Stomach
Following the clinical history, physical examination, and laboratory data base, survey radiographs and ultrasound are important diagnostic tools in dogs and cats with vomiting.
Radiography is a rapid method for assessment of extra-abdominal structures, the abdominal wall, diaphragm, vertebrae, and also the detection of obstructive lesions and radiopaque foreign bodies. The significance of the presence of radiopaque material in the gastrointestinal tract must be correlated to the type of foreign body, its size, and the clinical signs of the animal. Regardless of inherent diagnostic limitations, lateral and ventrodorsal survey radiographs should always be performed prior to contrast studies, ultrasonography, or endoscopy.Prior to both radiography and ultrasonography, animals should be fasted for a minimum of 12 hours, though this may not be possible in emergency situations. Dependent upon the radiographic findings, a combination of ultrasonography and endoscopy may be deemed necessary. Ultrasonography should always be performed prior to endoscopy or barium studies since the presence of excessive intestinal gas or barium sulfate will create ultrasound artefacts that prohibit examination of the abdomen.
For the ultrasonographic evaluation of the gastrointestinal tract, high frequency curved linear array or sector transducers are recommended. High frequency transducers have the best resolution for evaluation of gastrointestinal wall layers. Moreover, linear transducers allow the best resolution of small intestinal layering and echogenicity (Figure 1.20). A 5- to 7.5-MHz transducer is adequate for large dogs whereas frequencies of
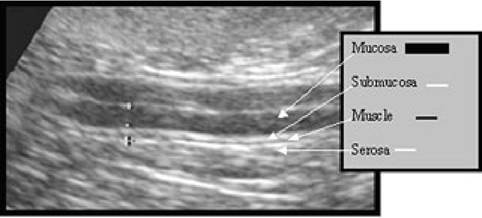
Figure 1.20:
Intestinal wall layering. Ultrasound image using a 7.5-MHz linear array transducer of a normal jejunal segment in a dog showing the normal wall layering.
>7.5 MHz are best for smaller animals. The ultrasound examination of the stomach and small bowel should include an assessment of the peritoneum, mesentery, and lymph nodes.
Gastrointestinal contents, especially air or barium, may hinder the ultrasonographic examination. Even under ideal conditions, it is difficult to examine the entire stomach during abdominal ultrasound, especially in large dogs or when the stomach is greatly dilated. In order to improve imaging of the stomach, it can be filled with small amounts of water by either allowing the animal to drink or by administering it by stomach tube. This may facilitate the examination of the gastric wall, which may be difficult when the stomach is contracted.
Ultrasonographic evaluation of the gastrointestinal tract should include assessment of the wall thickness, layering, and symmetry, localization and distribution of thickening, motility, and luminal content.
1.3.4.1 Gastric dilation and volvulus
Severe gastric distension may be caused by excess quantities of gas, food, and fluid in the stomach. If the stomach is dilated and food-filled but positioned normally, dilation is probably the most likely diagnosis (Figure 1.21a). Severe dilation together with displacement of the stomach is a sign of gastric volvulus. In gastric volvulus, the stomach appears compartmentalized or segmented with band-like soft tissue opacities apparent between the gas-filled segments (Figures 1.21b, c and d). The radiographic localization of the pylorus is the key to the diagnosis. The pylorus is usually displaced dorsally and to the left. A right lateral radiograph is usually sufficient to make the diagnosis of gastric volvulus, and the pylorus will be air-filled and located dorsally. The spleen is also often enlarged due to circulatory compromise and may also be displaced. The esophagus and small intestines may often appear dilated and air-filled. Gastric volvulus without severe distension may also
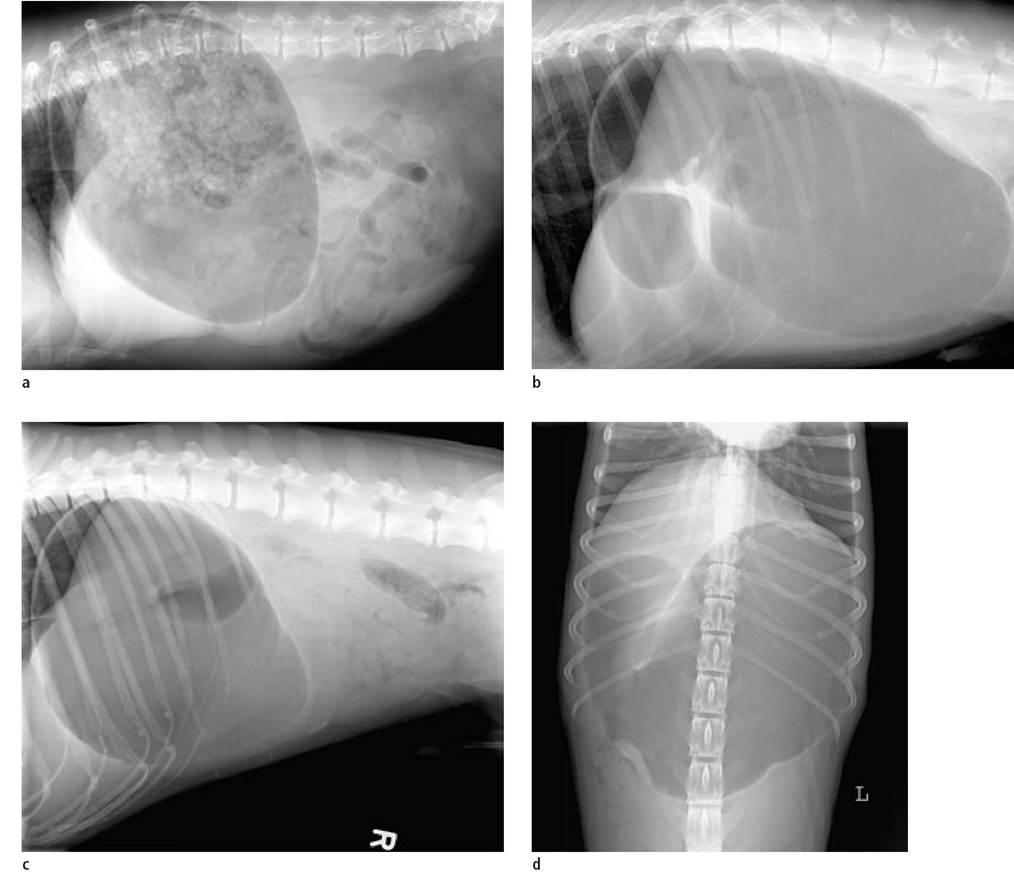
Figure 1.21a-d:
Gastric dilation, and gastric dilation and volvulus.
(a) Gastric dilation without volvulus. The gastric fundus is still located Craniodorsally.
(b) Gastric dilation and volvulus. The gastric fundus is located caudoventrally, the pylorus craniodorsally. Folds in the stomach create the appearance of compartmentalization.
(c+d) 360° gastric torsion. The fundus appears to be in its normal position. Note the soft tissue band between the body and pylorus in the ventrodorsal image. A stomach tube could not be passed in this dog and the 360° nature of the torsion was confirmed surgically.
occur. Therefore, it is always important to interpret the radiographic findings in the light of the clinical findings. Dogs with previous gastropexy that present with recurrent vomiting may have some degree of gastric distension and displacement radiographically.
1.3.4.2 Gastric causes of chronic vomiting
Primary gastric causes of chronic vomiting include diffuse inflammatory infiltration, neoplasia, foreign body, polyps, ulcers, pyloric hypertrophy, and delayed gastric emptying. Their diagnosis can be challenging and often requires a combination of radiography, ultrasound, and endoscopy. Thickening of the stomach wall is commonly associated with chronic vomiting and is probably one of the most commonly over-interpreted findings on survey radiographs. Superimposition of fluid with the stomach wall may lead to the impression that the wall is thickened. The same is true for fluid within the small intestines. Thickening of the rugal folds in chronic gastritis is difficult to appreciate on survey radiographs for the same reason. Liquid barium contrast studies or preferably, ultrasonography, is required to confirm a radiographic suspicion of wall thickening. Negative contrast studies can be obtained by filling the stomach with air and performing radiographs in various posi- tions.1 This technique may allow detection of focal wall infiltrations. However, because both negative and positive contrast radiographic studies of the stomach are very time consuming and can be difficult to interpret, ultrasound is generally the method of choice for imaging the stomach wall.
Ultrasonographically, thickening of the stomach wall can be characterized as focal or diffuse, concentric or asymmetric. Attention to technique is necessary since oblique scanning of the stomach wall may lead to an artificially increased thickness and disruption of wall layering.19 Therefore, scanning in multiple planes perpendicular to the stomach wall is necessary to avoid this error. Focal thickening with disrupted wall layering may be caused by neoplasia, granulomas, and ulcers. Generalized thickening is more commonly seen with inflammatory disease but can also occur with diffuse neoplastic infiltration. Thickening of the gastric wall is considered to be present when the wall thickness is greater than 5 mm in dogs and 3 mm in cats.
Radiopaque gastric foreign bodies such as ingested bone fragments are the most frequent incidental findings. If the object is still located in the stomach 1-2 days after the initial examination, its presence should be further investigated. Radiolucent foreign bodies can be identified by endoscopy, ultrasound, or contrast studies. Only a small amount of barium should be administered, or a double-contrast gastrogram should be performed since large volumes of barium can obscure both wall infiltrates and foreign material. Alternatively, a negative contrast gastrogram can be performed.
Chronic pyloric obstruction can occur either due to narrowing of the lumen because of wall infiltration or mechanical blockage of the orifice. Survey radiographs usually show some degree of gastric distension. Barium studies may help to identify pyloric obstructive disease. However, differentiating hypertrophic pyloric stenosis from inflammatory infiltrates or neoplasia is often difficult since they all lead to a narrowing of the pyloric orifice due to annular thickening, and they all have a similar appearance radiographically. Detecting intraluminal filling defects in the area of the pylorus is also possible. These may be due to foreign bodies, polyps, or severe inflammatory infiltrates and neoplasms.
The gastroduodenal junction can be examined ultrasonographically in dogs. Congenital hypertrophic pyloric stenosis and chronic hypertrophic gastropathy have a similar ultrasonographic appearance. Circumferential thickening (>3 mm) of the muscularis layer can be recognized by a hypoechoic layer that appears like a ring in cross-section. In chronic hypertrophic gastritis the mucosa can also be thickened. The strong peristaltic contractions against the thickened pylorus can also be observed. These contractions fail to propel food through the pylorus and a reflux movement of the gastric contents can be seen and recorded on video tape.
Gastric ulcers will lead to a disruption of the mucosal surface and they usually cannot be diagnosed using survey radiographs alone. Their diagnosis requires a contrast study, ultrasound, or endoscopy. It is important to remember that ulceration of the stomach wall has various causes and that the stomach wall should be thoroughly investigated, preferably with ultrasound, for evidence of underlying disease. Ultrasonographically, benign ulcers appear as a localized wall thickening. Mucosal craters with an irregular surface and the adherence of gas bubbles may also be detected.20 Unfortunately, the presence of air, food, or lack of ultrasound beam penetration in large or obese dogs may make their detection difficult. Benign ulcers may appear similar to those associated with neoplasms. When the thickened stomach wall shows a loss of wall layering, gastric neoplasia should be suspected.
Gastric neoplasia is generally only diagnosed on survey radiographs when it is large enough and when the proliferative tissue is projected into the air-filled lumen. Lack of air in the stomach may cause mural lesions to be overlooked. Diffuse stomach wall infiltrations are even more difficult to diagnose radiographically. Generalized wall thickening may be seen with a number of conditions including chronic hypertrophic gastritis, eosinophilic gastritis, fungal infiltrations, and malignant histiocytosis.
Both diffuse and localized gastric wall infiltrations may be detected with ultrasound, which often eliminates the need for contrast studies. Neoplasms can be recognized during abdominal ultrasound by observing thickening of the wall and the disruption of the normal wall layering, which is usually of decreased echogenicity and may create the appear-ance of pseudolayering.21 Also, regional lymph nodes are often enlarged. Gastric lymphoma occurs in both dogs and cats and causes a generalized, hypoechoic thickening of the stomach wall with loss of wall layering.22
Tumors with increased vascularity can be diagnosed by Doppler ultrasound. However, no larger studies have been performed in dogs and cats describing the vascular patterns of neoplastic versus inflammatory gastric wall infiltrations. Contrast-enhanced ultrasound may have future potential in the characterization of gastric tumors but further studies are needed.
Ultrasound-guided percutaneous fine-needle aspiration or biopsy of the gastric wall can be performed in order to differentiate neoplastic and inflammatory infiltrates. The author performs percutaneous tissue sampling when the gastric wall lesion is located submucosally, rendering endoscopic biopsy collection largely unsuccessful. Fine-needle aspiration can be performed with a 20-gauge needle or biopsies can be taken with an 18-gauge spring-loaded biopsy device. When the gastric wall is thicker than 2 cm, a true-cut spring-loaded biopsy is feasible.
Endoscopic ultrasound represents a new and alternative imaging modality for gastric lesions. High-quality video endoscopes provide both optical and sonographic imaging of the gastrointestinal wall and of the perigastric organs. The author believes that echoendoscopic imaging of the stomach allows a more thorough examination than transabdominal ultrasound alone (Figure 1.22). However, more work needs to be performed in cats and dogs in order to establish the role of echoendoscopy in veterinary gastroenterology.
1.3.4.3 Diagnosis of delayed gastric emptying
Mechanical obstruction due to pyloric foreign body, gastric neoplasia, pyloric hypertrophy, antral mucosal hypertrophy, and antral polyps can generally be ruled out with a combination of radiography, ultrasound, and endoscopy. The diagnosis of other causes of delayed gastric emptying can be more difficult. Sequential radiographic imaging methods are often required. These can be time consuming and require restraint or sedation, both of which can potentially affect the results. Radiographic methods employ either indigestible radiopaque markers, barium meals, or liquid contrast agents (barium or iodine-containing).15,23,24,25 However, radioscintigraphy is now considered the method of choice for detection of delayed gastric emptying.15,23
It has been shown that water intake, meal size, food type (dry vs. canned), and kibble shape can influence the rate of gastric emptying in cats.26,27 The rate of gastric emptying in normal animals depends mainly on the state of filling of the stomach and the type of contrast medium used as well as stress and sedation in the patient. Animals should be kept in a quiet environment during the study and should not be sedated if possible. Iodine-containing contrast media have a much more rapid passage time than barium sulfate. Furthermore, a low dose of contrast medium may lead to longer emptying times. The dose of barium suspensions is 6 ml/kg in dogs and 10 ml/kg in cats and should be administered when the stomach is empty. Barium sulfate should be present in the duodenum by 15 minutes in the dog and by 5 minutes in the cat. The stomach should be free of barium after 1 to 4 hours in the dog and after 20 minutes in the cat. The presence of food in the stomach prior to the examination will delay gastric emptying for up to 15 hours or even more (longer for dry than moist food).
1.3.5