Esophagus
The radiographic features that are associated with esophageal disease are listed in Table 1.7. Radiography is central to the diagnosis of megaesophagus. It allows rapid identification of the affected segments and also assessment of the degree of esophageal dilation.
A small amount of air in the esophageal lumen can be expected in dogs that are panting or nervous during the radiographic procedure or those under sedation or general anesthesia (Figure 1.16). The presence of ventral pulmonary consolidations and pleural fluid on thoracic radiographs should raise the suspicion of mediastinitis and /or aspiration pneumonia (Figure 1.17).Esophagography with barium sulfate creams or suspensions is indicated when esophageal disease is suspected and survey thoracic radiographs are unremarkable. In the presence of a pneumomediastinum or mediastinitis, aqueous iodine agents may be used orally, but if aspirated they may induce pulmonary edema due to their hypertonic nature. The goal of the esophagram should be to determine the location and type of esophageal abnormality. The esophagram may, however, only provide limited information since it can only differentiate intraluminal lesions from intramural or peri-esophageal ones. If the liquid barium suspension does not show a stricture, a barium-coated food bolus should be fed.
Peri-esophageal or intramural lesions that do not alter the esophageal mucosa may go unnoticed during conventional endoscopy of the esophagus. In contrast, echoendoscopy allows the detection of intramural neoplasms and extramural spaceoccupying lesions of the mediastinum that may compress the esophagus. The author has diagnosed both esophageal tumors and periesophageal lesions using echoendoscopy in both dogs and cats (Figure 1.19).
1.3.3.1 Generalized esophageal dilation
Generalized megaesophagus can be visualized by the presence of a dilated, gas-filled lumen along the entire length of the esophagus on survey radiographs.
The tracheal stripe sign is present due to superimposition of the esophageal and tracheal walls and the longus colli muscle ventral to the 5th and 6th thoracic vertebrae (Figure 1.18). The caudodorsal thorax may also appear hyperlucent due to the presence of air in the esophagus. Differential diagnoses for generalized dilation of the esophagus are numerous. In young animals megaesophagus is most commonly idiopathic. In adults, central nervous system and neuromuscular disorders, such as myasthenia gravis, feline dysautonomia, polyneuritis, or polymyositis are more likely to be the cause. Endocrinopathies such as hypothyroidism or hypoadrenocorticism and toxicities, trauma, tetanus, and thymoma are additional differential diagnoses. Dilation can also be seen with hiatal hernias and gastric volvulus. Furthermore, an air-filled megaesophagus can be seen in cats with lower airway disease causing dyspnea and aerophagia. Mechanical causes of generalized dilation can be due to foreign bodies and strictures located either intraluminally, murally, or peri- esophageally.a
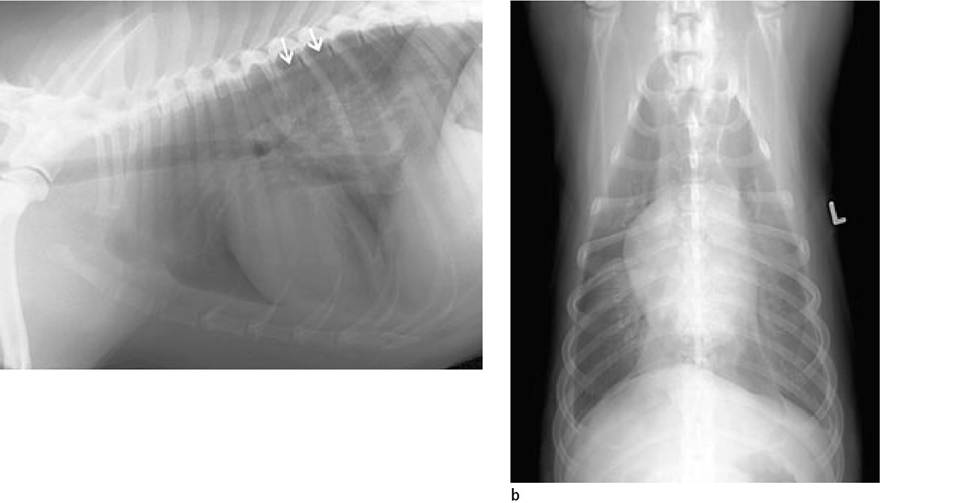
Figure 1.17a, b:
Perforated esophageal foreign body. Lateral (a) and ventrodorsal (b) thoracic digital radiographs of a 2-year-old American Staffordshire Terrier that presented in lateral recumbency and shock with severe abdominal pain. A mixed radiopacity in the region of the caudal esophagus is seen. Additional findings include the presence of pleural fluid and pneumothorax. Note the retracted border of the caudal lung lobe (arrows) with free air surrounding it dorsally. Differential diagnoses include trauma, pulmonary disease, and mediastinitis. A piece of rawhide was removed surgically from the esophagus, which was perforated.
Figure 1.18:
Megaesophagus. Lateral thoracic radiograph showing generalized megaesophagus. The esophagus is air-filled, the dorsal thorax appears hyperlucent, and the thin walls of the esophagus can be identified (arrows).
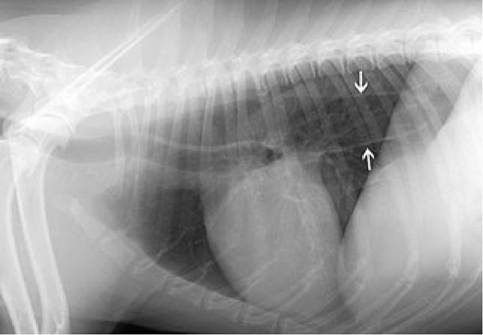
Table 1.7: Radiographic signs of esophageal disease
■ Increased visibility
■ Tracheal stripe sign
■ Dilation with air, fluid, or food
■ Pneumomediastinum
■ Mediastinal space-occupying lesion
■ Ventral displacement of the trachea and heart
■ Increased lucency of the dorsal thoracic region
■ Ill-defined pulmonary consolidations located ventrally
■ Pleuralfluid

b
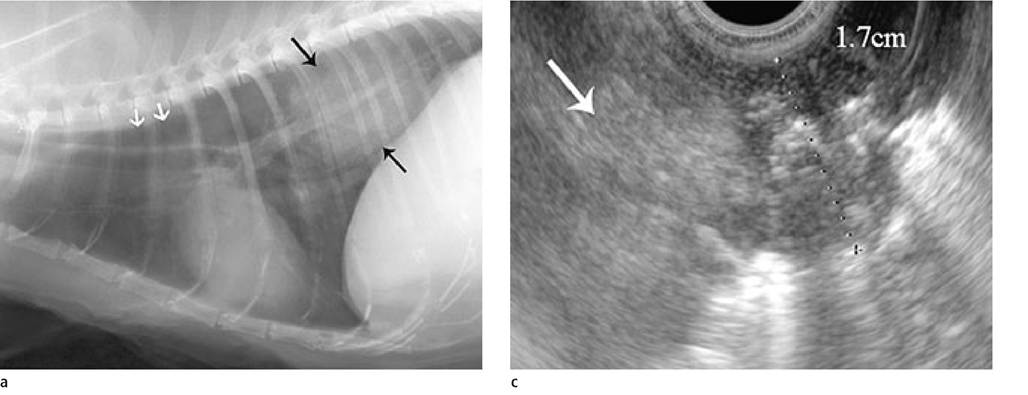
Figure 1.19a-c:
Esophageal mass.
(a+b) Lateral and ventrodorsal thoracic radiographs of a 16-year-old European Short Hair cat that presented with chronic dyspnea, anorexia, and weight loss. A round soft tissue opacity in the region of the caudal mediastinum can be seen (black arrows). Note the segmental dilation of the esophagus cranial to the lesion (white arrows). Additional pulmonary nodules are seen in the right caudal lung lobe. Possible origins of the mass are esophageal intraluminal, mural, or periesophageal as well as pulmonary. Differential diagnoses include neoplasia, granuloma, abscess, and esophageal foreign body.
(c) Esophageal echoendoscopy showed a nodular infiltration with disruption of the esophageal wall layering of 1.7 cm in diameter (distance shown: dotted line). The lesion has a complex echostructure that includes hyperechoic foci with reverberation echoes (gas bubbles in the mass). A separate portion of the lesion (arrow) was 2 cm in diameter, homogenous, and had broken through the esophageal wall to invade the periesophageal region. Multiple intralesional vessels with arterial flow could be shown by Doppler ultrasound. Histological diagnosis: esophageal carcinoma.
1.3.3.2 Segmental esophageal dilation
Localized or segmental esophageal dilations may be located anywhere along the esophagus.
(Figure 1.19). Potential causes include foreign bodies, segmental hypomotility, esophagitis, diverticuli, hernias, foreign bodies, acquired strictures, and mural or extramural lesions due to inflammation or neoplasia. Foreign bodies and strictures may also present radiographically as mediastinal soft tissue opacities rather than focal dilations. Common sites of esophageal strictures are the thoracic inlet, the base of the heart, and at the gastroesophageal junction. In young dogs and cats, esophageal strictures are often due to vascular ring anomalies such as a persistent right aortic arch. These are recognized by a ventral displacement of the trachea in the cranial thorax and varying degrees of esophageal dilation cranial to the base of the heart. Barium esophagrams are contraindicated in the presence of large fluid- or food-filled esophageal dilations. Angiography should be performed to definitively rule out a vascular ring anomaly in any puppy or kitten with suspected vascular ring anomaly.1.3.4