cellsZμL have been reported in horses with peritonitis. Cytologic evidence of extracellular bacteria can result from skin contamination and should be interpreted in relation to the clinical signs and remainder of the fluid analysis.
■ TABLE 32.9
Peritoneal Fluid Analysis in Normal Horses and After Conditions That Alter Peritoneal Fluid Values7-10
| Parameter | Normal | After Celiotomy | After Castration | After Foaling | Dystocia | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fluid character | Clear, straw- | Clear, straw-colored | Clear to cloudy | Clear, straw- | Serosanguineous | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Total nucleated cell | colored complications. FLUID THERAPY. Horses with peritonitis present with varying degrees of hypovolemia, dehydration, or both; thus fluid resuscitation with balanced, polyionic crystalloids should be the first step in treatment. Hypertonic solutions may be indicated in horses presenting with signs of hypovolemic shock, which may develop secondary to massive fluid shifts into the peritoneal cavity as a result of severe, acute inflammation. Because third spacing of albumin can lead to hypoproteinemia, administration of colloid solutions may be beneficial. Hetas- tarches (6%) are effective in fluid resuscitation and increase colloid oncotic pressure at doses of 8 to 10 mL/kg; however, caution should be used in patients with azotemia or underlying renal insufficiency because administration of those solutions is associated with acute kidney injury in humans.17 Large volumes of hyperimmune plasma may be used to raise plasma protein levels, whereas low doses (4.4 mL/kg) may aide in alleviating signs of endotoxemia.18 Acid-base disorders, as well as shifts in calcium, potassium, sodium, and chloride concentrations, may be observed in cases of peritonitis. Monitoring of acid-base status and electrolyte concentrations is recommended during the course of therapy with intravenous or oral supplementation as needed. See the ■ TABLE 32.10 Antimicrobial Therapy for Peritonitis in Adults
IM, Intramuscular; IV, intravenous; PO, oral; PR, rectal.
Fluid Therapy for Horses with Gastrointestinal Diseases section for a more in-depth discussion of fluid resuscitation and selection. ANTIMICROBIAL THERAPY. Antimicrobial therapy should be initiated in all cases of peritonitis, even when the inciting cause cannot be immediately identified. The site of infection, pathophysiologic features, pathogens probably involved, and concurrent patient conditions should be taken into consideration when an antimicrobial regimen is selected (Table 32.10). Lipophilic antibiotics (fluoroquinolones, potentiated sulfonamides) reach higher concentrations within the peritoneal cavity and in abscesses than do hydrophilic antibiotics (aminoglycosides, β-lactams); however, in the acute stages of the disease, inflammation of the peritoneal surfaces often causes hydrophilic antibiotics to reach therapeutic levels.18 Moreover, intravenous administration is recommended as drug concentrations achieved are more reliable than those achieved with oral administration in horses suffering from dehydration or ileus. A broad-spectrum antimicrobial regimen is recommended until culture and sensitivity results are available. Administration of a combination of a β-lactam and an aminoglycoside is appropriate; however, enrofloxacin may be substituted for gentamicin because of its increased lipophilicity or activity against Staphylococcus, or in cases of renal compromise. Metronidazole is often added on the basis of the frequency of B. fragilis isolated in horses with peritonitis. Oral antibiotic administration may be initiated after patients are stabilized and should be based on culture and sensitivity results. Antimicrobial selection in foals is based on age and likely causes of peritonitis. Neonatal foals with peritonitis should be maintained on broad-spectrum intravenous antibiotics, as for septicemia, including a combination of a β-lactam (ampicillin, 20 mg/kg IV qid, or ceftiofur, sodium 5 mg/kg IV bid) and an aminoglycoside (amikacin, 20 to 25 mg/kg IV q24h). Older foals and weanlings have a higher incidence of R. equi and S. equi infection; thus antimicrobial regimens in these patients include either penicillin (procaine penicillin G, 20,000 IU/kg IM bid) or a macrolide/rifampin combination in the absence 19 20 of other inciting causes.19, The duration of antimicrobial therapy is dependent on the inciting cause and the patient's response to treatment. Most peritonitis cases necessitate a minimum antimicrobial course of 7 to 10 days, and cases with intraabdominal abscesses may necessitate a 6- to 8-week course of antimicrobials. In cases of idiopathic peritonitis, antibiotics should be continued for several days after clinical signs resolve and peritoneal fluid counts return to normal. Other methods for monitoring progress and determining termination of therapy include serial ultrasound evaluation, CBCs, and measurement of fibrinogen levels in cases of internal abscesses. ANTIINFLAMMATORY THERAPY. All horses with peritonitis have varying degrees of local and systemic inflammation, and some may present with endotoxemia or endotoxic shock. Administration of medications with antiinflammatory properties, as well as those that bind and inactivate endotoxin, may be beneficial. NSAIDs should be administered in all cases of peritonitis for both analgesic effects and ability to reduce the production of inflammatory mediators through COX inhibition. Flunixin meglumine is most often used for its antiinflammatory properties and may be administered at higher doses (1.1 mg/kg IV or PO bid) in horses showing signs of discomfort or at lower doses (0.25 mg/kg IV or PO q6-8h) to minimize side effects. Other NSAIDs such as phenylbutazone (2.2 mg/kg IV or PO bid) or COX-2 selective firocoxib (0.1 mg/kg IV or PO q24h), may be used in place of flunixin meglumine. Lidocaine has become widely used as an antiinflammatory agent. Research demonstrated that horses administered LPS intraperitoneally and treated with lidocaine (1.3 mg/kg IV bolus followed by constant-rate infusion 0.05 mg/kg/min) had significantly lower clinical scores of endotoxemia and lower concentrations of plasma and peritoneal TNF-α than did those receiving saline.21 Therapy targeted at binding and inactivating endotoxin includes the administration of hyperimmune plasma, endoserum, and polymyxin B. Polymyxin B (3000 to 6000 IU/kg IV bid) has been demonstrated to effectively bind circulating endotoxin; however, its use carries a risk of nephrotoxicity and is cautioned in cases with azotemia or preexisting renal insufficiency. The pathophysiologic features of and therapy for endotoxemia are discussed in depth in the Endotoxemia and Sepsis section. ANTHELMINTICS. Peritonitis may develop in association with intestinal cyathostomiasis or verminous arteritis secondary to S. vulgaris migration; therefore anthelmintic administration is recommended when peritonitis is strongly suspected or in horses with a poor deworming history. Traditionally, fenbendazole (15 mg/kg PO for 5 days) or ivermectin (0.2 mg/kg PO) has been recommended after a horse with peritonitis is stabilized; however, resistance to both drugs has been reported. Alternative deworming protocols may include administration of moxidectin (0.4 mg/kg PO) or oxibendazole (10 mg/kg PO for 3 days). SURGICAL MANAGEMENT. Surgical intervention in peritonitis may be indicated to identify and correct the underlying cause, particularly when leakage or compromise of the intestinal or urogenital tracts is suspected. Ultrasonography occasionally reveals intraabdominal abscesses that could be drained via catheter or marsupialization. Peritoneal lavage and drainage should also be considered on the basis of peritoneal fluid analysis and are recommended when total nucleated cell counts exceed 100,000 cells/pL. The benefits of lavage and drainage include (1) reduction of bacterial numbers and concentrations of inflammatory mediators, (2) removal of foreign debris from the peritoneal/serosal surfaces, and (3) dilution of adhesionpromoting substances. Horses treated with peritoneal lavage must be monitored for dehydration, protein loss, and electrolyte imbalances. Complications associated with peritoneal drains include visceral puncture during insertion, ascending infection, subcutaneous leakage and edema, and herniation of intestine or omentum through the drain.22 Several techniques for peritoneal lavage and drainage have been described elsewhere, including the placement of ventral midline catheters in a standing horse, the use of active 18 23 24 intraabdominal systems, and open peritoneal drainage. ,, Standing intraabdominal catheters, such as Foley, mushroom, or thoracic catheters, may be briefly placed aseptically under ultrasonographic guidance by insertion through the skin, subcutaneous tissues, and external muscle layers at ventral midline, then secured in place with a purse-string suture and several half-hitch knots. Catheters are either allowed passive drainage and connected to a Heimlich valve or are connected to an active-drain system, to prevent ascending contamination. Balanced, polyionic solutions with a neutral pH are used to irrigate the abdomen. Antibiotics, antiseptics (povidone- iodine), and heparin have been suggested as additives to the lavage solution; however, no controlled studies have been performed to demonstrate any benefit. Severe inflammation of the peritoneal surfaces has been reported after the use of 3% or higher povidone-iodine lavage solutions. To perform peritoneal lavage, 10 to 20 L of solution is allowed to enter the abdomen via gravity flow through the ventral catheter. The catheter is then clamped and the patient is walked for 10 to 20 minutes to encourage distribution of the lavage fluid, after which the clamp is removed and the fluid is drained. This is repeated once or twice daily for 3 to 5 days or until fluid analysis findings normalize. A retrospective evaluation of 67 horses receiving active intraabdominal drainage after celiotomy revealed a high incidence of minor complications (49%), including obstruction of the drainage system, leakage of fluid around the system, and subcutaneous fluid accumulation. Moreover, the incidence of incisional infection in this group was higher (32%) than in the control group (23.5%); however, this was attributed to the severity of the primary condition for which the patients had 24 undergone surgery.24 Although open peritoneal drainage is preferred in humans and is reported to be successful in management of dogs and cats with peritonitis, this method has not been promoted in horses. In an experimental study, horses with induced peritonitis that received open drainage therapy with a plastic mesh sutured at the ventral abdominal wall had a significantly increased inflammatory reaction at the linea alba in comparison with those that were closed routinely. Moreover, all horses in the open drainage group developed incisional infections after removal of the mesh.23 ADHESION PREVENTION. Development of intraabdominal adhesions has a significant effect on long-term outcomes for horses with septic peritonitis. Systemic administration of antimicrobials, dimethyl sulfoxide, and flunixin meglumine has been promoted because it reduces adhesion formation by decreasing peritoneal inflammation.25 In addition, the systemic administration of heparin (20 to 40 IU/kg SC q8h) has been advocated for up to 72 hours in horses at risk of adhesion development or coagulopathy.25 Heparin acts to decrease fibrin formation through its inhibition of thrombin. Various intraperitoneal therapies have been evaluated in horses for the prevention of adhesions. Abdominal lavage, both intraoperatively and postoperatively, has demonstrated benefit in reducing the incidence of adhesion formation in horses undergoing exploratory celiotomy and those with peritonitis.22,24 Introduction of heparin directly into the peritoneum during abdominal lavage may be beneficial; doses of 20,000 IU are recommended26; however, studies of the effects of concurrent systemic and local administration on systemic coagulation have not been reported in horses. Intraperitoneal administration of recombinant tissue plasminogen activator and 0.4% sodium hyaluronate has been shown to decrease adhesion formation; however, these are currently cost prohibitive in clinical cases.25 The use of 1% sodium carboxymethylcellulose (2 L throughout the abdomen and applied to intestinal surfaces intraoperatively) has the most dramatic effect on adhesion formation, significantly decreasing the incidence of adhesions and the risk of death in 27 28 experimental horses in comparison with untreated horses. , ■ Prognosis Prognosis depends on the cause, severity, duration, and complications associated with peritonitis. Among horses with peritonitis, the prognosis is poorest for those suffering from gastrointestinal perforation or rupture and best for those with peritonitis associated with A. equuli. In two retrospective studies, rates of short-term survival were 86% (56 of 65) and 78% (43 of 55); however, both of these studies excluded horses with a diagnosis of gastrointestinal rupture.2,3 Another retrospective evaluation of 67 cases, including those with gastrointestinal rupture, demonstrated a higher mortality rate (40%).5 In that study, serum creatinine levels, anion gap, and pH at the time of presentation were significantly different between survivors and nonsurvivors; however, more recent research has not confirmed these findings. Celiotomy was found to have a negative effect on survival, with an odds ratio of 9.87 for nonsurvival in horses undergoing exploratory within 2 weeks of diagnosis or as a part of the treatment for peritonitis.3 Complications are not uncommon, occurring in 40% (22 of 55) of cases, and can have a negative effect on long-term survival.2,3 Reported complications include thrombophlebitis, ileus, diarrhea, drain site complications, intraabdominal adhesions, and laminitis. Monitoring and prophylactic therapy for these conditions may help reduce their adverse effect on outcome. With early diagnosis, correction of the inciting cause, aggressive medical therapy, and peritoneal lavage, the prognosis can be fair to good in acute cases of septic peritonitis in horses. Actinobacillus Peritonitis A subset of cases of peritonitis attributed to A. equuli infection has been reported among horses in Australia, New Zealand, and North America. Infection is generally thought to be secondary to translocation of the bacteria from the gastrointestinal tract or associated with Strongylus migration; however, the exact origin is unknown.29-31 Affected horses present with symptoms of mild to moderate colic (60%), tachycardia (94%), tachypnea (90%), decreased to no borborygmi (88%), and elevated rectal temperature (77%). A chronic form of the disease with a history of progressive weight loss is also reported. A poor deworming history was noted in 9 of 18 horses tested in which elevated numbers of strongyle ova were found on fecal examination.29,30 As with other causes of peritonitis, hemoconcentration, an absolute left shift, and hyperfibrinogenemia are common. In addition, peritoneal fluid cell counts are markedly increased—100,000 cellsZμL in 88% of samples (46,000 to 810,000/aL)—and protein levels are elevated in 98%. In contrast to other cases of peritonitis, cytologic findings are characterized by a predominance of nondegenerate neutrophils, and pleomorphic Gram-negative rods are identified in 53% of slides. A pure growth of A. equuli was obtained in 72% of cases.30 These cases responded rapidly to antibiotic administration (100% short-term survival), and most isolates were sensitive to penicillin; however, it is recommended that therapy include penicillin/gentamicin or oral therapy with trimethoprimsulfonamide until sensitivity results are available. Therapy should be continued for 7 days beyond return of peritoneal fluid analysis to normal values. Peritonitis associated with A. equuli is characterized by mild to moderate signs of colic, lethargy, elevated heart and respiratory rates, and marked elevations in peritoneal fluid protein and cell counts. It does not progress to endotoxemia or shock, and it is characterized by a rapid response to antimicrobial therapy, which distinguishes peritonitis associated with A. equuli from other causes of peritonitis. Hemoperitoneum Hemoperitoneum is defined as the abnormal accumulation of blood within the abdominal cavity. In several retrospective case series, researchers have evaluated the causes, clinical presentations, and outcomes associated with the diagnosis of hemoperitoneum.32-34 The various conditions diagnosed in horses with hemoperitoneum are summarized in Box 32.3. Clinical signs and prognosis depend on the cause and severity of the hemorrhage; however, most affected horses present with symptoms referable to abdominal discomfort/colic (78% to 79%) and hemorrhagic shock (60% to 85%), including tachycardia, tachypnea, pale mucous membranes, depression, weakness, and cool extremities.33,34 Antemortem diagnosis of hemoperitoneum is based on the identification of hemorrhagic effusion within the abdominal cavity by either ultrasonography or abdominocentesis. Characteristic swirling of echogenic fluid is noted on ultrasonography in cases of intracavitary hemorrhage, and a specific origin of hemorrhage may be identified on ultrasonography in 25% to 44% of cases.33,34 Peritoneal fluid analysis confirms hemorrhage with findings of PCVs greater than 5%, elevated protein levels, and gross appearance. Hematologic and biochemistry values are often unremarkable; however, alterations in acid-base status, blood gas analysis, and plasma lactate concentrations reflect the severity of hemorrhagic shock. Therapy for hemoperitoneum includes emergency stabilization of hemorrhagic shock, promotion of clot retention, and addressing the primary cause. Treatment of hemorrhagic shock includes conservative volume resuscitation with intravenous crystalloids, colloids, and blood transfusion (see the Fluid Therapy for Hemorrhagic Shock section in Chapter 44). Additional medications to support perfusion (inotropes, vasopressors) may also be indicated. Antifibrinolytics (aminocaproic acid at 3.5 mg/kg IV, conjugated estrogens at 25 to ■ BOX 32.3 Causes of Hemoperitoneum in Horses Idiopathic: Trauma Splenic rupture Rib fracture Pelvic fracture (iliac artery) Neoplasia Renal carcinoma Granulosal cell tumor Metastatic neoplasia Female Reproductive Tract Uterine artery Broad ligament tear Uterine tear/rupture Ovarian hematoma Ovarian dysgerminoma Vascular Aortic aneurysm Mesenteric rents Disseminated intravascular coagulation Hepatic Rupture Hepatic lipidosis Splenic Rupture Amyloidosis Hemangiosarcoma 50 mg/500 kg) are often administered to prevent breakdown of clots and help suppress continued hemorrhage.35 Exploratory laparotomy may have both diagnostic and therapeutic indications because the source of bleeding may be identified and corrected.34 Abdominal drainage and lavage is often not performed in these cases, unless severe abdominal distention precludes autotransfusion. To guard against development of septic peritonitis, antimicrobial administration is indicated if bacterial contamination is probably present. The prognosis for horses presenting with hemoperitoneum is guarded; overall survival rates range from 39% to 74% and depend greatly on the severity of hemorrhage, ability to control hemorrhage, and underlying cause.32-34 Nonsurvival is associated with respiratory rates higher than 30 bpm, diagnosis of neoplasia (odds ratio, 35.08), mesenteric vessel injury (odds ratio, 243.5), and uterine artery rupture (odds ratio, 13.72).33 Idiopathic hemoperitoneum is associated with the best long-term survival outcomes.34
More on the topic Disorders of the Peritoneum in Horses:
-
Veterinarian -
|