Oropharynx
Patients with dysphagia and regurgitation on the one side or vomiting on the other are approached differently depending on which sign predominates. Dysphagia and regurgitation can often be differentiated from vomiting by a thorough history and physical examination.
Regurgitation can occur with both oropharyngeal and esophageal disorders. Patients with exaggerated swallowing attempts, gagging, or pain when drinking or swallowing food, however, often have oropharyngeal dysphagia. Regurgitation is characterized by the passive retrograde expulsion of undigested food, whereas animals with vomiting show a forceful ejection of partially digested food with a marked abdominal effort.Survey radiographs should always be performed to rule out structural abnormalities, such as fractures of the hyoid apparatus or radiopaque foreign bodies in the oropharyngeal region. The pharyngeal and laryngeal regions and the entire esophagus should be included in both lateral and ventrodorsal views. Thoracic radiographs in two planes are strongly recommended in animals with dysphagia to rule out the presence of aspiration pneumonia.
a
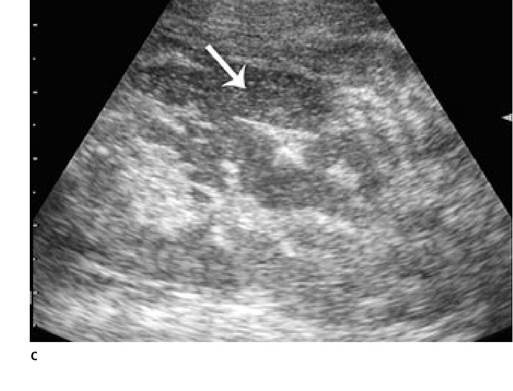
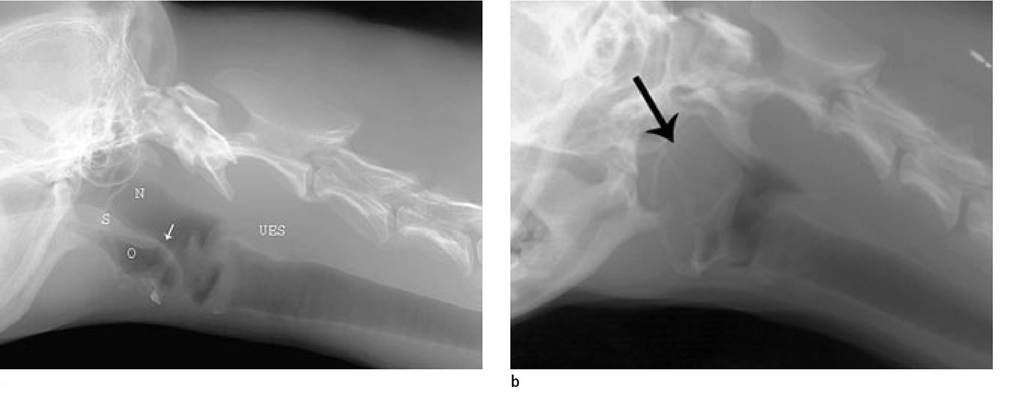
Figure 1.9a-c:
Imaging of the pharyngeal region.
(a) Normal pharynx. N=nasopharynx, O=oropharynx, S=soft palate, UES=upper esophageal sphincter, arrow=epiglottis
(b) Oblique lateral radiograph of the pharyngeal region in an 11-year-old Coton de Tulear that presented in respiratory distress. In this dog, the nasopharynx is compressed and the pharynx is displaced dorsally (arrow) due to an opaque soft tissue space-occupying lesion.
(c) Ultrasonographic image of the soft tissue lesion from the patient shown in Figure 9b. A complex cavitary mass with fluid-filled pockets (arrow) in the center was identified.
The mass was surgically removed and diagnosed as an abscess.1.3.2.1 Structural abnormalities
Survey radiographs should be inspected for increased soft tissue opacities in the pharyngeal, retropharyngeal, or cervical region, which may impinge upon or displace the airways of the oropharynx, nasopharynx, larynx, or trachea (Figure 1.9). Soft tissue space-occupying lesions may be due to lymphade- nomegaly, abscesses, polyps, neoplasias, or foreign body granulomas. Radiopaque foreign bodies may be immediately evident; however, radiolucent ones may only appear as spaceoccupying lesions of soft tissue opacities. The presence of gas within soft tissues can be seen with abscesses or percutaneous foreign body penetration.
Ultrasonography can be used to determine the origin of soft tissue swellings of the neck and retropharyngeal region. High frequency linear array transducers are best for the examination of the cervical region since most structures are very superficial. However, curved-linear array transducers are also adequate.16 The thyroids and salivary glands and the retropharyngeal or mandibular lymph nodes can all be enlarged due to inflammation, abscessation, or primary or metastatic neoplasia. Perforating foreign bodies can be recognized as hyperechogenic structures of varying size with acoustic shadowing (Figure 1.10).17 Pinpoint hyperechogenic structures with reverberation echoes signal the presence of air and should not be mistaken for foreign material. Lingual foreign bodies and abscesses can also be diagnosed with ultrasound using a ventral, inter-mandibular approach (Figure 1.11). 18
MRI and CT are excellent alternative modalities for examining the cervical region, screening for foreign bodies, and for determining the origin of complex masses.
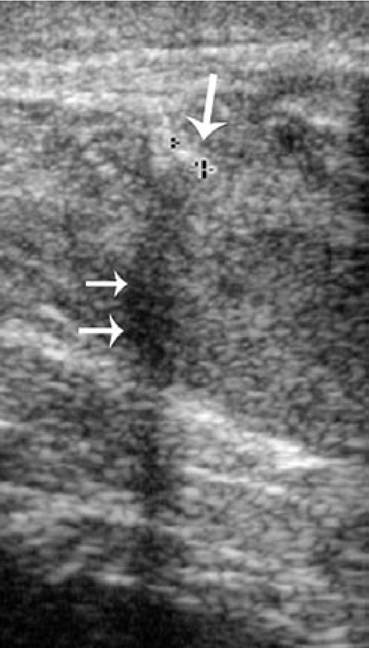
Figure 1.10:
Foreign body in the cervical region. Ultrasound image of the cervical region of a dog with a chronic draining fistula.
A 3-mm long, hyperechoic, linear structure (arrow) with distinct acoustic shadowing (two smaller arrows) was detected in the soft tissue. Diagnosis: wood splinter with abscess.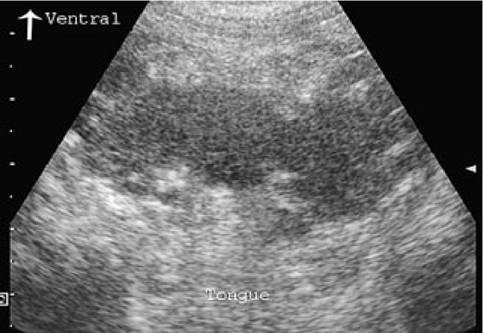
Figure 1.11:
Lingual foreign body. Ventral transverse ultrasound image of the caudal oral cavity at the level of the angular processes of the mandible in a dog with acute dyspnea, cyanosis, and pharyngeal swelling. A space-occupying lesion with a complex echotexture at the base of the tongue was identified. The mandibular rami can be seen as the anechoic structures on either side of the tongue. The lesion was explored surgically and found to be an abscess most likely to be due to a perforated foreign body.
1.3.2.2 Functional Disorders
Survey radiographs of animals with neuromuscular causes of oral, pharyngeal, and cricopharyngeal dysphagia are generally unremarkable. Thoracic radiographs are strongly recommended to rule out the presence of aspiration pneumonia, which can occur with cricopharyngeal dysphagia. Lateral radiographs of the oropharyngeal and cervical region are required to rule out structural abnormalities. Focal accumulations of gas may be detected in the proximal esophagus due to either esophagitis or functional disorders. The presence of an open, air-filled upper esophageal sphincter and an air-filled esophagus can be seen with cricopharyngeal chalasia since the sphincter cannot maintain a positive resting pressure (Figure 1.12). However, the finding of air in the esophagus in sedated or anesthetized animals is not uncommon and should be interpreted with caution.

Figure 1.12:
Megaesophagus. Lateral radiograph of the pharynx in a 4-year-old German Shepherd with regurgitation due to megaesophagus. The upper esophageal sphincter is open and air-filled (arrow). The cervical esophagus is also dilated and air-filled.
The presence of air in these structures signals the possibility of either a functional or structural disorder. The diagnosis in this dog was chalasia due to myasthenia gravis. (Image courtesy of Dr. Johann Lang, Division of Radiology, Faculty of Veterinary Medicine, University of Bern, Switzerland.)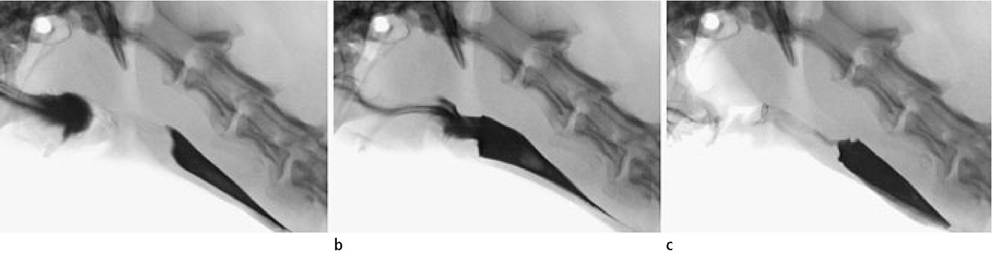
a
Figure 1.13a-c:
Barium swallow in a normal dog. Static digital fluoroscopic images of a barium swallow in a normal dog. The pharyngeal (a), cricopharyngeal (b), and esophageal (c) phases are shown. (Images courtesy of Dr. Johann Lang, Division of Radiology, Faculty of Veterinary Medicine, University of Bern, Switzerland.)
When survey radiographic examination is unremarkable, a contrast study performed with either fluoroscopy, serial radiographic exposures, or static radiographic images is indicated. However, without the possibility of fluoroscopy and dynamic acquisition of images, the details of bolus formation and passage can usually not be observed with static radiographic images alone.
Swallowing studies are generally performed in conscious animals since sedation may inhibit swallowing or increase the risk of aspiration. Initially, a liquid contrast agent should be administered into the oral cavity. Liquid barium sulfate suspensions (45-85% w/w) are preferred for barium swallows and 5-20 ml of the suspension is administered depending on the size of the animal. If the animal has a history of having difficulty swallowing food but not liquids, the study should be repeated using barium-coated food. With the animal in lateral recumbency, the act of swallowing should be observed immediately with fluoroscopy and recorded on video tape or using rapid serial radiography (Figure 1.13).
Retention of contrast medium in the oral cavity and its absence in the pharynx and esophagus can be observed in animals with oral dysphagia. When direct damage to the tongue is ruled out, a brain stem lesion (hypoglossal nerve) may be suspected as the underlying cause.
Retention of substantial amounts of contrast medium in the pharynx following swallowing of the bolus is observed in pharyngeal phase dysphagia. Laryngeal aspiration may also be observed. When mechanical obstruction can be ruled out, idiopathic neuromuscular dysfunction is usually the cause.Cricopharyngeal dysphagia is characterized by retention of contrast medium in the pharynx with reflux of the contrast medium into the oro- or nasopharynx, aspiration into the larynx, retention in the cervical esophagus, and hypertrophy or distortion of the upper esophageal sphincter. Often, very small amounts of contrast medium are observed to pass through the hypertrophied sphincter. This disease is often seen in young dogs and is called cricopharyngeal achalasia (Figure 1.14). In contrast, in patients with cricopharyngeal chalasia, the upper esophageal sphincter remains open and contrast can be observed moving freely between the esophagus and pharynx through an open sphincter (Figure 1.15). This should alert the clinician to a neuromuscular disorder such as myasthenia gravis.
Figure 1.14:
Cricopharyngeal achalasia. Static digital fluoroscopic image of a barium swallow in a 5-month-old American Staffordshire Terrier with dysphagia and failure to thrive. The puppy showed clinical signs of cricopharyngeal dysphagia and could only swallow food intermittently. There is retention of contrast in the pharynx. Fluoroscopically, pharyngeal contractions were evident and the contrast bolus was repeatedly advanced towards a closed upper esophageal sphincter (black arrow). Occasionally, some contrast material could pass through the sphincter and was visible in the esophagus (white arrow). Diagnosis: cricopharyngeal achalasia.
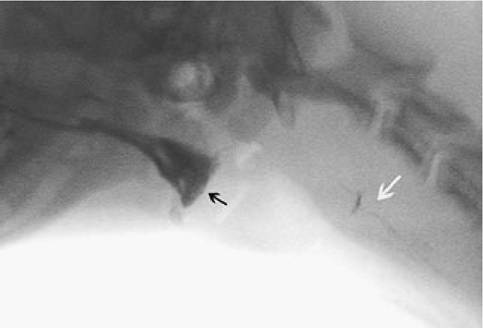
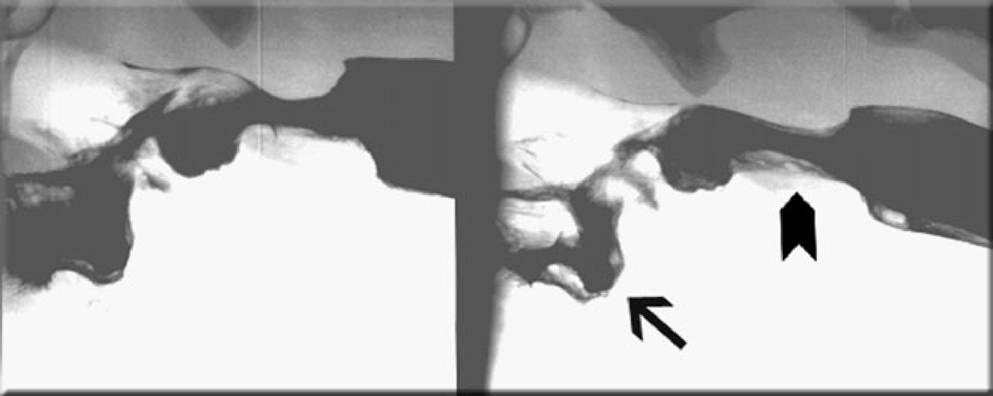
Figure 1.15:
Barium swallow in a dog with myasthenia gravis. This figure shows a barium swallow in the same dog as shown in Figure 1.12. Note that there is retention of contrast in the pharynx (arrow) and the upper esophageal sphincter remains open (arrow head) and filled with contrast. (Image courtesy of Dr. Johann Lang, Division of Radiology, Faculty of Veterinary Medicine, University of Bern, Switzerland.)
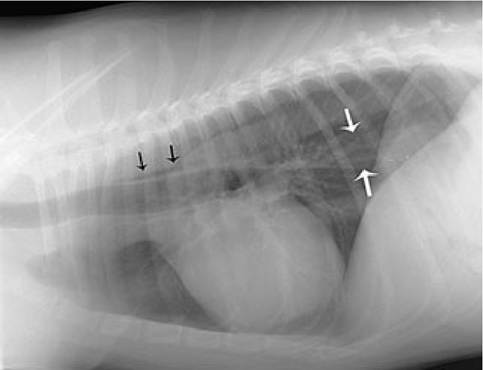
Figure 1.16:
Radiographic appearance of the esophagus in normal dogs. Lateral thoracic radiograph of a normal dog. Dogs and cats that are nervous and panting when radiographs are taken may have small amounts of air or fluid in the esophagus. Air is typically seen just cranial to the base of the heart (black arrows). The caudal esophagus may appear as a soft tissue opaque band (between white arrows) between the aorta and caudal vena cava.
1.3.3