HIATAL DISORDERS
The esophageal hiatus is the opening in the diaphragm through which the esophagus passes from the thorax into the abdominal cavity. Anatomic abnormalities of the hiatus may cause symptoms of esophageal disease.
Hiatal lesions may allow hiatal hernia, paraesophageal hiatal hernia, gastroesophageal intussusception, or diaphragmatic hernia to occur. Hiatal hernias are protrusions of the abdominal esophagus, GES, and sometimes a portion of the gastric fundus through the esophageal hiatus into the caudal mediastinum cranial to the diaphragm. Hiatal hernias likely occur more commonly than they are recognized in dogs and cats.Congenital or acquired enlargement of the esophageal hiatus or laxity of the surrounding phrenicoesophageal ligaments may predispose to hiatal hernias. Most hernias are probably congenital. Acquired hiatal hernias may occur secondary to high positive intraabdominal pressure (e.g., blunt abdominal trauma, vomiting) or very negative intrathoracic pressure associated with chronic upper airway obstruction (e.g., laryngeal collapse). Hiatal hernias are seen more commonly in brachycephalic breeds such as English bulldogs and in shar-peis. Although most symptomatic animals with congenital hiatal hernia demonstrate clinical signs by 1 year of age, significant signs may not occur until later. Patients with acquired hernias may develop signs at any age.
Clinical Signs
The most common clinical signs of hiatal hernia are regurgitation, dysphagia, hypersalivation, and vomiting. Hematemesis may occasionally occur.
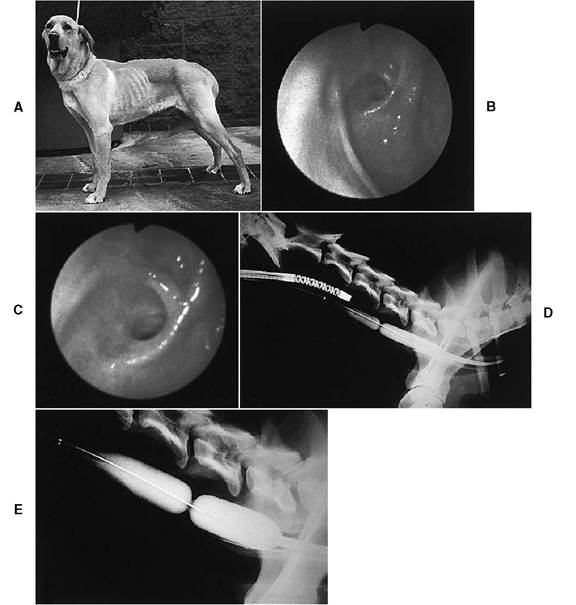
Figure 4-17 Chronic severe esophageal stricture that was not amenable to balloon dilation. A, A 6½-year-old male Labrador retriever that underwent a gastrotomy at an emergency clinic 10 months earlier for suspected foreign body removal.
No foreign body was found. After the surgery there was intermittent vomiting. At 2 weeks the dog began to regurgitate solid food, and at 4 weeks esophagoscopy revealed a stricture in the cervical esophagus. Balloon dilation was recommended, but the dog’s owner chose conservative management, which consisted of feeding a gruel diet. Nine months after the stricture was diagnosed, however, the owner decided to proceed with balloon dilation because he could not maintain the dog’s weight. Weight loss totaled 33 lb since the initial diagnosis. B, Endoscopic photograph of the proximal cervical esophagus. Note the fibrotic band in the near field. An esophageal stricture is visible beyond the band. C, Close-up view of the stricture. There is a fibrotic ring around the stricture, and the narrowed lumen curves on the far side of the stricture. A 7.9-mm endoscope could not be advanced into or through the stricture. D, Under endoscopic guidance, a 15-mm balloon catheter was advanced through the stricture. In this radiograph both the endoscope and the dilated balloon are visible. The stricture is delineated by the narrowed waist in the balloon (just ventral to the proximal border of the fifth cervical vertebra). At 45 psi for 4 minutes the stricture did not dilate. E, The largest balloon available (20 mm dilated) was then used. At 45 psi for 9 minutes the stricture did not dilate because of severe fibrosis. The short stricture is clearly visible on this radiograph. Surgery was later done to resect the stricture, and the dog recovered uneventfully. During the following year the dog gained 33 lb. Histologic examination of the stricture revealed severe fibrosis. It is strongly recommended that balloon dilation be done on esophageal strictures early in their course.Small hiatal hernias may be asymptomatic. Symptoms may be evident only occasionally in animals in which herniation occurs intermittently. In fact, the diagnosis is often difficult to prove in patients because many cases probably involve only sporadic movement. Most hiatal hernia cases are associated with some degree of reflux esophagitis.
Malpositioning or a lack of support of the gastroesophageal sphincter reduces gastroesophageal pressure and leads to gastroesophageal reflux. Most of the clinical signs are related to esophagitis and altered esophageal motility.Diagnosis
Various types of hiatal disorders have been described. These are depicted in Figure 4-18. The most common type of hiatal hernia in dogs and cats is a sliding hiatal hernia with cranial displacement of the abdominal esophagus, gastroesophageal junction, and a portion of the stomach through an enlarged and lax hiatus. Paraesophageal hernias are uncommon. In this type of hernia the gastroesophageal junction remains fixed in the intraabdominal location and the gastric fundus protrudes through a defect in the diaphragmatic hiatus parallel to the esophagus. Gastroesophageal reflux disease is less commonly associated with paraesophageal hernias because the LES remains functional and in a normal intraabdominal position.
Gastroesophageal intussusception is a rarely encountered syndrome. Gastroesophageal intussusception results when the gastric cardia invaginates into the terminal esophagus. The gastroesophageal sphincter does not move cranial into the thorax as occurs with a hiatal hernia. Entrapment of the stomach in the esophagus may result in acute esophageal obstruction.
Survey thoracic radiography may confirm the diagnosis in some cases. Findings include an increased opacity in the caudal dorsal mediastinum caused by presence of the stomach in the thoracic cavity. Positive contrast esophagrams may reveal displacement of a portion of the stomach into the thorax. Contrast radiography is used to determine the location of the GEJ and to evaluate the mucosal pattern of the lower esophagus. Compressing the abdomen during radiography in patients with a suspected hernia may help force part of the stomach into the thorax and increase the likelihood of obtaining diagnostic films.
Occasionally the diagnosis is made at endoscopy.
Endoscopy may confirm gastroesophageal intussusception, in which gastric rugal folds are seen bulging into the lumen of the distal esophagus. A careful assessment of the esophageal mucosa, the GEJ, and the stomach is important in the determination of the treatment plan. Finding reflux esophagitis helps raise suspicions of a hiatal disorder. Endoscopic findings of cranial LES displacement and a large esophageal hiatus, in conjunction with appropriate clinical signs, is suggestive of a sliding hiatal hernia. When the endoscope is passed from the esophagus into the stomach, it should be retroflexed, after the stomach is insufflated with air, to view the LES from the gastric side. With gastric insufflation there may be cranial displacement of the LES and cardiac region of the stomach through a weakened or enlarged esophageal hiatus.Treatment
Surgical correction is indicated in patients with a symptomatic hiatal hernia. Fundoplication procedures have been described. Other techniques include diaphragmatic hiatal reduction and plication, esophagopexy, and left-sided fundic gas- tropexy. Medical management for esophagitis is instituted as soon as the diagnosis is made. If surgery is not corrective, medication may have to be continued indefinitely in order to control symptoms of reflux esophagitis. Medical management (H2-receptor antagonist, prokinetic therapy, and a low-fat diet) without surgery is often useful in patients with mild symptoms related to intermittent herniation. A PPI (e.g., omeprazole) is recommended over an H2-receptor antagonist for moderate to severe esophagitis (see section earlier in this chapter on management of esophagitis).