Disorders of the Equine Soft Palate
Safia Z. Barakzai • Padraic Martin Dixon
■ Anatomy and Physiology of the Soft Palate The equine soft palate extends caudally from the hard palate and completely divides the pharynx into nasal and oral compartments.
Because the horse is an obligate nasal breather, the caudal border of the soft palate normally fits snugly around the base of the epiglottis, and the soft palate remains in this subepiglottic position at all times except during deglutition. The soft palate consists of the oral mucous membrane, palatine glands, palatine aponeurosis, palatal muscles, and nasopharyngeal mucosa. The soft palate is relatively thick (>2 cm) rostrally and tapers caudally as the amount of glandular tissue within it reduces considerably.1 The paired muscles that control palatal position include the palatinus muscles (running rostrocaudally on either side of midline), the palatopharyngeus muscles (running from the palatine aponeurosis and lateral aspect of the palatinus, sweeping laterally up the walls of the nasopharynx), the tensor veli palatini muscles that tense the rostral aspect of the soft palate, and the levator velipalatini muscles that elevate the soft palate during deglutition.The dorsal aspect of the soft palate forms the floor of the nasopharynx and has longitudinal ridges that become more apparent endoscopically when the palate is flaccid. Horses that resent endoscopic examination of the upper respiratory tract often tense their soft palate, giving its rostral aspect a dorsally “domed” appearance.
Dysfunction of the soft palate presenting as dorsal displacement of the soft palate (DDSP) or palatal instability (PI) at fast exercise is by far the most frequent palatal abnormality that clinicians are presented with in equine practice. Other palatal disorders are relatively uncommon.
Dorsal Displacement of the Soft Palate and Palatal Instability
Palatal dysfunction, which includes the two syndromes of DDSP and PI, is the most commonly diagnosed cause of upper airway obstruction in racehorses, with a reported prevalence of around 10% to 20%.2,3 It also affects other types of horses, particularly those that are exercised with their head and neck in a flexed position, such as dressage horses, showjumpers, and Saddlebreds.4,5 Intermittent DDSP is a disorder that characteristically occurs in horses toward the end of fast work, when the caudal border of the soft palate becomes displaced dorsal to the epiglottis (Fig.
31.45). A definitive diagnosis of intermittent DDSP or PI can only be made using exercising endoscopy on a treadmill or using overground endoscopy. Palatal instability is seen as wavelike dorsal billowing of the rostral and caudal aspects of the soft palate but without actual displacement of the caudal border of the soft palate dorsal to the epiglottis. Palatal instability commonly precedes DDSP.6-9 Swallowing may temporarily halt PI, but instability usually recurs within a few seconds and may then progress to true DDSP. As the soft palate “billows” dorsally, it may lift the epiglottis, changing the epiglottic conformation and causing the aryepiglottic folds to deviate medially.9,10 It is unclear what degree of soft palate instability is “normal” and what percentage of horses diagnosed with PI would experience DDSP under different conditions, such as training versus racing. When PI is observed in isolation, it has been described as equivalent to a “presumptive” diagnosis of DDSP11 and has also been suggested as a “prodromal” sign of impending DDSP.9,12“Rostral palatal instability” is another form of palatal instability that has been reported in horses and ponies, associated with neck flexion during exercise.13,14 As the name suggests, the condition is characterized by dorsoventral billowing confined to the rostral aspect of the soft palate. Rostral palatal instability causes inspiratory nasopharyngeal obstruction and respiratory noise. Experimentally this condition has been produced by bilateral tensor veli palatini tenectomy.15
■ Pathophysiology Horses that have other abnormalities of the palate or larynx, such as epiglottal entrapment, pharyngeal paralysis, and palatal cysts, are predisposed to DDSP. If no such abnormalities are present, the etiology of the disorder is currently unknown despite research efforts to improve understanding of the condition, with the ultimate goal of developing more effective treatments.15-20 Current theories include neuromuscular dysfunction of the intrinsic soft palate muscles,20-22 variations in the anatomic positioning of the laryngohyoid apparatus and the role of the thyrohyoid muscles in laryngeal “elevation,”19,23,24 and the role of the distal hypoglossal nerve in maintaining nasopharyngeal stability.25 Epiglottic hypoplasia

FIG.
31.45 Dorsal displacement of the soft palate seen in a horse undergoing exercising endoscopy. The epiglottis can no longer be visualized.or flaccidity was previously thought to be associated with intermittent DDSP. However, clinical and experimental data show that the epiglottis is not required to maintain the palate in a normal position and that the majority of horses that experience DDSP during treadmill endoscopy have an epiglottic length that is within normal limits.
■ Clinical Signs Most horses with DDSP make a rough “snoring” or “gurgling” noise at exercise and may either pull up abruptly or slow down significantly after the palate has displaced. DDSP results in a flow-limiting expiratory obstruction, leading to decreased airflow, increased tracheal expiratory pressure and impedance, reduced minute ventilation and subsequent hypoxia, hypercapnia, and impaired athletic per- formance.17,26,27 Conversely, once the soft palate has displaced, minimal obstruction is observed during inspiration as the upper airway inspiratory pressure maintains the soft palate in close apposition to the dorsal aspect of the epiglottis. During expiration, because a proportion of the exhaled air is directed ventral to the displaced palate and into the oral cavity, some horses are reported to exhibit “fluttering” of the cheeks during exhalation. Palatal instability has also been shown to have a negative effect on ventilatory parameters if moderate to severe.28 Low- frequency fluttering of the caudal border of the palate is believed to be the source of the loud expiratory and inspiratory “gurgle” or “snore” reported in 70% to 80% of affected horses29; however, up to 30% of horses can experience DDSP yet make no audible abnormal respiratory noise (“silent displacers”).30-32
■ Diagnosis An accurate history that includes details of reduced exercise performance and of abnormal noise production, including the type of noise made and the stage of exercise when it occurred, can be very helpful.
A thorough resting endoscopic examination of the nasopharynx should be performed to rule out other causes of palatal dysfunction such as pharyngeal or palatal cysts, epiglottic entrapment, or pharyngeal paralysis. The lower portion of the respiratory tract should also be examined for evidence of lower airway disease. DDSP and PI are dynamic conditions, and findings of resting endoscopy have been shown to correlate poorly with dynamic endoscopic findings.12,31,32 Horses that displace their soft palates at rest are often normal during exercising endoscopy, and conversely many horses that are normal during resting endoscopic examination can develop DDSP at exercise.12,32 One study reported that use of a characteristic history of gurgling and poor racing performance plus findings of resting endoscopy alone resulted in a 35% misdiagnosis rate of palatal dysfunction, as compared to findings of treadmill endoscopy.32Exercising endoscopic examination, either on a high-speed treadmill with a standard videoendoscope or during ridden or driven exercise using a portable telemetric endoscopic system, is the gold standard for diagnosis of DDSP and PI.3,6-8,12,31-34 Clinically normal horses may transiently displace their soft palates during exercise and particularly when pulling up. However, a normal horse typically swallows and replaces the palate to its normal subepiglottic position within a few strides, whereas DDSP is typically diagnosed if the palate remains dorsal to the epiglottis for a longer period of time (several seconds) or if DDSP occurs repeatedly.
Sound analysis has also been used as a research tool for diagnosis of DDSP,30 but it has not been reported in significant numbers of clinical cases and its accuracy is therefore unknown. A significant relationship has been reported between the depth of the basihyoid bone measured using percutaneous ultrasonography at the caudal aspect of the lingual process at rest and the occurrence of DDSP at exercise.35 A more ventrally located basihyoid at rest was associated with an increased probability of DDSP occurring during treadmill endoscopy.
This test had a high negative predictive value (89%) but a low positive predictive value (36%),35 meaning that DDSP could be ruled out with reasonable certainty but that care should be taken when making a positive diagnosis of DDSP using this method.■ Treatment Many treatments are available for horses with DDSP, and this probably reflects both the unknown etiology of the disorder and the fact that most treatments have a similar success rate. Concurrent respiratory disorders, including upper or lower airway inflammation or infections, should be addressed fully, prior to resorting to surgical remedies, and if the horse has only just been brought into work, improving its fitness can resolve palatal issues. The use of systemic corticosteroids, NSAIDs, and topical antiinflammatory nasopharyngeal (“throat”) sprays has been advocated to try to reduce upper airway inflammation.2,31 One study showed that in young 2- and 3-year-old Thoroughbred racehorses, 56% of horses with DDSP were reported to show spontaneous resolution of the disorder within 3 months of their initial exercising endoscopic diagnosis, without receiving any specific treatment.35 Spontaneous resolution was less common in older racehorses, with only 12% no longer experiencing DDSP on repeat overground endoscopic exam.36 Tack changes, including use of a tongue tie,36,37 dropped or crossed noseband,36-39 and “W” or “Serena Song” bits, have also been reported anecdotally to be of benefit in affected racehorses. The laryngohyoid support device (“Cornell collar”) has been advocated as a nonsurgical “tieforward” procedure for horses with DDSP and was effective in 100% (7 of 7) of horses with experimentally induced DDSP.40 In horses with naturally occurring DDSP, the Cornell collar was reported to be effective in around 60% of horses by one study.36
Surgical treatments for DDSP are numerous and include insertion of a thyrohyoid prosthesis (the laryngeal “tie-forward” procedure), staphylectomy, myectomy of the sternothyrohy- oideus muscles, epiglottic augmentation with Teflon™, tension palatoplasty, thermocautery of the oral surface of the palate, laser cautery of the nasopharyngeal surface of the palate, in addition to multiple combinations of these procedures. A systematic review of treatments for palatal dysfunction in the horse41 concluded that “the low level of evidence makes it difficult to draw firm conclusions as to the efficacy of procedures used to treat DDSP” The use of combinations of surgeries usually represents a “belt and braces” approach but arguably may provide a multimodal approach to a disorder with a multifactorial etiology.
However, the use of multiple treatments in scientific studies also means that we are often left unsure as to which of the reported treatments, if any, may have had a beneficial effect.41Failure of surgical remedies for DDSP is not uncommon. As a surgical principle, it is unwise to repeat a surgical procedure that the animal did not respond to the first time, unless the surgical procedure can be documented to have been performed suboptimally or has technically failed (i.e., broken or loose tie-forward suture).42 Furthermore, the morbidity associated with certain procedures such as staphylectomy makes their repetition risky.42 Few studies have analyzed the effects of surgery for DDSP using the “gold standard” of postoperative exercising endoscopy. A study that performed overground exercising endoscopy on 20 racehorses after laryngeal tieforward showed that the surgery eliminated DDSP in 65% of horses but that 70% still exhibited a degree of palatal instabil- ity.43 However, this study population was biased toward horses that had a suspected problem after the tie-forward (60% of cases presented had trainer-reported ongoing respiratory noise and/or poor performance).43 Causes of failure of laryngeal tie-forward include not having a definitive diagnosis of the palatal issue preoperatively, migration of the larynx caudally after surgery, and suture pull-through or failure.
Persistent Dorsal Displacement of the Soft Palate
Persistent DDSP, where the soft palate is permanently positioned dorsal to the epiglottic cartilage, is rare compared to intermittent DDSP. It is observed in the resting horse and is often secondary to underlying structural abnormalities such as subepiglottic cysts, epiglottitis, epiglottic entrapment, intrapalatal cysts, pharyngeal paralysis, pharyngeal neoplasia, or pharyngeal foreign bodies,13,41 but it can also be idiopathic. Persistent DDSP is seen most commonly after surgery to release epiglottal entrapment44-46 if a large fold of the subepiglottic mucosa is resected but has also been reported after many other types of laryngeal surgery, including laryngoplasty and Ventriculocordectomy.47 Horses affected with persistent DDSP make a loud gurgling noise at exercise, have poor exercise tolerance, and can be dysphagic, often coughing when eating.44,47
■ Diagnosis Diagnosis is easily made by endoscopic examination of the nasopharynx in the resting horse where the epiglottis is never visible because the soft palate lies dorsal to it. Horses should be prompted to swallow several times during the examination to see if any transient relocation of the palate occurs. Ulceration of the caudal border of the soft palate can sometimes be observed. Observation of persistent DDSP with the endoscope passed per nasum, is an indication to perform endoscopy of the oropharynx (with a full dental speculum in place) to examine the epiglottis and associated structures for abnormalities. If 60-cm broncho-oesophageal forceps are available, the larynx and caudal soft palate can be desensitized by application of topical local anesthetic and the forceps then used to manipulate the palate to a subepiglottic position and to elevate the epiglottis to examine its ventral aspect (Fig. 31.46).
■ Treatment In most cases, persistent DDSP is secondary to some other disorder, and treatment should therefore be directed at the initiating cause. If no primary disorder is found, the tie-forward procedure (laryngohyoid prosthesis) has been reported to be effective in alleviating idiopathic persistent DDSP in 7 of 15 affected horses.44 In the same case series, the remaining 8 of 15 horses additionally required laser staphylectomy after the tie-forward procedure to resolve persistent DDSP.44 A subepiglottic “releasing” incision, which may include a hyoepiglottic myotomy, has also been described for treatment of cases where it was felt that the epiglottis could not be manually repositioned dorsal to the palate due to subepiglottic adhesions.47
Congenital Palatal Defects
Congenital defects of the palate (cleft palate or palatal hypoplasia) are rare in horses, having a reported prevalence of 0.01% to 0.02%.2 True cleft palates arise from incomplete embryologic closure of the palatal folds, but often there is a tissue deficit that should correctly be called palatal hypoplasia. Tissue defects or clefts may involve only the caudal aspect of the soft palate (Fig. 31.47) or both the hard and the soft palates. Affected foals should be examined carefully for other congenital defects such as cardiac, GI, and nasal septum abnormalities.
■ Clinical Signs and Differential Diagnosis Clinical signs of cleft palate include nasal regurgitation of milk (in foals) or other feed material in older horses, coughing, poor growth, and signs indicative of aspiration pneumonia such as cough during eating and persistent nasal discharge.48-52 If the defect is small, abnormal respiratory noise due to PI or DDSP may be the only presenting sign, or the foal or horse may be asymptomatic. Endoscopic examination of the nasopharynx (using a small-diameter endoscope) reveals an abnormal outline to the caudal soft palate and food material within the nasopharynx, larynx, and trachea. The defect can be characterized by a midline cleft where there is an almost normal amount of tissue but failure of fusion of the left and right sides, a unilateral (Fig. 31.48) or bilateral soft palate hypoplasia. Defects of both the hard and the soft palates are less common (7% to 18%48,52), and these animals are usually presented as foals,48 probably due to the increased severity of clinical signs. Differential diagnoses for dysphagia with aspiration of food material in foals includes subepiglottic cysts, pharyngeal paralysis or dysfunction (which can be transient in neonatal foals,53 particularly if premature or dysmature), and in older horses, oesophageal obstruction (choke), guttural pouch mycosis, severe arytenoid chondritis, complications of laryngeal surgery (e.g., laryngoplasty or arytenoidectomy), and large pharyngeal cysts or pharyngeal or laryngeal foreign bodies or neoplasms.
■ Treatment If signs associated with the palatal defect are confined to noise during exercise, occasional coughing after eating and/or nasal discharge (i.e., there are no or minimal systemic signs), affected foals can survive to adulthood and may be capable of ridden work if left untreated or treated symptomatically.48,51,52 Surgical repair is possible for foals with less than 20% to 30% of the palatal tissue missing, but this is generally a salvage procedure only, and only a few go on to
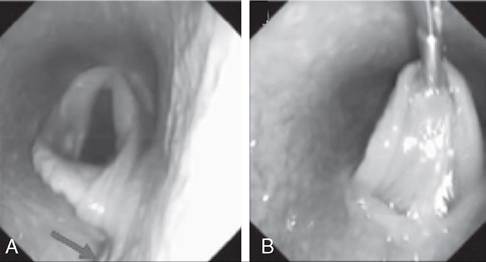
FIG. 31.46 Case of persistent dorsal displacement of the soft palate (at rest). A, A 60-cm broncho-oesophageal forceps (arrow) is used to manipulate the soft palate ventral to the epiglottis (topical local anesthetic has been applied). B, The forceps is then used to elevate the epiglottis and view the ventral surface.

FIG. 31.47 Congenital midline defect (“cleft”) of the soft palate.

FIG. 31.48 Unilateral right-sided hypoplasia of the caudal soft palate.
perform athletically to a high level when older, even if surgery is successful.2,52 Surgical repair of soft palate defects is extremely challenging and has a high prevalence of complications and failure. Therefore if signs of severe aspiration pneumonia or a large palatal defect are present, euthanasia of affected foals should be considered as an alternative. Surgical approaches to the soft palate include transoral, pharyngotomy, laryngotomy, and mandibular syphysiotomy, and laryngeal tie-forward has been described to close small palatal defects.49,50-52
Palatal Cysts
These rare lesions usually occur in young horses and may be a cause of abnormal respiratory noise and airway obstruction if they become large or if they disrupt the normal palate- epiglottic relationship. Palatal cysts probably form as the result of the obstruction of mucus-secreting glands within the soft palate, or they may have a traumatic aetiology.54 The presence of palatal cysts predisposes horses to DDSP.
■ Clinical Signs and Diagnosis Clinical signs include respiratory noise (at rest or during exercise), coughing, exercise intolerance, nasal discharge, dysphagia, and signs of aspiration pneumonia. Diagnosis is made by endoscopic examination of the nasopharynx where a raised intrapalatal mass can be seen. Oral endoscopy (as described above) may also be of value. Obtaining an “open-mouthed” straight lateral radiograph (with the incisors held apart with a gag) will cause the soft palate to move dorsally away from the tongue and allows focal thickening of the palate to be visualized more easily than on a standard closed-mouth lateral view. Differential diagnoses include palatal neoplasia and intrapalatal abscesses, the latter being usually associated with intrapalatal foreign bodies or strangles infection. Transendoscopically guided aspiration of the cyst should yield clear, viscous fluid.
■ Treatment Treatment involves surgical excision or laser ablation of the cystic structure, if it is large enough to cause abnormal respiratory noise or airway obstruction. If the cyst is simply drained and some of the lining is left in situ, it is likely to recur.
Neoplasia
Neoplasms of the soft palate are rare. Lymphosarcoma and squamous cell carcinoma occur most frequently, and lesions may vary markedly in appearance. Surgical excision of pharyngeal neoplasms is rarely successful because total excision with wide margins is almost impossible to achieve. Radiotherapy may provide an alternative for treatment of pharyngeal neoplasms but is not widely available for horses.