Disorders of the Trachea
Safia Z. Barakzai • Padraic Martin Dixon
Anatomy of the Trachea
The equine trachea extends from the caudal larynx to the carina where it divides into the two mainstem bronchi at the level of the fifth to sixth intercostal spaces and is about 75 to 80 cm long in a 500-kg horse.55 The trachea occupies a midline position in the neck and also in the rostral thorax, where it lies in a fold of mediastinum, but at its termination it becomes slightly displaced to the right by the adjacent aortic arch.56 It is composed of 48 to 60 individual tracheal rings of hyaline cartilage, which are incomplete dorsally.55 In the cervical trachea, the free ends of the tracheal rings usually overlap, but in the thoracic trachea, the free ends rarely meet.56 Each individual tracheal ring is 10 to 12 mm wide, being 2 to 3 mm thick dorsally and 5 to 7 mm thick ventrally.
The dorsal tracheal ligament completes the dorsal aspect of the tracheal lumen, attaching to the inner surface of the tracheal rings. The cartilage rings vary a little in shape in the normal horse; the first few rings are slightly dorsoventrally flattened but more distally the rings become more circular in shape. Finally, at the level of the aortic arch, the rings can become slightly laterally flattened, particularly on the left side.55 The tracheal ligament contains the transversely oriented trachealis muscle, and this elastic structure allows the trachea to expand slightly during times of increased respiratory effort.Each tracheal ring is covered by and connected to adjacent rings by an intimately attached fibroelastic ligament called the annular ligament. This arrangement of semirigid cartilaginous rings and elastic annular ligaments, along with the loose attachment of the tracheal adventitia to other tissues, allows much flexibility of the trachea during head and neck movement while retaining its rigid cross-sectional shape.
The cricotracheal ligament, which attaches the first tracheal ring to the cricoid cartilage, is of similar structure to the annular ligaments but is wider (craniocaudally) and under less tension.Running bilaterally along the dorsolateral aspects of the trachea are many vital structures, including the carotid artery, vagus and recurrent laryngeal nerves, sympathetic truck, tracheal lymph ducts, and cervical lymph nodes. The trachea is lined by a pale mucosa, containing numerous mucus and serous glands, and may contain fine longitudinal folds. Ciliated epithelial cells are the predominant cell type,57 with each cell containing about 200 cilia that beat 15 to 20 times per second. These cilia transport mucus from the lungs proximally to the nasopharynx. In the equine trachea, mucus is transported at a velocity of 13 to 20 mm/min.57 The “sump-like” depression in the rostral thoracic trachea is a common place for excessive respiratory secretions to accumulate in horses.58
Primary tracheal disorders are relatively uncommon in horses, but abnormal pooling of respiratory secretions in the “sump” of the trachea is often seen as a consequence of lower airway inflammation or exercise-induced pulmonary haemorrhage.59 Primary lung disorders are not discussed further in this section.
Cricotracheal Ligament Prolapse
A limited number of clinical reports describe this disorder in Thoroughbred racehorses during fast exercise.60-63 The cri- cotracheal membrane is normally longer (rostrocaudally) and under less tension than the tracheal annular ligaments. It is suggested that an abnormally long and/or slack cricotracheal ligament may prolapse dorsally, ventrally, or circumferentially into the airway lumen as a result of the very negative inspiratory airway pressures that are generated during fast exercise. One case series reported that cricotracheal ligament collapse can reduce the cross-sectional area of the tracheal lumen by 36% to 52%.63 Concurrent upper and lower airway disorders may increase the severity of cricotracheal ligament prolapse by further increasing the negative pressure generated within the upper respiratory tract.
■ Clinical Signs and Diagnoses Clinical signs include abnormal respiratory noise during exercise and reduced exercise performance61-63 due to the dorsally displaced ligament causing turbulent and restricted airflow. Differential diagnoses must include all forms of dynamic upper airway collapse, in particular those that are associated with inspiratory noise, including recurrent laryngeal neuropathy, medial deviation of the ary- epiglottic folds, vocal fold collapse, ventromedial luxation of the apex of the corniculate cartilages, epiglottic retroversion, and nasopharyngeal collapse. Diagnosis requires exercising endoscopy, either overground63 or on a high-speed treadmill, with a specific effort made to examine the caudal laryngeal area by having the endoscope tip positioned caudally and a good light source. In most reports of this disorder, multiple concurrent dynamic upper airway abnormalities are present.62-63 Presumably, cricotracheal collapse is exacerbated with head and neck flexion, as this position will reduce tension on the cricotracheal ligament; however, this has not been discussed in any of the case reports to date. Palpation of the ventral aspect of the cricotracheal ligament in the resting horse can subjectively reveal flaccidity, and much of the overlying tracheal lumen can be occluded with digital pressure. Ultrasonography of the ventral aspect of the cricotracheal ligament with the horse's head extended may be useful to measure the length and thickness of the ligament, but the range of these ultrasonographic measurements in normal horses has not yet been reported.
■ Treatment Conservative management of cricotracheal ligament collapse (7 days of oral phenylbutazone therapy) is reported to be successful in young (~2 years old) Thoroughbred racehorses that had other concurrent dynamic abnormalities noted on exercising endoscopy at the time of diagnosis.63 Horses in which cricotracheal ligament collapse spontaneously resolved had evidence of nasopharyngeal inflammation (grade 3 pharyngeal lymphoid hyperplasia) at the time of initial diagnosis.
This inflammation decreased or resolved at the time of follow-up exercising endoscopy, when the cricotracheal ligament collapse was noted to have resolved.63For persistent cases, treatment is via imbrication of the ventral aspect of this ligament after closing the space between the cricoid cartilage and the first tracheal ring.61,63 The dorsal half of the ligament cannot be accessed without risk of damaging the recurrent laryngeal nerves; however, Pollock and colleagues63 report that imbrication of the ventral aspect only appeared to prevent prolapse in two mature horses.
Tracheal Collapse
Tracheal collapse is commonly recorded in many breeds of toy dogs64-66 and can also occur in goats,67 sheep, and cattle (P.M. Dixon, personal observations). In Equidae, this developmental disorder is often reported in small ponies and miniature horses68-73 but also occurs in larger breeds of ponies74 and donkeys.71,75 In many small ponies, the disorder remains undiagnosed due to their low workload. There is a high prevalence of tracheal deformities in donkeys; in one postmortem study, 68.8% of tracheal rings did not have an oval or circular shape. Affected donkeys are usually asymptomatic unless severe tracheal deformity or intercurrent pulmonary disorders, such as advanced pulmonary fibrosis, are present.75
■ Pathophysiology Tracheal collapse is usually caused by a cartilage ring deformity, including where the normal rounded or oval tracheal ring is replaced classically by a flatter tracheal ring with a greatly reduced dorsoventral diameter (Fig. 31.49). In some cases, a slack and enlongated dorsal tracheal ligament can exacerbate the dynamic tracheal collapse.68,69,74 A more recent study also showed that most cases of tracheal collapse in donkeys were caused by grossly misshapen tracheal cartilages,75 and perhaps a term other than tracheal collapse should now be used.
Many ponies and donkeys with tracheal collapse will have some dorsoventrally flattened tracheal rings (especially in their lower cervical trachea) but will also have other types of ring deformities (Fig. 31.50) at more caudal thoracic sites.71,75 In other cases with relatively normal-shaped tracheal rings, there appears to be separation of the dorsal ligament from the dorsal aspect of the tracheal rings (Fig. 31.51). This defect usually involves the mid and distal cervical as well the intrathoracic trachea and may occasionally involve the mainstem bronchi. Some affected equids may also have a degree of tracheal rotation,
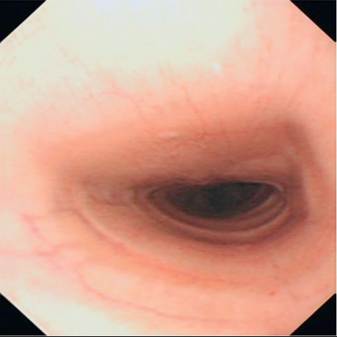
FIG. 31.49 Endoscopic view of a dorsoventrally collapsed trachea.

FIG. 31.50 Severe structural abnormality of an equid trachea.

FIG. 31.51 This tracheal ring is a normal C shape, but the dorsal tracheal ligament has separated from the dorsomedial aspect of the tracheal rings.
with the dorsal aspect of trachea facing dorsolaterally (authors' personal observations).
Most ponies and miniature horses develop clinical signs of tracheal collapse in middle age, 73,75 thus indicating that some degenerative process of the tracheal cartilage or connective tissue also plays a role in the pathogenesis of this disorder. In one case series of 13 American Miniature Horses, all 4 horses that had tracheal histopathology performed on them had chondromalacia, which varied from mild multifocal hyalinization of the extracellular matrix to marked multifocal coalescing areas of chondromalacia characterized by complete degradation of the cartilaginous matrix and loss of chondrocytes.73 The presence of chronic respiratory disease that may cause tracheal mucosal thickening and also increase intrapleural pressure swings, and neuromuscular problems causing loss of tone of the trachealis muscle have also been implicated in the pathogenesis of this disorder in donkeys.75
Temporary Tracheal Collapse
Horses with severe expiratory dyspnea due to pulmonary disease have increased positive intrathoracic pressure during expiration, which can cause a temporary collapse of the intrathoracic trachea, particularly of its dorsal ligament.
Such temporary and often near-total tracheal collapse can also be observed transiently in all horses if they cough during bronchoscopy.■ ClinicalSigns The typical clinical signs in affected equids are dyspnea and stridor, which commonly occur in hot or humid weather and may regress in autumn. Aleman and col- leagues73 report that clinical signs were initially intermittent and often associated with stressful events, exercise, dusty environment, and eating, but that all owners reported increasing severity of clinical signs with age. Stridor may be very loud, with Delahanty and Georgi68 reporting a pony that made sounds like a truck horn that could be heard more than 800 m away. The stridor is loudest when auscultated directly over areas of tracheal obstruction. Severe dyspnea may occur even at rest because hyperventilation will exacerbate the partial tracheal obstruction in a self-perpetuating cycle. Affected horses can also exhibit tachycardia (60 to 130 bpm) and hyperthermia (38.2o to 40.0o C).73
Exercise-induced pulmonary hemorrhage may occur in severe cases, presumably because of increasingly negative intrathoracic pressures. Coughing may also occur, and it is unclear if this is due to tracheal inflammation caused by abnormal contact of dorsal and ventral tracheal mucosa or due to underlying pulmonary disease that may have precipitated the clinical tracheal problem.
■ Diagnosis Palpation of a collapsed cervical trachea may reveal sharp lateral protrusion of the deformed cartilage rings. However, palpation of the lateral edges of the flattened trachea can be difficult, as the deeper, distal cervical trachea is most commonly affected. In addition, some small ponies such as Shetlands have very thick skin and much subcutaneous fat, which makes tracheal palpation difficult.54
Endoscopy of affected cases will show the normal circular or oval appearance of the tracheal lumen to be replaced by a wider, flatter, or otherwise restricted lumen. In addition, excessive dynamic movement of the dorsal tracheal wall and even airway occlusion may be observed during deep breathing, with inspiratory narrowing of the cervical tracheal lumen and expiratory narrowing of the intrathoracic tracheal lumen. The mucosa may be red and inflamed.
Lateral radiographs of the distal cervical and thoracic trachea may be diagnostic, demonstrating the flattened appearance of the trachea,69,73 but must be taken during inspiration for the cervical trachea and during expiration for the intrathoracic trachea. Radiography can be misleading in cases where tracheal rotation is present along with collapse, where the affected trachea may actually appear wider than normal on lateral radiographs.
■ Treatment and Prognosis Treatment of such cases should initially be conservative, by restricting exercise, keeping affected cases indoors in cool boxes with an adequate water supply in hot weather, and treating any concurrent pulmonary disease. Acutely affected horses will benefit from intranasal oxygen therapy that reduces hyperventilation and thus decreases the degree of tracheal collapse. Tracheostomy usually does not provide relief because it does not bypass the affected region (usually distal cervical and intrathoracic trachea). Therefore insertion of an endotracheal tube via the tracheotomy to keep the collapsed trachea patent is usually necessary to provide a temporary functional airway in severely affected animals. Hyperthermia, if present, increases the metabolic rate and thus increases the respiratory demand further, causing a vicious cycle of events. Cooling down such ponies with a cold-water hose can be beneficial. Parenteral corticosteroids are also indicated in severely affected cases to reduce the secondary tracheal mucosal inflammation or edema that is likely to be present. The long-term prognosis for severely affected miniature horses appears to be poor, with 10 of 13 horses in the largest case series to date either dying of this disorder or requiring
73
euthanasia.73
Surgical correction of affected cartilaginous cervical tracheal rings (as is commonly performed in miniature dogs), such as placing external stents over deformed tracheal rings70,76,77 or inserting stainless steel sutures into every third tracheal ring along with imbrication of the slack dorsal membrane,68 has been performed in horses and ponies with varying success. The use of a metallic intraluminal stent has also been reported to have been successful in one miniature horse, but intratracheal granulation tissue formation and lower airway infection was associated with the stented area.72 In some ponies, surgically altering the shape of the tracheal rings may not be successful because separation of the dorsal ligaments from the cartilage rings is the primary problem. In addition, careful evaluation will usually reveal involvement of the intrathoracic trachea, and because only 3 to 4 intrathoracic rings can be exteriorized cranially to the distal cervical area for surgical correction, this type of surgery may be of limited benefit to the horse. Although intrathoracic surgery to correct more caudal tracheal deformities is technically feasible, it is not practical.
Other Congenital Defects of the Trachea
Congenital defects of the trachea, other than tracheal collapse, are rare in horses, with only a few other types of deformities recorded, including a few reports of accessory or ectopic pulmonary tissue, including by Davis and colleagues,78 who recorded an accessory cervical tracheal bronchus in a 3-day-old foal. The foal presented with a large, air-filled sac in its cervical region caused by rudimentary accessory lung that contained cartilaginous tissue and ciliated epithelium. Peek and colleagues79 reported a combined tracheal and esophageal duplication cyst in a 4-month-old Arabian foal with a slowly developing cervical swelling that was successfully resected.
EXTERNAL TRACHEAL TRAUMA. Tracheal trauma is usually caused by blunt trauma, such as kicks to the neck region that can cause severe tracheal damage, particularly if the trachea is compressed between a hoof and the overlying cervical vertebral body. Tracheal trauma can cause tearing of the mucosa (Fig. 31.52) and of the overlying annular ligaments, and fracture of tracheal rings. Penetrating tracheal injuries occur less commonly.
■ Clinical Signs and Diagnosis A common presenting sign in horses with tracheal rupture is extensive subcutaneous emphysema and swelling over the cranioventral aspect of the neck.80-82 External skin wounds are not always present. The emphysema may later spread to involve the head, trunk, mediastinum, and even limbs. Horses will later become stiff and possibly febrile from secondary infection, and epistaxis and coughing may occur.81 In addition to possibly having a ruptured trachea, horses with emphysematous cervical swellings should always be suspected of suffering from a ruptured esophagus83 (authors' personal observations). Because the esophagus may lie lateral to the trachea at around the level of the sixth cervical vertebra in some horses, it is prone to trauma at this site.54
Cervical radiography of horses with tracheal or esophageal rupture will show extensive gas infiltration along the fascial planes of the neck, in addition to variable soft tissue or fluid-filled swellings of the cranial and ventral neck regions. Thoracic radiography may also reveal pneumomediastinum and possibly pneumothorax. Endoscopy (tracheoscopy) will confirm if tracheal trauma has occurred, by evidence of mucosal tears, prolapse of submucosal tissue into tracheal lumen, distortion or partial occlusion of the lumen due to cartilage ring fractures, and/or local inflammation.81,82 Esophageal endoscopy to examine the integrity of the esophagus should also be performed with the greatest of care in horses with neck swelling and emphysema.
■ Treatment and Prognosis If the esophagus is ruptured, the prognosis is poor, as compared to tracheal rupture, where the prognosis is usually good. Small tears of the tracheal mucosa will usually heal spontaneously. In addition to tetanus prophylaxis, NSAIDs should be administered to such cases to decrease the traumatic inflammation, along with broad-spectrum antibiotics to reduce the potential spread of pathogenic bacteria with entrapped air along the fascial planes of the neck and into the mediastinum. The emphysema present in such cases will usually resolve in 1 to 2 weeks but may remain for up to a month in some horses.81 Large rents in the tracheal mucosa with extensive herniation of soft tissue into the tracheal lumen can be sutured as described by Fubini and colleagues.82 Structural damage to the tracheal rings has been corrected using an extraluminal titanium mesh.76
Fractures of the cartilaginous tracheal rings with gross distortion of the trachea may also occur, and it may be difficult to evaluate the degree of cartilage ring damage in the presence of severe local inflammation and emphysema. If available, CT

FIG. 31.52 Tracheal trauma: oval-shaped tear in the tracheal mucosa showing separation of the underlying tissues.
or MRI of such lesions is the optimal method of assessing cartilage damage. If life-threatening tracheal obstruction occurs, a temporary tracheostomy may be performed with insertion of an uncuffed endotracheal tube through the tracheostomy to open up the collapsed section of trachea if the obstruction is distal to the mid-cervical region.
Intraluminal granulation tissue and subsequent development of circumferential fibrotic bands of tissue can be long-term sequelae of tracheal trauma. Occasionally such rings of tissue may eventually (months later) reduce the tracheal lumen to a significant extent, leading to respiratory obstruction with stridor. Transendoscopic laser resection of the protruding stricture can be attempted, but the site should be monitored postop- eratively for recurrence of the lesion. The use of topical corticosteroid after laser surgery may be of use in preventing recurrence of strictures. Complete resection of the affected cervical tracheal rings (up to four rings maximum) with end- to-end tracheal anastomosis can also be attempted,84 but such procedures can be very challenging. If the stricture is in the cranial cervical trachea, a permanent tracheostomy can be placed at a more distal site for horses that are not required for competition.
Intraluminal Tracheal Trauma
There have been several reports of intraluminal tracheal damage associated with the use of endotracheal tubes for maintaining general anesthesia, including inflammation,85 focal perforation,86 and severe ischemia of the tracheal mucosa if excessive cuff pressure is applied.87 An experimental study showed that histologic evidence of tissue damage was present in all horses at the site of cuff contact with the trachea, at pressures that are commonly used in clinical practice (up to 120 cm H2O).87 The use of ethylene oxide for sterilizing endotracheal tubes between patients may also pose a risk, as this chemical can be retained in rubber and plastic and can result in tissue necrosis if tissue comes into contact with the sterilized item.88
Recommendations for tracheal intubation in horses include flushing the horse's mouth before anesthesia, using a clean endotracheal tube, gentle intubation technique, minimal head and neck movement after the tube cuff is inflated, and disconnection of the endotracheal tube from the anesthesia machine while moving the horse.88 Measurement of cuff pressure should also be performed to identify excessive inflation.88
Focal Intraluminal Tracheal Lesions Including Neoplasia
Apart from granuloma formation post tracheostomy (Fig. 31.53) or after tracheal trauma, focal intraluminal tracheal lesions are
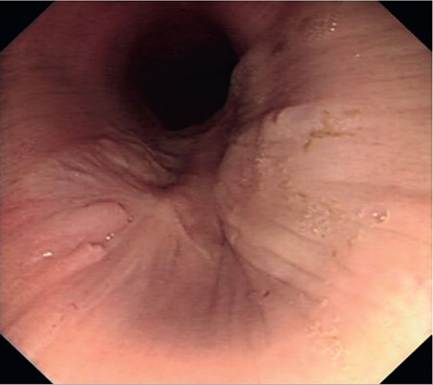
FIG. 31.53 Intraluminal scar tissue formation and cartilage deformity after tracheostomy tube removal.
rare in horses (although many horses and especially ponies have multiple small cartilaginous nodules that are of no clinical significance). Charlton and Tulleners89 reported infected or necrotic mid-cervical tracheal proliferative lesions in two adult horses following intratracheal antibiotic administration in one and following a transtracheal aspiration in the other. The masses were resected using a transendoscopic laser in one horse and a combination of transendoscopic laser and conventional surgery in the other.
Malignant tracheal tumours are rare in horses, but squamous cell carcinomas have been reported in the trachea of aged horses.90 Benign lesions including papillomas, fibromas, eosinophilic polyps, chondromas, and adenomas are more common91,92 and often can be successfully resected using a distal cervical tracheostomy and/or a transendoscopic laser excision. Transnasal retrieval of excised masses is usually possible using a transendoscopic grasping or “basket”-type forceps.
Extramural Tracheal Compression
Occasionally, enlarged lymph nodes compress the trachea, causing stridor. Severe lymphadenopathy is usually associated with S. equi subsp. equi (“strangles”) infection93 and may involve the upper cervical chain, compressing the proximal cervical trachea. They can also involve the distal cervical chain that compresses the trachea at the thoracic inlet. , 95 Diagnosis usually can be made from the history and clinical signs, which are indicative of strangles, and confirmation can be made by needle aspiration and/or ultrasonography of cervical swellings. Treatment of strangles is reviewed in the Streptococcus equi subsp. equi Infection (Strangles) section earlier in this chapter.
Mediastinal tumours, mainly lymphosarcomas; other cranial thoracic tumours, including primary lung tumours; or grossly abscessed mediastinal lymph nodes can cause compression of the intrathoracic trachea or of one or both mainstem bronchi, leading to stridor and dyspnea. Such an endoscopic finding should lead to a careful thoracic examination, including radiography and ultrasonography. Thoracic tumours are usually untreatable in the horse.
Tracheobronchial Foreign Bodies
Inhaled foreign bodies are common in man and dogs but less common in horses, possibly due to their height. O'Connor96 described a range of laryngeal and tracheal foreign bodies in horses and stated that a fatal bronchopneumonia could develop if the foreign body was not expelled by coughing. Inhaled foreign bodies seldom bypass the larynx, but if they do, they will usually become entrapped at the carina or in the mainstem bronchi,9'-100 predominantly in the right mainstem bronchus.76
A history of sudden onset of persistent coughing is a very prominent finding in these cases, and malodorous breath will often be present. Other signs of pulmonary disease, such as increased respiratory rate or the presence of abnormal lung sounds, are usually absent, at least initially, unless secondary lung infection occurs. If significant pulmonary infection develops, abnormal lung sounds and possibly purulent or blood-tinged nasal discharge may occur. No or only a temporary response (decreased coughing and nasal discharge) may occur following antibiotic therapy. Radiography may show a localized interstitial pattern caudal to the vena cava.99
Endoscopically, local airway inflammation and purulent respiratory secretions may obscure a foreign body. Even small foreign bodies may significantly obstruct airflow if they become lodged in a bronchus, and the induced local bronchial inflammation may also obstruct normal drainage of respiratory secretions from the affected bronchus, inducing severe, focal pulmonary infection. Transendoscopic lavage of the area may help determine if a bronchial foreign body or tumour is present. When identified, bronchial foreign bodies may be removed using transendoscopic grasping or basket forceps. Cranially facing leaves, branches, or thorns will make the recovery of such vegetation difficult, but with persistence, most bronchial foreign bodies will eventually become loose and retrievable. If this is unsuccessful, a distal cervical tracheostomy can be performed, and long, rigid, grasping instrumentation (such as broncho-oesophageal grasping forceps) can be used under endoscopic guidance to grasp and retrieve the foreign body.98,99
Epiglottic Entrapment
Santiago D. Gutierrez-Nibeyro
■ Definition and Etiology Epiglottic entrapment, persistent or intermittent, refers to the dorsal displacement of the aryepiglottic folds and subepiglottic mucosa over the epiglottis. The aryepiglottic folds attach to the free margins of the epiglottis and blend with both the dorsal epiglottic and the subepiglottic mucosa. Normally the subepiglottic mucosa is loosely attached to the epiglottis to allow movement of the cartilage during swallowing. The etiology of the disease is unknown, but inflammation of the subepiglottic mucosa and submucosa, redundant subepiglottic mucosa, and epiglottic hypoplasia or flaccidity have been reported as predisposing factors.1-4 Epiglottic entrapment has a reported prevalence of 8% to 27% in Thoroughbred and Standardbred racehorses,5-8 although it has been reported in nonracing Thoroughbreds and other breeds.9 Epiglottic entrapment is often an incidental finding in weanlings and yearlings.10
■ Clinical Signs and Differential Diagnoses Clinical signs are variable and depend on the severity of the entrapment and the presence of other diseases of the upper respiratory tract. Some racehorses can be asymptomatic and compete successfully with an entrapped epiglottis.8,11 However, affected horses most commonly have a variable degree of abnormal respiratory noise and/or exercise intolerance due to partial airflow obstruction.1,2,12 Clinical signs may also include coughing and nasal discharge.9,13 Severe inflammation and ulceration of the entrapping tissue can exacerbate airway obstruction and noise production; rarely it may also cause dysphagia.1,12 Potential endoscopic differential diagnoses include subepiglottic cysts, epiglottitis, epiglottic granulomas, and dorsal displacement of the soft palate.5,13,14
■ Definitive Diagnostic Tests Endoscopic examination of the nasopharynx with the horse at rest is frequently diagnostic. Typically the scalloped edge of the epiglottis and the vessels on its surface are not evident on endoscopy because they are obscured by the entrapping aryepiglottic fold (Fig. 31.54). Most epiglottic entrapments are persistent and thick, and approximately half of them are ulcerated.2,12 If the epiglottis is not entrapped during the initial endoscopic evaluation but intermittent entrapment is suspected, overground endoscopy or endoscopy during a high-speed treadmill test is necessary for definitive diagnosis.5,8
Although radiography is not used to diagnose the disease, an epiglottic entrapment can be detected using this diagnostic technique.4 Epiglottic hypoplasia can be determined with both subjective endoscopic evaluation and radiographic measurement of the epiglottic length (determined by thyroepiglottic length).4,15
■ Treatment and Prognosis Intermittent epiglottic entrapment may be treated conservatively with topical and systemic anti-iflammatory therapy and exercise restriction. Persistent epiglottic entrapment is typically treated surgically.2,12 Surgical techniques to correct epiglottic entrapment include transendoscopic axial division using a Nd:YAG or diode laser,2 transnasal or transoral axial division using a curved bis- toury,1,12,16-18 transnasal axial division using a shielded curved bistoury,19 transendoscopic axial division using monopolar electrocautery,20 transoral wire-snare resection of redundant subepiglottic mucosa,21 and surgical excision via a laryngotomy.3 Currently axial division of the entrapping aryepiglottic folds and subepiglottic mucosa is the preferred technique because the tissues are simply transected avoiding “debulking” of the epiglottis and excessive scarring postoperatively, which can cause dorsal displacement of the soft palate.22 Resection of the entrapping tissues through a ventral laryngotomy is typically reserved for excessively thickened, ulcerated, or fibroticappearing entrapping membrane.3 Postoperative care consists of topical and systemic antiinflammatory therapy and exercise restriction.
The prognosis is generally good; however, postoperative complications include recurrence of the entrapment, intermittent or persistent dorsal displacement of the soft palate, and epiglottis deformity.2,12,17,23 The recurrence rate after surgical correction of an entrapped epiglottis using laser axial division is 5%2; it is between 0% and 15% using a curved bistoury12,16,18,19 and as high as 40% using electrosurgical division.20
Pharyngeal Cysts in Horses
Santiago D. Gutierrez-Nibeyro
■ Definition and Etiology Pharyngeal cysts are uncommon in the horse1-3; however, they are occasionally diagnosed in young Thoroughbreds, Standardbreds, and Quarter Horses.4-8 Pharyngeal cysts occur most commonly in the subepiglottic region (Fig. 31.55) and occasionally in the soft palate (see the Congenital Palatal Defects section earlier in this chapter) or dorsal wall of the nasopharynx (Fig. 31.56).4,6,8 Some authors believe that subepiglottic cysts are embryonic remnants of the thyroglossal duct (precursor of the thyroid gland), but others believe that these cysts are secondary to inflammation and obstruction of the mucus-secreting glands that line the pharynx.5 Cysts formed within the dorsal nasopharyngeal wall are thought to be embryonic remnants of the craniopharyngeal duct (precursor of the adenohypophysis).4 The origin of soft palate cysts has not been elucidated; however, histopathologic examination of these cysts is consistent with a mucocele.6
■ Clinical Signs In foals subepiglottic cysts are frequently asymptomatic,3 but many cause increased respiratory noise, cough, nasal discharge, persistent dorsal displacement of the soft palate, dysphagia, and aspiration pneumonia.5,6 The most common presentation in the adult performance horse is partial obstruction of the upper respiratory tract, abnormal respiratory

FIG. 31.54 Endoscopic image of the nasopharynx of a 3-year-old Standardbred racehorse with a history of increased respiratory noise and chronic epiglottic entrapment. The entrapping membrane was thick, wide, and mildly ulcerated, and the epiglottis had moderate hypoplasia once the entrapment was corrected surgically. As in this case, most epiglottic entrapments are persistent and thick, and approximately half are ulcerated.

FIG. 31.55 Endoscopic image of the nasopharynx of a 2-year-old Standardbred horse with a small, smooth, and rounded subepiglottic cyst. The horse had a history of abnormal respiratory noise during training.
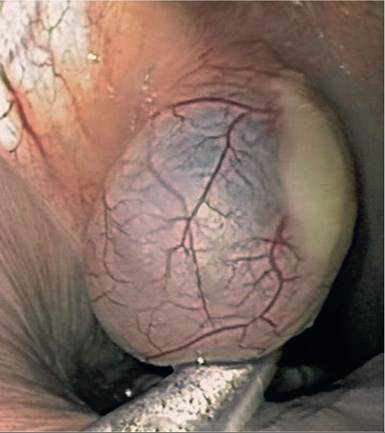
FIG. 31.56 Endoscopic image of the nasopharynx from a 1-week-old foal with a large cyst attached to the dorsal wall of the pharynx and a nasogastric tube in place. The cyst was resected with a cyst snare under endoscopic control.
noise, exercise intolerance, coughing, dysphagia, and in rare
4 7 9 cases, complete obstruction of the upper respiratory tract.4,'
■ Clinical Pathology CBC and biochemistry profiles are typically within normal limits unless concurrent inflammatory airway disease, pneumonia, or acute upper respiratory tract obstruction exists.
■ Definitive Diagnostic Tests Endoscopic examination of the nasopharynx confirms the diagnosis and may also detect concomitant pathology such as epiglottic entrapment.4,5,8 Occasionally a lateral radiographic view of the pharynx or transoral endoscopic examination of the oropharynx with the patient anesthetized is needed if the cyst is within the soft palate or beneath the epiglottis protruding into the oropharynx. Although contrast pharyngography has been described to help delineate cysts in the oropharynx,6 in the authors’ opinion the use of contrast is unnecessary if digital radiography is available. The use of ultrasound has been described to delineate the cyst from the adjacent structures before surgery, if necessary.10
■ Treatment and Prognosis Pharyngeal cysts can be surgically removed, ensuring complete removal of the secretory lining without excessive excision of surrounding pharyngeal mucosa in the case of a subepiglottic cyst, which may lead to cicatrization and epiglottic dysfunction.8 Subepiglottic cysts can be removed by a ventral laryngotomy,4 via an oral or transnasal approach using an endoscopically guided laser, electrocautery snare, or cyst snare constructed with obstetric wire loop threaded through a Chambers catheter.8,9 More recently, intralesional administration of 10% formalin has been reported, which provides an economically suitable alternative to surgical treatment11; however, multiple treatments may be required for complete resolution of the cyst.11 Postoperative care consists of topical and systemic antiinflammatory therapy and exercise restriction. The prognosis following removal of subepiglottic cysts is good, and most horses return to full athletic function.4,8 Less information is available regarding the prognosis after removal of other pharyngeal cysts.
Nasopharyngeal Cicatrix Syndrome
Ben Buchanan
The nasopharyngeal cicatrix syndrome is an inflammatory condition that was first described in 1987 in horses from south Texas1 and continues to be a common finding of horses grazing pastures in certain areas of Texas. It is also sporadically reported in other U.S. Gulf Coast states. The syndrome is a combination of inflammation and scarring of the nasal passage, pharynx, larynx, arytenoid cartilages, and proximal trachea. Severity ranges from incidental findings during endoscopy to airway obstruction that requires permanent tracheostomy.2,3
■ Clinical Signs Clinical signs include abnormal respiratory noise, nasal discharge, exercise intolerance, coughing, respiratory distress, and abnormal vocalization.4 The character of the nasal discharge is frequently clear and mild. When compared with a case-controlled population in a retrospective study, affected horses made up 118 of 1236 horses examined endoscopically for any reason.4 Of these affected horses, 97% had some degree of pharyngeal inflammation or scarring, of which 50% had a circumferential scar. In addition, 91% of affected horses had some inflammation or scarring of the larynx, and 39% had an airway obstruction, with the majority being at the level of the larynx. In this same study, horses with endoscopic evidence of acute nasopharyngeal cicatrix syndrome were more likely to have nasal discharge and respiratory distress, whereas horses with endoscopic evidence of chronic nasopharyngeal cicatrix syndrome were more likely to make respiratory noise or suffer from respiratory distress.
■ Endoscopic Signs A scoring system used by the author is presented in Fig. 31.57 and builds on a system previously proposed by Rakestraw.5 This system was developed to provide practitioners with a concise, simple, and complete system to document any abnormality of the upper respiratory tract seen on standing endoscopy.
NASAL PASSAGE. Both nasal passages should be examined. Lesions in the nasal passage appear as ulcerations and occur in less than 10% of cases.4
PHARYNGEAL SCAR. Schumacher and Hanselka first proposed a scoring system for this syndrome that focused on the pharyngeal scar.1 This system has been adapted into a 7-point scale, with 0 indicating no visible scarring. A score of
1 indicates a scar just forming on the ventral floor. A score of
2 indicates a consistent ventral scar. A score of 3 indicates a prominent ventral ridge with scarring just evident on the lateral walls of the pharynx. A score of 4 indicates a ventral scar with evidence of a dorsal scar just forming. A score of 5 indicates a complete ring with less than 25% reduction in the size of the airway. A score of 7 indicates a severe case with a complete ring that has reduced the airway more than 75% (Fig. 31.58).
GUTTURAL POUCH PLICA. Occasionally, scarring of the external guttural pouch plica is observed as a deformity to the guttural pouch openings.
PHARYNGEAL INFLAMMATION. The overall appearance of the pharyngeal walls should be graded with attention to degree of redness, edema, and chronic scarring. Acute/active is indicated by erythematous edematous tissue with or without discharge and no areas of scarring noted (Fig. 31.59). The level of inflammation should be graded as mild, moderate, or severe. Chronic/active is similar, with areas of active inflammation mixed with areas of previous scarring (Fig. 31.60). The degree of inflammation should be graded as mild, moderate, or acute.
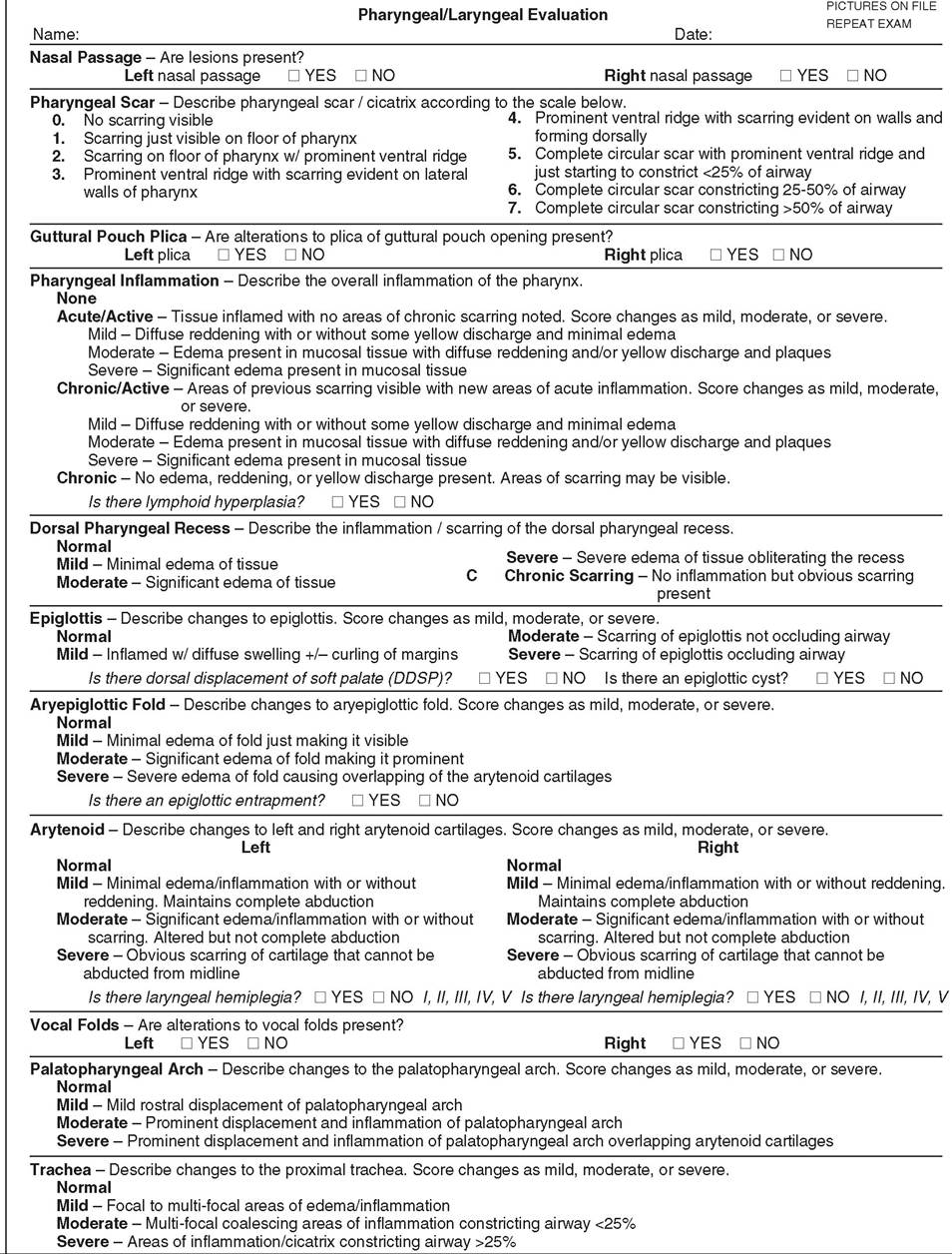
FIG. 31.57 PharyngealZlaryngeal scoring system.
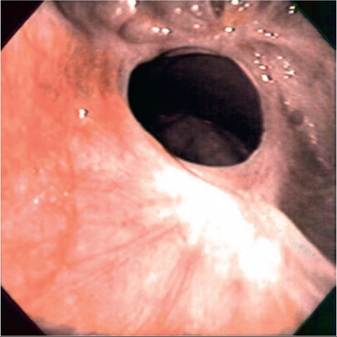
FIG. 31.58 Endoscopic image of nasopharyngeal cicatrix. This is an example of a grade 7 cicatrix.
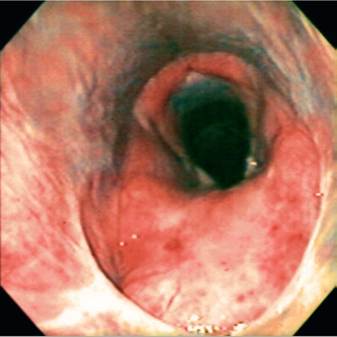
FIG. 31.60 Endoscopic image of chronic/active nasopharyngeal syndrome. There is both inflammation and swelling with a grade 3 cicatrix.

FIG. 31.59 Endoscopic image of acute pharyngeal inflammation and swelling consistent with nasopharyngeal cicatrix syndrome.

FIG. 31.61 Endoscopic image of chronic nasopharyngeal syndrome.
There is scarring of the epiglottis and left arytenoid cartilage and a grade 3 cicatrix.
A chronic description is indicated when there are areas of scarring with no active inflammation (Fig. 31.61). Any level of pharyngeal lymphoid hyperplasia should be noted.
DORSAL PHARYNGEAL RECESS. The dorsal pharyngeal recess should be examined for inflammation and areas of previous scarring. Occasionally this area is the only area of inflammation noted in the pharynx. The recess should be graded as mild, moderate, severe, or chronic.
EPIGLOTTIS. The epiglottis should be examined for swelling, scarring, displacement, occlusion of the airway, and cysts. Mild changes of the epiglottis include diffuse swelling with some curling of the margins. Moderate changes, although more severe, do not occlude the airway. Severe changes are noted as scarring of the epiglottis with occlusion of the airway. Any displacement of the soft palate or epiglottic cysts should be recorded.
AryepigLOTTIC FOLD. The aryepiglottic fold should be examined for edema and entrapment of the epiglottis. The abnormalities should be described as mild, moderate, or severe. Mild abnormalities are noted as minimal edema just making the fold visible. Severe changes are noted as significant edema causing the fold to overlap the arytenoid cartilages.
ARYTENOIDS. The left and right arytenoid cartilages should be evaluated for swelling, reddening, scarring, and abnormalities of abduction. Each cartilage is graded separately as having mild, moderate, or severe changes. Mild changes are noted as minimal edema or inflammation with or without reddening of the cartilage, with complete abduction. Moderate changes are noted as significant edema or inflammation with or without scarring, causing altered abduction of the cartilages. Severe changes are noted as obvious scarring of the cartilage that cannot be abducted from midline. Any laryngeal hemiplegia should be recorded.
VOCAL FOLDS. The vocal folds should be evaluated for edema and scarring. Changes in this area are common and should be recorded as present or absent.
PALATOPHARYNGEAL ARCH. The palatopharyngeal arch should be examined for edema and rostral displacement. The abnormalities should be described as mild, moderate, or severe. Mild abnormalities are noted as minimal edema causing minimal displacement. Moderate changes are noted as significant edema causing a prominent rostral displacement. Severe changes are noted as significant edema causing overlap of the palatopharyngeal arch over the apex of the arytenoids. Rostral displacement of the palatopharyngeal arch was noted in 36% of cases.4
TRACHEA. The proximal trachea should be evaluated for areas of edema, inflammation, and scarring, as lesions in the proximal 6 to 10 rings of the trachea are common. Changes in this area should be graded as mild, moderate, or severe. A mild change involves multifocal areas of inflammation not reducing the size of the airway. A moderate change involves areas of inflammation causing a reduction in the airway of less than 25%. A severe change causes airway reduction greater than 25%. Abnormalities in the trachea have been reported in 75% of cases.4
■ Progression This syndrome is rarely seen in horses younger than 4 years of age, and the length of time for an acute case to develop respiratory distress is unknown. In the author's experience the most severe cases occur in older horses.
■ Pothogenesis To date no specific etiology has been identified, although some risk factor analysis has been completed. A retrospective case-control study of 121 horses2 with nasopharyngeal cicatrix syndrome found a high association with housing on pasture or part time on pasture and with increased age. Cases of nasopharyngeal cicatrix syndrome were more likely to be presented in the summer months, with acute cases also being seen in the spring and fall. No breed or sex risk factor was noted. Cases seem to be more prevalent in years with higher rainfalls, although a few new cases may be seen during times of drought.
Inhalation of larger sized particulate matter (>5 microns) is suspected to be the inciting cause, as these particulates are deposited in the nasal mucosa, pharynx, larynx, and proximal trachea. This corresponds to the anatomic areas where the inflammation and subsequent scarring are noted. Whether these particulates include bacteria, fungus, allergen, or some other irritant is not known. There is some discussion of the oomycete Pythium insidiosum as a possible cause, although in the author's experience this is not likely a primary pathogen in these cases.
■ Treatment Because the agent or combination of agents causing this syndrome has not been identified, a single effective therapy has not been found. In addition, identification of effective treatments is complicated by the chronicity of the syndrome when it is typically first identified, the cyclical or seasonal nature of the clinical signs, and the response to changes in environmental factors. Current therapy consists of reducing exposure to pasture and reducing inflammation. No treatment has been effective if the horse remains on pasture. Surgical resection of affected areas frequently leads to excessive granulation tissue, especially after arytenoidectomy. If the airway is compromised, a permanent tracheostomy is the therapy of choice. If surgical reduction of the affected tissue is elected and the horse is not moved to a new environment, the lesions will recur.
■ Outcome In acute cases, simply removing the horse from pasture and feeding in a dry lot or stall resolves most of the condition. It is believed that repeat or continual exposure of acute cases leads to the chronic scarring. Once the chronic scarring has developed, it will not resolve.