Disorders of the Descending (Small) Colon
Nimet Browne • Vanessa L. Cook
Colic resulting from a problem with the small colon is comparatively rare: It has been identified in only 4.2% of cases of surgical colic but represents up to 18% of horses admitted to referral centers with gastrointestinal disease.1-3 However, American Miniature horses seem to be at increased risk for obstruction of the small colon2; small colon lesions account for 60% of cases of surgical colic in that breed.4 Arabian horses and ponies also appear to be predisposed to small colon disease.2,5,6 Of interest is that horses older than 15 years of age also seem to be at an increased risk for small colon conditions,2 especially strangulating lipoma, injury from foaling, and submucosal hematoma.6 Mares may also be at increased risk for small colon lesions, possibly because of hormonal fluctuations affecting gastrointestinal motility,2 because of the small colon's predisposition to injury during foaling, or because of the small colon could become entrapped by an ovary.
One of the biggest challenges with small colon lesions is that the associated clinical signs and rate of physiologic deterioration are less severe than those of a more orad obstruction, which often results in later referral.2,6 Early clinical signs include lethargy and inappetance, whereas progression of disease typically results in abdominal pain, diarrhea, decreased fecal production, and abdominal distention. Gastric reflux occurs in 30% of cases with small colon strangulation.7 A complete examination of abdominal distention with rectal examination and abdominocentesis provides useful information in determining the diagnosis and indicating surgical intervention.6,8,9 However, because the small colon lies caudally in the abdomen, transabdominal ultrasonography may be less useful than it is for lesions in other sections of the intestinal tract.
Transrectal ultrasonography, performed with care, may be a more sensitive method of detecting a compromised small colon and may aid in earlier diagnosis.4Conditions affecting the small colon can be categorized as congenital diseases, simple obstructions, vascular lesions, neoplasia, or strangulating lesions.
■ Congenital Diseases
ATRESIA COLI AND AGANGLIONOSIS. Atresia coli is much rarer in foals than in calves; the reported incidence is 0.44%.10 There are several theories on the pathogenesis of this disease, but an ischemic vascular accident that results in atrophy of the affected segment is the most widely accepted one.11,12 One study showed that fibroblastic growth factor 10 and its receptor are important in colonic development in mice; the lack or deficiency in growth factors could play a role in colonic atresia in foals.13,14 There are four types of atresia.15 Type 3, blind-end atresia, with no connection of the atretic segments, is the type most commonly found in foals.10,14 Atresia coli may be confused with overo lethal white syndrome, in which affected foals have myenteric aganglionosis of the distal intestinal tract as the result of a mutation in the endothelin receptor type B gene.16,17 In atresia coli, however, the intestinal tract is patent but nonfunctional. Loss of neurons in the myenteric plexus of the small colon can also be found in equine dysautonomia (grass sickness), although it is usually less severely affected than the ileum.18
Newborn foals with atresia coli usually appear normal but develop progressive abdominal distention and colic within 24 hours of birth. Atresia can be differentiated from other causes of colic in foals by the complete absence of feces with no meconium staining on digital rectal examination or even after an enema.11 It may be possible to confirm a blind-ending rectum or distal small colon by digital palpation or passage of a soft catheter or endoscope.
However, the defect is usually too proximal to visualize this way, and the friable colonic mucosa can be perforated easily; therefore this method is not recommended for diagnosis, but the use of A7-butylscopolammonium can aid in diagnosis when colonoscopy is performed.19 Plain radiographs do not usually identify the atresia but can help differentiate it from a meconium impaction. Retrograde contrast radiography, as described later in this section for meconium impaction, may give a more definitive answer.20 A large volume of barium sulfate, up to 20 mL/kg, may be needed if the atresia is proximal to the transverse colon. If atresia is present, the path of the contrast agent is seen to end abruptly at the atretic segment.The only chance for survival in cases of atresia is early exploratory celiotomy to assess the affected segment and determine whether surgical correction is possible. In calves with atresia, the prognosis is vastly improved if the diagnosis is made early and the animal is alert and is stabilized medically before surgery.21,22 However, in foals, despite attempts at surgical resection of the atretic segment and anastomosis, the prognosis is grave; a 100% mortality rate has been reported in several studies.10,14
■ Simple Obstructions
SIMPLE IMPACTION. Small colon impaction is the most common abnormality of the small colon in adult horses, affecting 1.9% to 2.5% of all horses seen for colic at referral institutes.3,9,23 Several studies report a strong association between small colon impaction and diarrhea. The most recent study documented that horses with diarrhea are 10 times more likely to develop a small colon impaction than are horses with a large colon impaction.8,24 In other studies, diarrhea developed during hospitalization in 70% of all horses with small colon impaction, and 43% of those treated surgically yielded cultures positive for Salmonella spp.23 These studies suggest that impaction of the small colon may be a sequela to colonic inflammation or colitis, such as Salmonella infection; therefore some hospitals use isolation protocols for all horses with a small colon impaction.
Diarrhea, fever, leukopenia, and rectal mucosal edema are findings with small colon impactions and colitis; it is not known whether the underlying mucosal inflammation led to the impaction or whether the inflammation caused primarily by the small colon impaction predisposes horses to colitis.2,8,9 A dramatic increase in the incidence of small colon impaction has been documented in the fall and winter, possibly because of decreased water intake or close housing that increases the incidence of infectious colitis, but a definitive reason is unknown. Of interest is that this seasonal incidence was not significant in the most recent study, possibly because of the milder winters in the southern United States.8Diagnosis of a small colon impaction is most easily made by rectal palpation, with an accuracy of 79 to 87%.8,23 A solid tube of ingesta with loss of the normal sacculations is found, but other rectal examination findings include gas distention of the large intestine and cecum and loose manure.6,8,23 Great care should be taken in performing a rectal examination because the rectal mucosa may be edematous, and many horses will strain. 3 One of the best parameters for determining when surgical treatment of these cases is required is the presence of abdominal distention; affected patients are five times more likely to require surgical correction than are horses without abdominal distention.8 In addition, increases in abdominal pain and alterations in abdominal fluid that are consistent with deterioration of the bowel are also indications for surgery.2,6,8,23 Transabdominal trocharization in the right paralumbar fossa can be an effective and safe method of relieving gas accumulating orad to the impaction. This can be performed to relieve abdominal distention and improve the chance of success with medical therapy without the need to proceed directly to surgery.
Medical therapy should consist of intravenous fluid therapy to correct electrolyte abnormalities, in combination with enteral fluid therapy with a balanced electrolyte solution, and analgesics as necessary.9,23 Because enteral fluids can iniate the gastrocolic reflex and gastric distention can stimulate contraction of the colon, typically 4 to 6 L of warm water with 1 oz of sodium chloride alternating with 1 oz of potassium chloride can be administered via nasogastric tube every 2 hours.25,26 The administration of oral laxatives such as mineral oil, dioctyl sodium sulfosuccinate, or magnesium sulfate can be used to soften the impaction.
The time it takes for the impaction to resolve with medical treatment is often longer than for large colon impactions; mean time to resolution is more than 2 days.8 Affected horses that develop signs of systemic inflammation, such as fever, leukopenia, tachycardia, or tachypnea, may require treatment with antibiotics or antiendotoxin therapies.9 Enemas may be administered in a standing horse to break down very aborad impactions but should be done so with extreme caution to avoid mucosal injury. Adequate sedation, epidural anesthesia, and the administration of N-butylscopolammonium bromide may decrease the risk of injury.1,3,9,27Surgical correction of the impaction through exploratory celiotomy is usually performed with administration of a high enema and extraluminal massage by the surgeon. The impacted small colon is extremely friable, and the surgeon should be careful when manipulating the bowel in order to avoid serosal tears. Application of sterile carboxymethylcellulose to the serosal surface may help lubricate the intestine and reduce the trauma of manipulation. In severe cases, infusion of the impacted contents with isotonic fluids or an enterotomy in the small colon may be necessary to facilitate evacuation of the impaction.3 An additional concern is the risk of reimpaction of the small colon as ingesta from the large colon move aborally after surgery. Therefore if there are ingesta in the large colon at the time of surgery, a pelvic flexure enterotomy is also recommended so as to empty the large colon and reduce the risk of recurrence.23 Surgical correction of the impaction can be time-consuming; to reduce anesthesia time, the items needed for high enema administration, such as a stomach tube with a rounded atraumatic end, a stomach pump, and buckets of warm water, should be assembled in the operating room before induction.
The prognoses with medical and surgical treatment appear to be similar in most studies.8,23 Of interest is, however, that overall prognosis appears to have improved since the 1980s, increasing from approximately 75% in cases from 1986 to 1996 23 to approximately 95% in cases from 1999 to 2004.8 Therefore overall, the prognosis for small colon impaction is excellent, even if surgical intervention is necessary.
However, because of the underlying inflammatory cause of this condition, length of hospitalization tends to be longer and associated costs higher than those incurred with a simple large colon impaction.8Fecaliths, enteroliths, and foreign bodies. Simple obstruction of the small colon also involves inspissated feces (fecaliths), enteroliths, foreign bodies, or, less frequently, concretions of plant material (phytobezoars) or masses of matted hair (trichobezoars).
Fecaliths are improperly formed fecal balls, ranging in size from 4 to 6 cm, that are a result of poor diet, inefficient mastication, or reduced water intake.28,29 They are a common cause of colic in young or old (>15 years) miniature horses; an occurrence rate of 63% was documented in a study of surgical colic in miniature horses.4,29-31 Fecaliths that become lodged in the small colon usually cause complete intestinal obstruction and necessitate surgical removal, as described later. When colic is managed in a miniature horse, regardless of the cause, the serum triglyceride concentration should be monitored to allow early detection and treatment of hyperlipemia.32
Enteroliths are, as described previously, composed mainly of magnesium ammonium phosphate deposited in concentric layers around a nidus such as a small rock.33 The incidence is very high in certain regions, such as California, where enterolithiasis accounts for 15.1% of all cases of colic seen at the University of California, Davis,34 in comparison with less than 2% of colic cases at Texas A&M University.35 Enteroliths can lodge in the large colon, transverse colon, or small colon. According to some studies, the transverse colon may be the most common site of obstruction; however, larger trials indicate that the small colon is most commonly involved, with an incidence of 22%.34,36-38 Horses with enteroliths were found to have certain changes in the composition of their colonic contents, in comparison with other surgical colic cases, which may predispose them to enterolith formation. These differences include a more alkaline pH, more colonic fluid, and higher mineral concentrations.38 Certain management practices, including a high proportion of alfalfa in feed and less access to pasture, may also predispose a horse to enterolith formation.35,38
Clinical signs of enterolithiasis are similar to those seen with other nonstrangulating obstructions of the large or small colon. Many horses with enterolithiasis have a history of intermittent colic, but once the stone becomes lodged within the small colon, it can either be passed in the feces or become wedged.34 Most enteroliths that obstruct the small colon lodge in the proximal third, presumably because of the change in lumen diameter between the transverse colon and descending colon.38 Horses with an enterolith in the small colon are more likely to be tachycardic and leukopenic than are horses with an enterolith in the ascending colon.38 Sensitivity of radiography for the diagnosis of enterolithiasis ranges from 41.6% to 62.5% for enteroliths located in the small colon and from 75% to 91.67% for enteroliths located in the transverse colon. Digital radiography has been shown to be more sensitive than computed radiography, which in turn is more sensitive than analog radiography. Enteroliths in the large colon are easier to identify than those located in the small colon, and increased gas distention negatively affects the sensitivity of 39 41
radiographic images of enteroliths.39 41
Medical management aimed at reducing colonic pH has been suggested to try to prevent recurrence after surgery. However, when an enterolith lodges in the small colon, it usually causes complete obstruction and acute colic that necessitate surgical intervention, as described later. Rupture of the gastrointestinal tract is particularly common if the enterolith is lodged in the small colon and surgery is delayed.34
Ingestion of foreign material such as rope, twine, rubber fencing, cloth, or tires can also cause obstruction of the small colon.31,42 This is usually a problem in younger horses, possibly because they are more inquisitive and will eat nonfood items found in their environment. It is possible for the foreign body to cause signs of small intestinal obstruction first, followed by a period of quiescence while it passes through the large colon before it finally causes complete obstruction of the small colon and causes acute onset of severe colic and abdominal distention.1,42 The fibers become covered in crystalline material during their transit through the intestinal tract, and the resulting irregular sharp projections cause pressure necrosis and mucosal ulceration,6 which can be seen during exploratory celiotomy orad to the site where the foreign body has finally become lodged. These sharp projections make it virtually impossible to manipulate the foreign body orally or aborally within the lumen and thus make removal more complicated.
The majority of these obstructions necessitate exploratory laparotomy and an enterotomy to allow the obstruction to be removed.29,34,42 Regardless of the cause of the obstruction, the overlying intestine is friable and can rupture easily either during induction of anesthesia or during surgical manipulation.31,34,42 If possible, the mass should be gently manipulated more proximal or distal to the original site at which it lodged, so that the enterotomy can be performed in uninjured areas of the intestine.6 However, foreign bodies in particular may be difficult to manipulate, and the enterotomy may have to be performed directly over the top of the obstruction. The site selected for the enterotomy should be isolated from the abdomen with sterile towels before the enterotomy incision is made. The incision should be made longitudinally through the antimesenteric taenia in order to preserve luminal diameter, reduce hemorrhage, and maximize speed and ease of the procedure.43,44 The enterotomy can be closed in one layer with an inverting suture pattern.44 Small areas of necrosis caused by transmural pressure from the obstruction can be managed by oversewing the affected segment.
Problems arise when intraluminal obstructions occur at the proximal portion of the descending colon, where the lumen narrows between the transverse and descending colon. Here, manipulation of the obstruction aborally into a section of small colon that can be exteriorized may be impossible. In such cases, an antimesenteric teniotomy, through the seromuscular layer alone, can be performed. This allows the obstruction to be advanced aborally into a section that can be exteriorized, while the intact mucosa prevents abdominal contamination.45 The enterotomy and seromuscular incision are then closed as described earlier. An alternative approach is to administer a high enema to repulse the obstruction in an orad direction into the ascending colon, where it can be removed via a pelvic flexure enterotomy. Approximately 50% of horses with enteroliths in the descending colon have additional stones in the ascending colon; thus complete examination of the large intestine, especially the right dorsal and transverse portions of the colon, is recommended after the removal of a stone through a small colon enterotomy.34,38 The overall prognosis for horses with enteroliths of the descending colon is excellent. In one study, the short-term survival rate among horses that survived surgery was 94%.38 Common postoperative complications include fever, anorexia, and diarrhea, which do not seem to worsen the prognosis but may prolong hospitalization. Recurrence has been identified in up to 7% of 34
horses.34
MECONIUM RETENTION. Meconium is composed of substances that are present in the intestinal tract at birth, such as glandular secretions, sloughed cells, and swallowed amniotic fluid, and is therefore sterile. Healthy foals pass meconium, which is a thick, tarry substance, within 48 hours; the presence of soft, yellowish stool is an indicator that meconium passage is complete.30,46,47 Several studies indicate a higher incidence of meconium retention in colts than in fillies, presumably because the pelvis is longer and narrower in males.30,47 Any factors that reduce intestinal motility (such as failure to ingest colostrum) and dysmaturity can result in difficulty passing meconium, which is described as meconium retention. Clinical signs include tail flagging, straining, and reduced suckling, which can progress to more severe signs of colic over time, such as rolling and abdominal distention. These signs are similar to those seen with ruptured bladder, and the two conditions can occur together; therefore a complete examination of an affected foal is important.
It may be possible to palpate meconium retained at the pelvic inlet by careful digital rectal examination. If the meconium is retained more proximally, it may be identified on a plain lateral radiograph. Presence of the obstruction may be confirmed by retrograde contrast radiography, which provides excellent sensitivity and specificity for evaluation of the transverse and descending colon.20 Retrograde contrast radiographs may provide additional information when plain radiographs are inconclusive. A Foley catheter (28- to 30-French) is placed into the rectum, and up to 20 mL/kg (approximately 1 L) of 30% barium sulfate is carefully allowed to flow in by gravity until it squirts around the catheter or discomfort is observed.20 Lateral and, of more importance, ventrodorsal radiographs are then obtained. If a meconium impaction is present, the path of the contrast agent stops before it reaches the transverse colon. Ultrasound examination can reveal gas distention of the large intestine and, in some cases, the meconium itself can be identified as a row of fecal balls in the small colon. The echogenicity of the meconium varies, but a typical “speckled” appearance has been described.48-50
Supportive medical management of all affected foals should be performed first, including correction of fluid and electrolyte imbalances, provision of nutritional support, and correction of failure of passive transfer if indicated.51 Judicious use of analgesics such as flunixin meglumine or butorphanol and oral fluids may aid resolution of the impaction. The most effective treatment is administration of an enema. The enema can be a commercial phosphate enema or simply soap and water administered through a Foley catheter by means of gravity flow, as described previously. In cases that are refractory to simple enemas, an acetylcysteine enema may be effective. Acetylcysteine is a mucolytic, which acts by breaking disulfide bonds to make meconium less viscous. These enemas are available commercially (E-Z Pass Foal Enema Kit; Animal Reproduction Systems, Chino, Calif.) or can be formulated by adding 20 g of baking soda to 200 mL of water and then adding 8 g of acetylcysteine powder to make a 4% solution.47 The solution is infused slowly through a Foley catheter, which is then clamped to allow the solution to be retained for up to 45 minutes to allow maximum activity of the acetylcysteine. The meconium retention was resolved successfully in all acetylcysteine-treated foals in one study, although 5% of foals required three enemas before resolution was obtained, and three foals in the study developed a bladder rupture.47
One report indicated that in approximately one third of foals with meconium retention, exploratory celiotomy is needed for resolution.30 However, this study was carried out before the increased use of acetylcysteine retention enemas, and the current rate of surgical intervention is probably much lower. Because adhesions can develop in up to 33% of foals undergoing gastrointestinal surgery, long-term prognosis may be improved by reducing the number of foals undergoing exploratory celiotomy.30,47,52
OTHER CAUSES OF SIMPLE OBSTRUCTION. Because of the proximity of the descending colon to the urogenital tract, it is possible for the descending colon to be obstructed by intraabdominal structures such as an ovary or retained testicle. Although such conditions occur infrequently, the most common is for the small colon to become entwined around an ovary.6 The intestine can be freed and is not usually compromised, but the ovary itself is usually nonviable and must be resected.53 A similar problem has been reported from the spermatic cord of a retained teratoma that occluded the small colon.54
■ NeopIasia With the exception of lipomas, neoplastic processes of the small colon are quite rare. In a study characterizing intestinal neoplasia in horses, lymphoma and adenocarcinoma were the most frequent neoplastic lesions located in the small colon.55 Development of leiomyomas has been attributed to small colon intussusceptions, but they are also as incidental findings.56
■ VascuIar Lesions
INTRAMURAL HEMATOMA. Intramural or submucosal hematomas are rare, although some cases may not be diagnosed if they do not cause complete obstruction and if they resolve without intervention.57,58 Blood hemorrhages between the mucosa and muscularis layers, which expand to occlude the lumen and cause complete obstruction. If left untreated, hematomas can lead to ischemic necrosis of the bowel wall and thus to septic peritonitis, endotoxemia, circulatory shock, and possible death.57,58 The length affected has been reported to range from 24 to 65 cm. The cause is unknown, although blunt abdominal trauma has been associated with the condition in humans.59 In one equine case series, iatrogenic rectal trauma was implicated as the cause. 58 There is an increased incidence among older horses; those affected had an average age of 11 years in one study.6 Clinical signs include varying degrees of abdominal pain, as well as signs of vascular compromise from blood loss.6,58 The presence of dark or clotted blood on rectal palpation may aid diagnosis, and in some cases, a mass within the small colon may be identified.57,58
Exploratory celiotomy with complete resection of the affected segment and end-to-end anastomosis (as described later) is necessary. Because of the length of the affected segment, it may be difficult to exteriorize and resect all damaged intestine. However, if the entire affected segment can be removed, the prognosis is good; one study demonstrated a 75% survival rate.57
MESOCOLIC TEARS AND RECTAL PROLAPSE. Tears in the mesentery of the small colon can occur as a complication of parturition, especially in multiparous mares,60,61 and result in segmental ischemic necrosis of the small colon. Trauma and straining during parturition can result in tearing of the mesocolon and devitalization of the associated descending colon, which may progress to an intussusception of the small colon, which manifests as a type III or IV rectal prolapse. In a type III rectal prolapse, the rectal ampulla prolapses, as with a type II prolapse, but in addition, a portion of the small colon intus- suscepts into the rectum. In type IV rectal prolapse, part of the small colon and the rectum intussuscepts through the anus.60,62 Gentle palpation around the prolapse can help determine the type of prolapse. Although a rectal prolapse is readily identifiable, devitalization of the small colon caused by tears of the mesocolon results in a more insidious onset of clinical signs, including depression and lack of feces.60,61
The mesocolic tear is frequently located caudally; as a result, the affected area is inaccessible through a midline celiotomy. Therefore it may be more prudent to first perform standing flank laparoscopy to determine the location and extent of the lesion.63 This allows assessment of the lesion to determine whether resection and anastomosis of the affected segment via celiotomy are feasible or whether a permanent colostomy is required.64,65 The prognosis is often poor because of the extent of the tear or delay in surgical intervention.60,61,65
■ Strangulating Obstructions
STRANGULATING LIPOMA. Pedunculated lipomas can cause a strangulating or nonstrangulating obstruction of the small colon, but this occurs much less frequently than in the small intestine. In a large retrospective study, lipomas were found to involve the descending colon in approximately 10% of cases.2,7,66 The overall incidence of lipomas affecting any portion of the gastrointestinal tract is increased among older geldings and in Saddlebred and Arabian horses.66,67 It is therefore likely that lipomas specifically affecting the descending colon have a similar distribution. Fig. 32.72 illustrates a pedunculated lipoma that had strangulated a short section of the small colon.

FIG. 32.72 A short section of small colon that had been strangulated by a pedunculated lipoma.
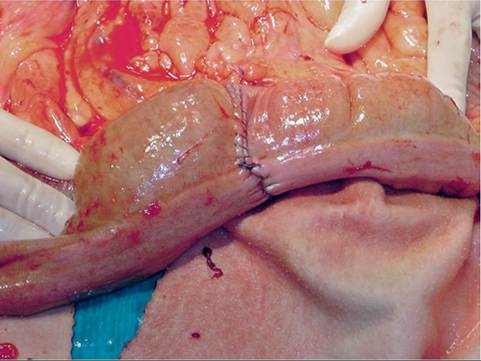
FIG. 32.73 The same case as in Fig. 32.72 after resection of the ischemic segment and end-to-end anastomosis.
Clinical signs typical of a strangulating obstruction include a significantly elevated heart rate, abnormal abdominocentesis findings, and distendtion of the large colon on rectal examination.6 Horses may only show mild to moderate signs of abdominal pain, in contrast to strangulating lesions in other parts of the gastrointestinal tract.7 Rectal examination may yield unspecific findings, but a constriction of the lumen of the small colon caused by the lipoma may be palpated and feels like a blind end or narrowing of the lumen.7
Surgery is necessary to free the constricting lipoma, followed by resection and anastomosis if the intestine is nonvi- able (Fig. 32.73). Strangulating lipomas of the small colon are the most common reason for resection and anastomosis.7 The prognosis is worse if resection is required, with a 50% survival rate in one study, in comparison with 100% survival for nonstrangulating lipomas.6 However, a multicenter study documented a substantially better survival rate after resection and anastomosis of the small colon; the majority of patients were horses with a strangulating lipoma.7 In that study, 84% of cases were discharged after hospitalization for a median of 8.5 days. The end-to-end anastomosis is usually sutured in two layers, with a simple continuous pattern in the mucosa followed by closure of the serosa with an inverting suture pattern interrupted at 180 degrees. It is possible that failure of the anastomosis occurs more commonly in the small colon than the small intestine, but numbers are too low to definitively confirm this.7 Diarrhea, fever, and delayed passage of feces are common postoperative complications, but long-term survival is good; of horses discharged in the aforementioned study, 93% were alive at 6 months.7
OTHER CAUSES OF STRANGULATING OBSTRUCTION. Several other causes of strangulating obstruction can occur, but each condition is relatively rare. These include volvulus of the small colon1 and strangulation through internal hernias such as a vaginal tear2 or tears in the gastrosplenic ligament.68 Intussusception can occur without rectal prolapse, and in some cases, the intussusceptum may protrude from the anus. Diagnosis can be made if a finger can be inserted between the protruding bowel and anal sphincter.56,65,69,70
■ Prognosis A good survival rate was found in two large reviews of small colon disorders: 71% and 91% of patients were discharged from the hospital.2,6 The main reason for euthanasia at the time of surgery was an inability to completely exteriorize the affected segment to allow adequate resection and anastomosis.6 Previous reports have suggested that resection and anastomosis in the small colon may carry a poor prognosis because of a relatively poor blood supply, higher bacterial counts, the presence of solid fecal material, and increased collagenase activity in comparison with the small intestine.1 However, among patients that survive surgery, short-term survival after surgery for a small colon lesion is excellent a rate of 100% survival was reported in one study.71 In addition, horses that required resection and anastomosis did not have a worse prognosis for survival2 and were less likely to develop the complications associated with small intestinal resection, such as postoperative ileus (POI).71