esophageal FOREIGN BODIES
Dogs and cats occasionally experience lodgment of a foreign body in the esophagus. Although this problem occurs most commonly in young dogs and cats, older animals also may be affected.
Because of their more indiscriminate eating habits, dogs tend to experience foreign body problems more commonly than cats do.Major factors in determining whether a foreign body will pass uneventfully or be retained are its size and its configuration (e.g., rough versus smooth edges, presence or absence of projections, and width). There are four areas of physiologic narrowing in the esophagus: the UES, the thoracic inlet, the heart base area, and
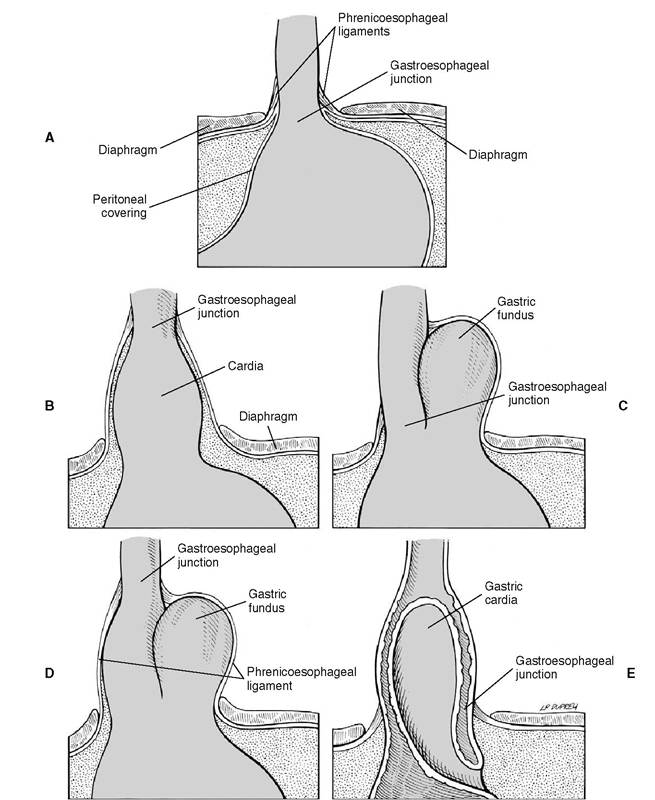
Figure 4-18 A, Diagram of a normal gastroesophageal junction. B-E, Diagrams of hiatal abnormalities: B, sliding or axial hiatal hernia, C, paraesophageal or rolling hiatal hernia, D, combination of sliding and paraesophageal hernia, and, E, gastroesophageal intussusception. (Hedlund CS: Surgery of the digestive system. In Fossum TW, ed: Small animal surgery, ed 2, St. Louis, 2002, Mosby).
the distal esophagus just proximal to the GEJ. Most foreign bodies become impacted in one of the latter three areas in dogs and cats. A variety of foreign bodies can be involved, but in my experience bones and fishhooks are the most common objects found in the esophagus. Needles are the most common foreign bodies found in cats. Although there is potential for a sharp object to perforate the aorta at the aortic arch or through the esophagus to cause a communication to the chest cavity, this is an extremely rare occurrence. Failure of blunt objects to pass through the esophagus spontaneously should raise suspicion that there is an esophageal motility disorder or a pathologic area of narrowing, such as a benign or malignant esophageal stricture.
Clinical signs
Clinical signs related to foreign body impaction in the esophagus are often acute and usually include salivation, which may become bloody, and regurgitation. There also may be odynophagia, dysphagia, forceful retching, lethargy or restlessness, and anorexia. Occasionally, a foreign body remains undetected in the esophagus for a number of days to even weeks. Chronic signs usually include depression, anorexia, salivation, and regurgitation. There also may be clinical evidence of an esophageal foreign body complication such as esophageal perforation with resultant pleuritis, mediastinitis, and pyothorax. Other potential sequelae include esophageal stricture, diverticula, and severe esophagitis.
Diagnosis
The diagnosis of a retained foreign body may be readily apparent from the history. For example, an owner may have observed the patient ingesting a bone found during a garbage foray, reported a missing section of a toy, or found a fishing line attached to a hook dangling from the pet's mouth. In other cases there is no specific relevant history, and in yet others the owner may deny any possibility of foreign body ingestion.
Survey radiographs of the cervical soft tissues and thorax should be the first studies performed because radiopaque objects can easily be localized in most cases. Lateral films of the neck are particularly important in recognizing bone fragments impacted in the cervical esophagus. There may be evidence of an esophageal foreign body. Thoracic radiographs should be carefully evaluated for any evidence of esophageal perforation, including pneumomediastinum and pleural effusion. Also, survey radiographs must be evaluated carefully for evidence of additional foreign bodies that may be less obvious than an easily recognized radiopaque object. Contrast radiography is occasionally necessary to identify radiolucent objects. An iodinated compound (e.g., Gastrografin) should be used instead of barium if there is a possibility of esophageal perforation.
Alternatively, esophagoscopy can be done to confirm or deny suspicions of an esophageal foreign body.A complete blood count should be obtained if the patient is febrile, has aspiration pneumonia, or demonstrates evidence of esophageal perforation.
Treatment
Once a foreign body has been localized, a decision must be made whether to observe for its passage or to remove it endoscopically or surgically. Most esophageal foreign bodies are amenable to endoscopic retrieval. As a rule, any foreign object retained in the esophagus should be removed as soon as possible or, if this cannot be done, at least advanced to the stomach. Although uncommon, the risk of esophageal perforation always exists, especially when a sharp or pointed object is involved. Lodged esophageal foreign bodies can also cause significant pain. In most cases an esophageal foreign body does not have to be removed as a true “emergency” procedure. Exceptions include foreign body impaction in the proximal esophagus that is causing respiratory distress because of tracheal compression and a wedged sharp object such as a bone that is causing significant patient distress. This may be evidenced by groaning, copious salivation, or forceful gagging. If the situation does not require rapid intervention, the patient should be stabilized as needed with intravenous fluids, antibiotics, and pain relievers, and a thorough radiographic assessment should be completed. Ideally, endoscopy should be undertaken within 4 to 6 hours of presentation. Endoscopy is indicated as the initial procedure of choice for all esophageal foreign bodies. If endoscopic equipment is not available, the patient should be referred to an appropriate facility.
If pleural effusion is detected on thoracic radiographs, the chest should be tapped to obtain a sample for cytology, Gram stain, and culture and sensitivity. Pyothorax is best managed with placement of a chest tube for drainage and lavage. Once the patient is stabilized, a thoracotomy is done as soon as possible either alone or in conjunction with endoscopy to remove the foreign body and to evaluate and repair the esophageal wall.
In my experience, it is rare for even bone foreign bodies that have been lodged in the esophagus for several days to weeks to cause complete esophageal perforation.Safe extraction of an esophageal foreign body requires an adequate preliminary evaluation and the selection of proper equipment, including appropriate grasping forceps or snare. Although flexible endoscopes are used most commonly, rigid equipment is also excellent for esophageal foreign body retrieval. A laryngoscope and curved grasping forceps should also be readily available in case their use becomes necessary. As with any type of endoscopic procedure, the patient is maintained under general anesthesia in left lateral recumbency. The endotracheal tube is especially important in preventing tracheal compression as a large foreign body is pulled retrograde through the esophagus and in preventing aspiration of any object that might be inadvertently dropped in the pharynx during retrieval. The endoscope should be passed under direct visual guidance through the pharynx and the UES to avoid striking any foreign body material that may be present in the proximal esophagus and that consequently has the potential for causing mucosal damage. The esophageal mucosa should be carefully evaluated for any foreign body-related damage as the endoscope is advanced. Air should be insufflated to distend the esophageal walls so that visualization is enhanced, but the patient's respiratory status must be monitored while this is being done. Air may be forced around an impacted foreign body and into the stomach, which can lead to significant gastric distention. The distention should be relieved as quickly as possible. In most cases, this can be done by periodically passing the endoscope around the foreign body and into the stomach so that the air can be suctioned. Air insufflation to a perforated esophagus can result in acute respiratory signs and death. The anesthetist is advised to monitor both respiratory character and degree of gastric distention during the procedure.
Successful extraction of a foreign body requires adequate visualization, a firm grasp of the object, and removal with minimal force to avoid further damage. The tip of a flexible endoscope should not be used as a “ramming rod” to dislodge or advance an object because such action could cause significant damage to the endoscope. Once freed, most objects can be pulled back to the tip of the endoscope, and the endoscope and foreign body can then be gently removed simultaneously. Undue force should not be exerted. Gentle manipulation is the rule. If at all possible, pointed objects such as bones and needles should be withdrawn with the pointed end trailing. If there is a sharp- ended object (e.g., toothpick or needle) positioned proximally, the grasping prongs can sometimes be used to cover it so that the esophageal mucosa is protected, or the object can be advanced to the stomach and repositioned so that the sharp end trails. This technique works well when irregular pieces of material such as plastic are involved. Alternatively, objects with sharp or irregular edges can be removed with the aid of an overtube to prevent mucosal damage. After the esophageal foreign body is removed, the entire esophagus should be inspected for damage, and the stomach also should be examined for the presence of any foreign material. There is usually some degree of mucosal laceration at the site of bone impaction in the esophagus. The extent of damage should be carefully evaluated and appropriate medication instituted after the procedure.
If the foreign body cannot be retrieved in a retrograde manner, an attempt should be made to advance it to the stomach.Bones are usually rapidly decalcified by gastric juices, and the remaining fragments will pass through the intestinal tract without incident. If a bone is firmly wedged in the distal esophagus at the time of presentation, it may be best to direct all efforts to advancing it to the stomach rather than risking any problems by pulling it retrograde.
Foreign bodies other than bones that are advanced to the stomach are removed via gas- trotomy. If the foreign body cannot be removed endoscopically and cannot be advanced into the stomach, an esophagotomy should be done. With availability of either rigid or flexible endoscopic equipment, this is rarely necessary.The esophageal wall is invariably damaged by impaction by a bone or another sharp object and subsequent retrieval efforts (Figure 4-19). Most lacerations heal uneventfully, however, and when careful endoscopic techniques are used, surgical intervention is rarely necessary. The mucosa should be carefully inspected once the bone is removed. The degree of damage is usually directly related to the length of time the foreign body was lodged and can be worsened by retrieval efforts. If there is significant erosive damage, treatment for severe esophagitis should be administered as described earlier in this chapter. Pain relief medication also should be given as needed. Effective analgesia may include fentanyl CRI, morphine administered SQ or IM q6h, oxymorphone or hydromorphone, or a fentanyl patch with an injectable opioid administered in conjunction until the patch has been in place long enough for effective blood levels of fentanyl to be reached.
Water is generally offered 12 hours after bone removal, and soft food can be offered at 18 to 24 hours. If there is any concern about esophageal
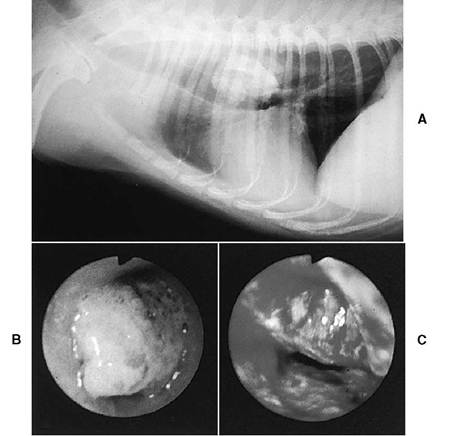
FIGURE 4-19 Esophageal foreign body (pork bone) in a 4-year-old 14-lb mixed-breed dog. The owner had given the bone to the dog as a treat and observed frequent gagging episodes 1 hour later. Radiographs were not obtained at the referring hospital until 3 days after bone ingestion. Clinical signs included intermittent gagging, salivation, nausea, and regurgitation shortly after eating. A, Lateral thoracic radiograph showing a large irregular bone lodged in the esophagus at the heart base. B, Endoscopic appearance of the bone. The bone had been lodged for 3 days before examination. C, The bone was successfully retrieved. Severe esophageal trauma resulted from lodgment of the bone and efforts to remove it. Postendoscopy treatment included sucralfate suspension, intravenous famotidine, subcutaneous amoxicillin, butorphanol for pain, intravenous fluids, and NPO for 36 hours. Several follow-up endoscopies were done over the following 2 weeks to examine for stricture formation. No stricture developed, and the esophagus was grossly normal at 2 weeks. (From Tams TR: Endoscopic removal of gastrointestinal foreign bodies. In Tams TR, ed: Small animal endoscopy, St.Louis, 1990, Mosby-Year Book.)
perforation, thoracic radiographs should be obtained immediately and at 12 and 24 hours after bone removal and compared with preprocedure films. Pneumomediastinum, pneumothorax, or pleural fluid may be present if there has been a perforation. Most patients are discharged from the hospital 1 to 4 days after the foreign body has been removed.
If there has been severe esophageal mucosal damage, periodic endoscopic surveillance during the first 1 to 3 weeks after a bone has been removed is recommended to evaluate for stricture formation. Once-weekly examination is usually adequate. If damage has been particularly severe, the first examination should be done at 3 to 5 days.