Evaluation of Immunologic Response in Horses
Lais R.R. Costa
Assessment of immune response encompasses in vivo, in vitro, and ex vivo measurements of immune function and can be divided into three categories: (1) assays for characterizing the adequacy of the immune response when an immunodeficiency
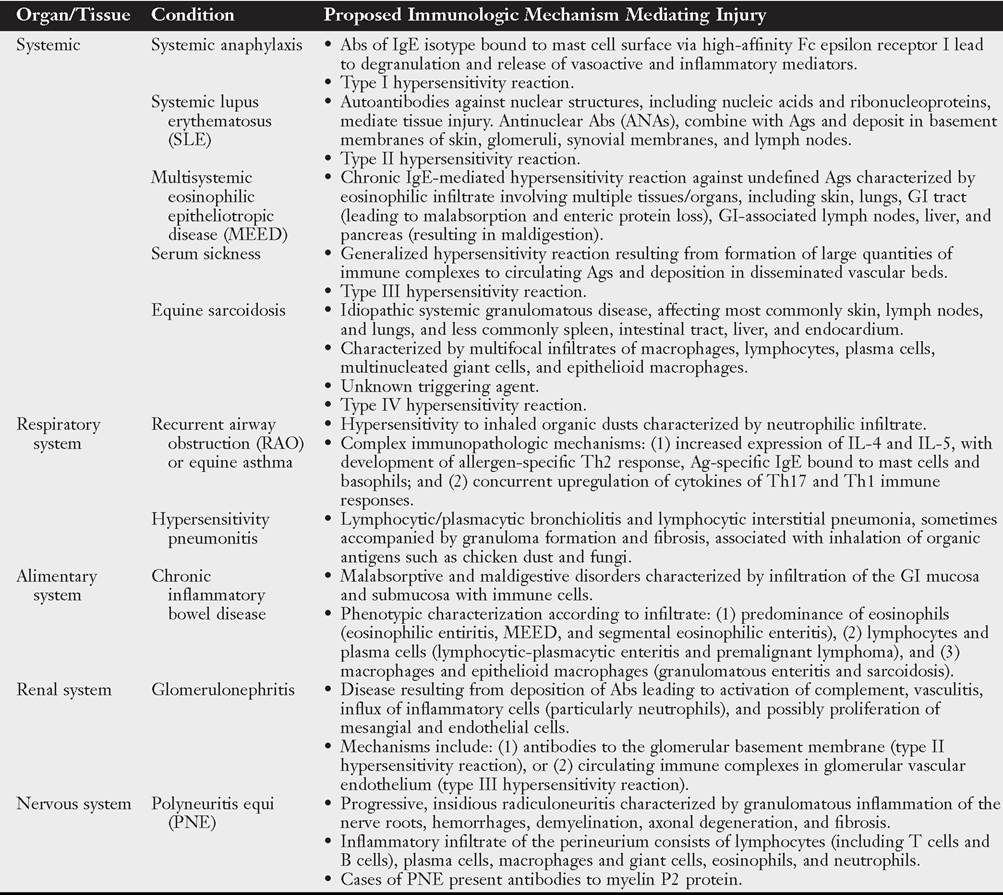
■ TABLE 53.4
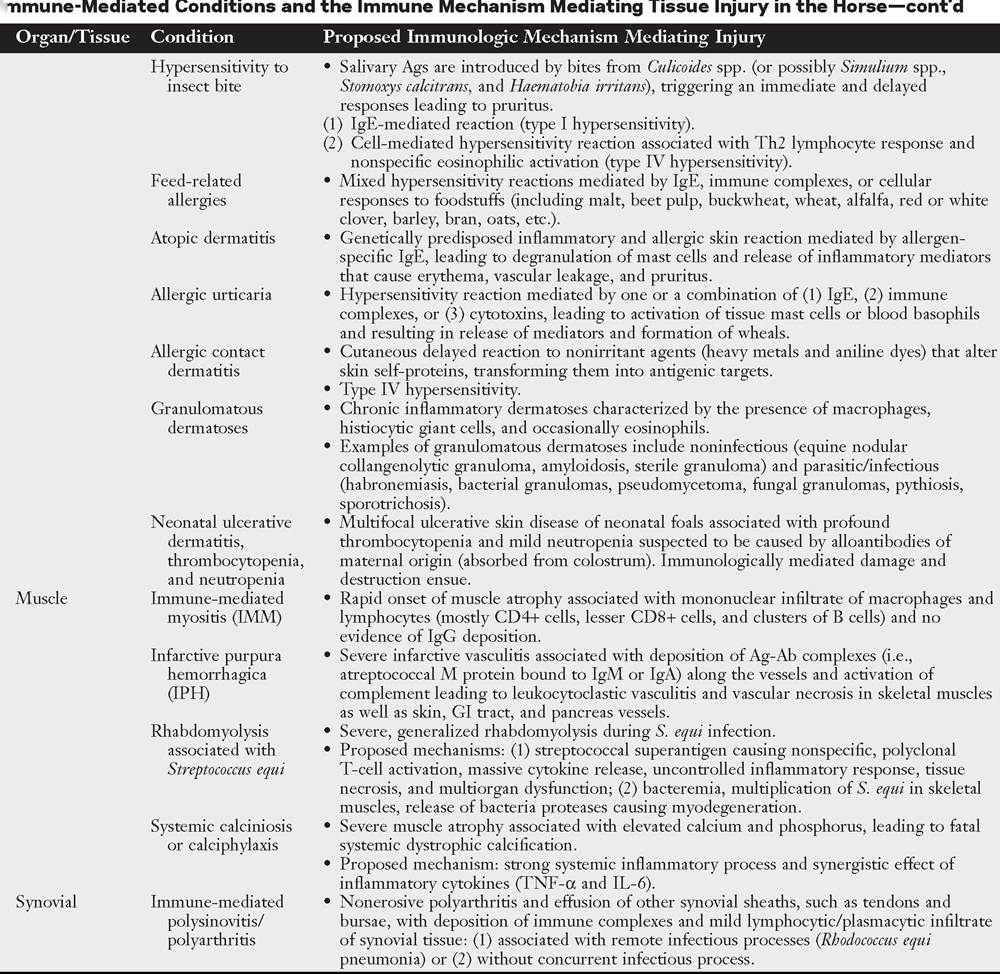
Immune-Mediated Conditions and the Immune Mechanism Mediating Tissue Injury in the Horse
■ TABLE 53.4
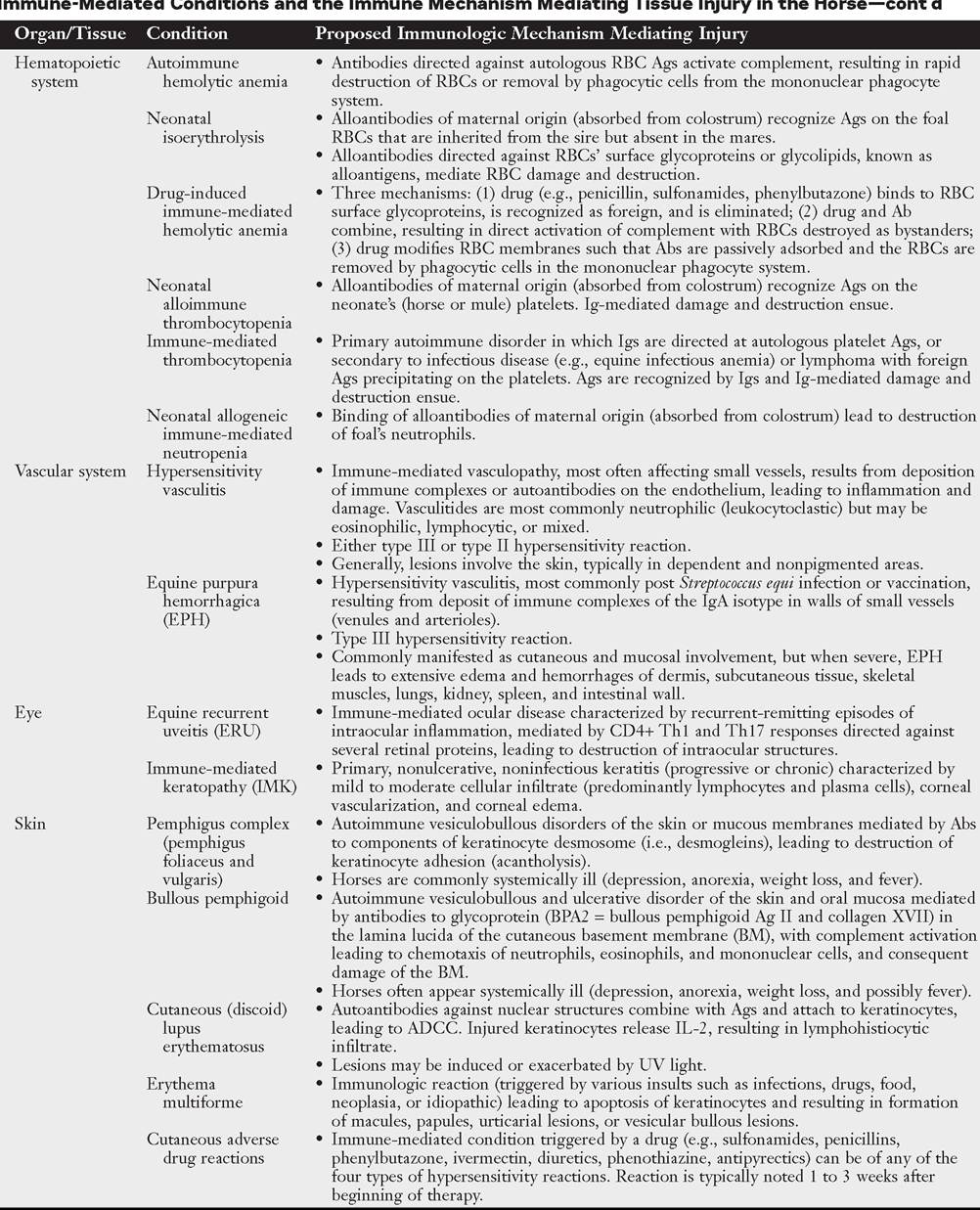
■ TABLE 53.4
Γ ---------
Ab, Antibody; ADCC, antibody-dependent cellular cytotoxicity; Ag, antigen; GI, gastrointestinal; Ig, immunoglobulin; IL, interleukin; RBCs, red blood cells; Th, T-helper cell; TNF, tumor necrosis factor; UV) ultraviolet.
or immunosuppression is suspected (e.g., assays to assess humoral, cellular, and innate immune responses)1-5; (2) assays for identifying inappropriate or exaggerated immunologic responses when immune-mediated injury is suspected (e.g., antinuclear antibody titer, assay for platelet surface-associated IgG, isotype-specific antibodies coating erythrocytes)6-9; and (3) assays of immunologic recognition of pathogens (e.g., antibody titer to specific antigens or pathogens) and protection against infectious agents.10 The aspects of immune response evaluation discussed in this section include only assays for characterizing the adequacy of the immune response when immunodeficiency or immunosuppression is suspected.
Assays for identifying inappropriate immunologic responses when an immune-mediated condition is suspected and assays of immunologic recognition of pathogens and protection against infectious agents are discussed in this book under body systems or found elsewhere. Genetic tests are also available to diagnose inheritable conditions, and those are discussed under their respective diseases in this book.11,12Characterizing the Adequacy of the Immune Response
Assessment of the adequacy of a patient’s immune response is warranted when there is an increased recurrence, severity, or chronicity of infectious illness above and beyond what is considered normal, especially if the possibility of enhanced virulence of the pathogen involved has been ruled out. Because true immunodeficiency disorders are uncommon, they should be considered only after more common causes of recurrent infection have been excluded. It is important to remember that inadequate immune response may occur in association with malnutrition, neoplasia (especially leukoproliferative disorders), autoimmune diseases, immunosuppressive therapy, and the presence of underlying diseases such as PPID. In addition, immunosuppression and immune evasion mediated by the infectious agent itself should be considered. Therefore the diagnostic plan should include evaluating the patient's immune response as well as ruling out conditions that may account for the inadequate immune response of the patient.
In case of increased recurrence, severity, or chronicity of infectious illness above and beyond what is considered normal, the type of infectious agent involved may provide clues that will guide the choice of diagnostic plan. For instance, when the recurrent, severe, or chronic infection is caused by encapsulated bacteria such as Staphylococcus aureus, Streptococcus zooepidemicus, Klebsiella spp., or Actinobacillus equuli, it raises the suspicion of compromised B-cell function, complement deficiency, or phagocytic dysfunction.4,13-16 Assays for humoral immunity and phagocytic function should be investigated first. When the recurrent, severe, or chronic infection is caused by an intracellular organism such as R. equi, P. jirovecii, Candida albicans, or Aspergillus spp., compromised cellular immunity should be considered.5
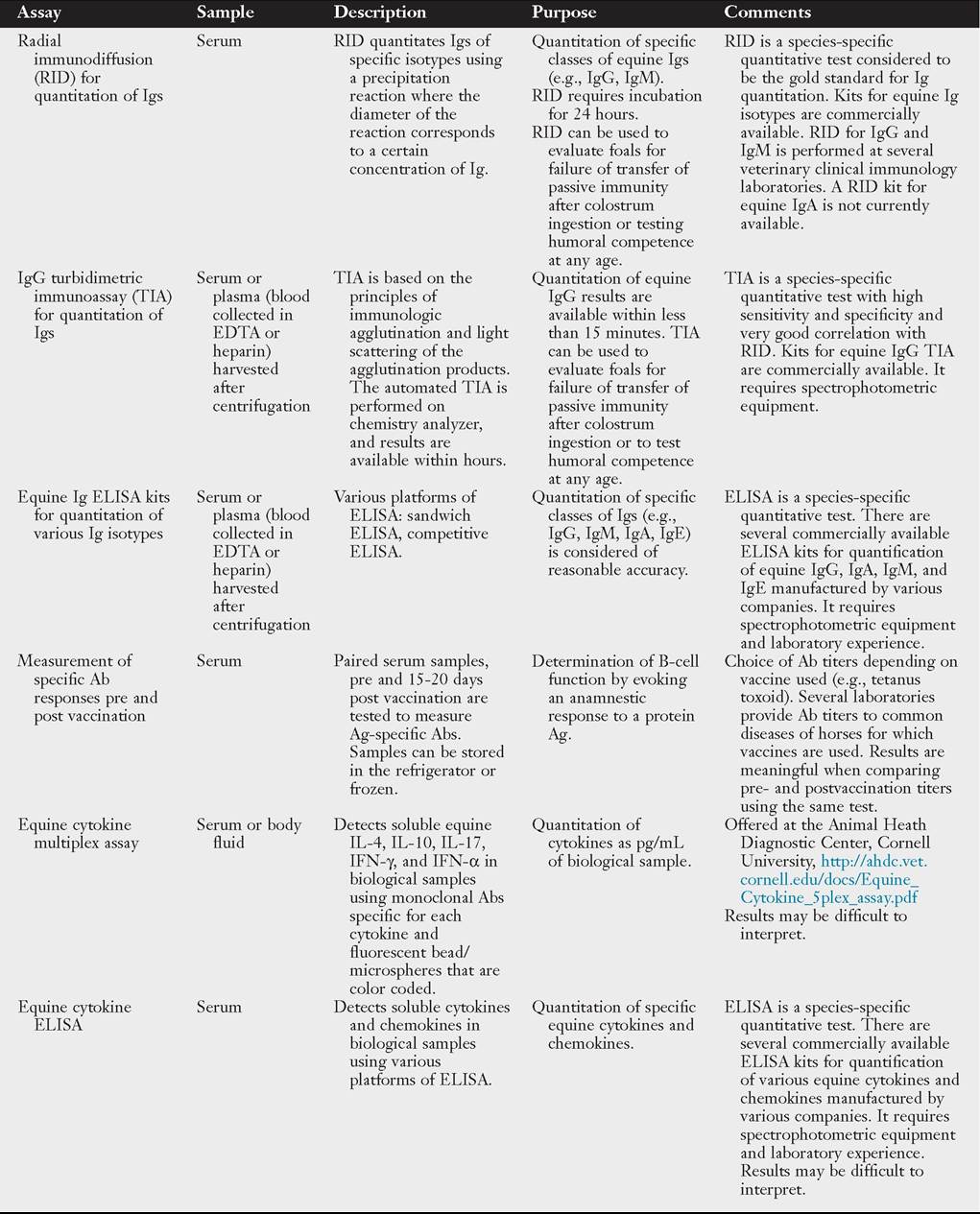
Evaluation of humoral immunity is assessed readily by measurement of Igs.
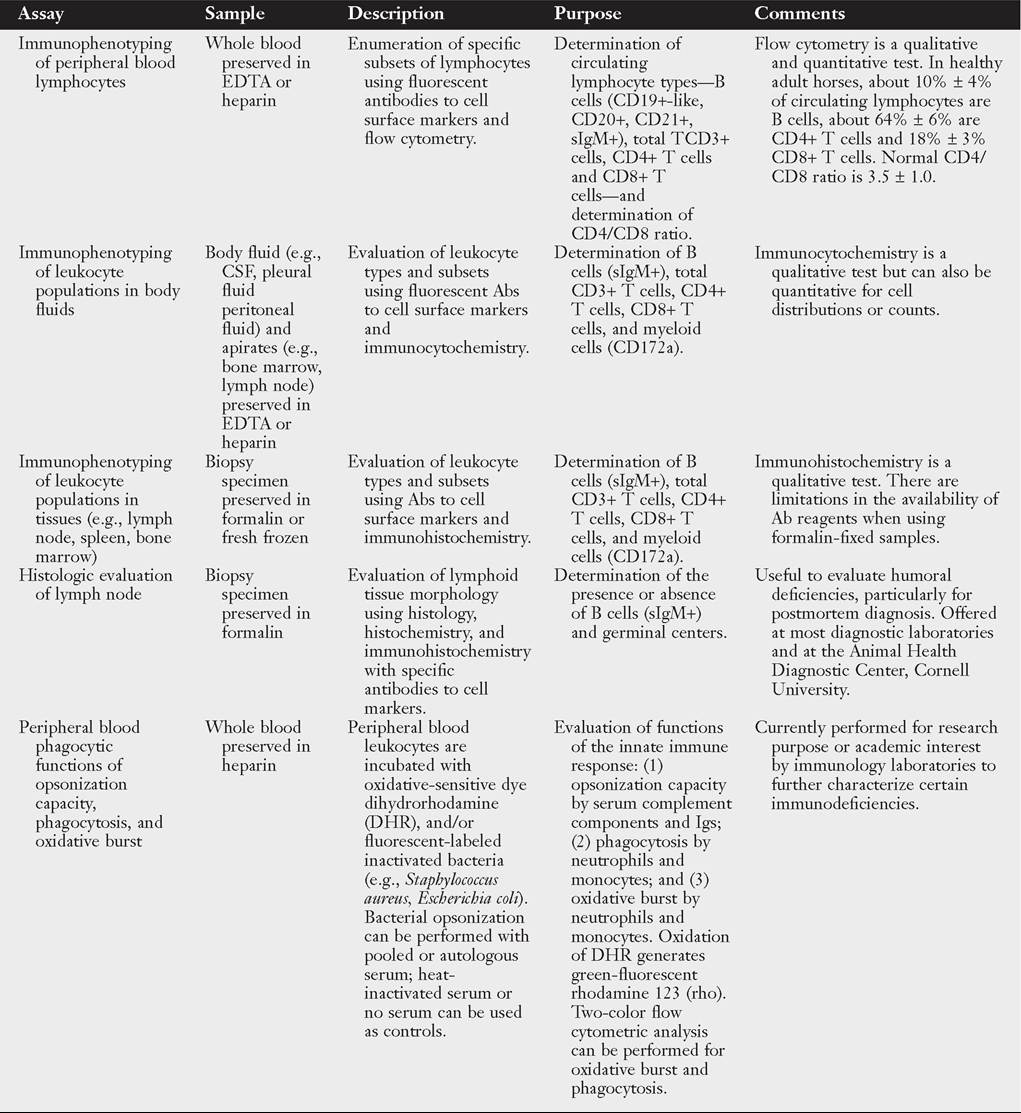
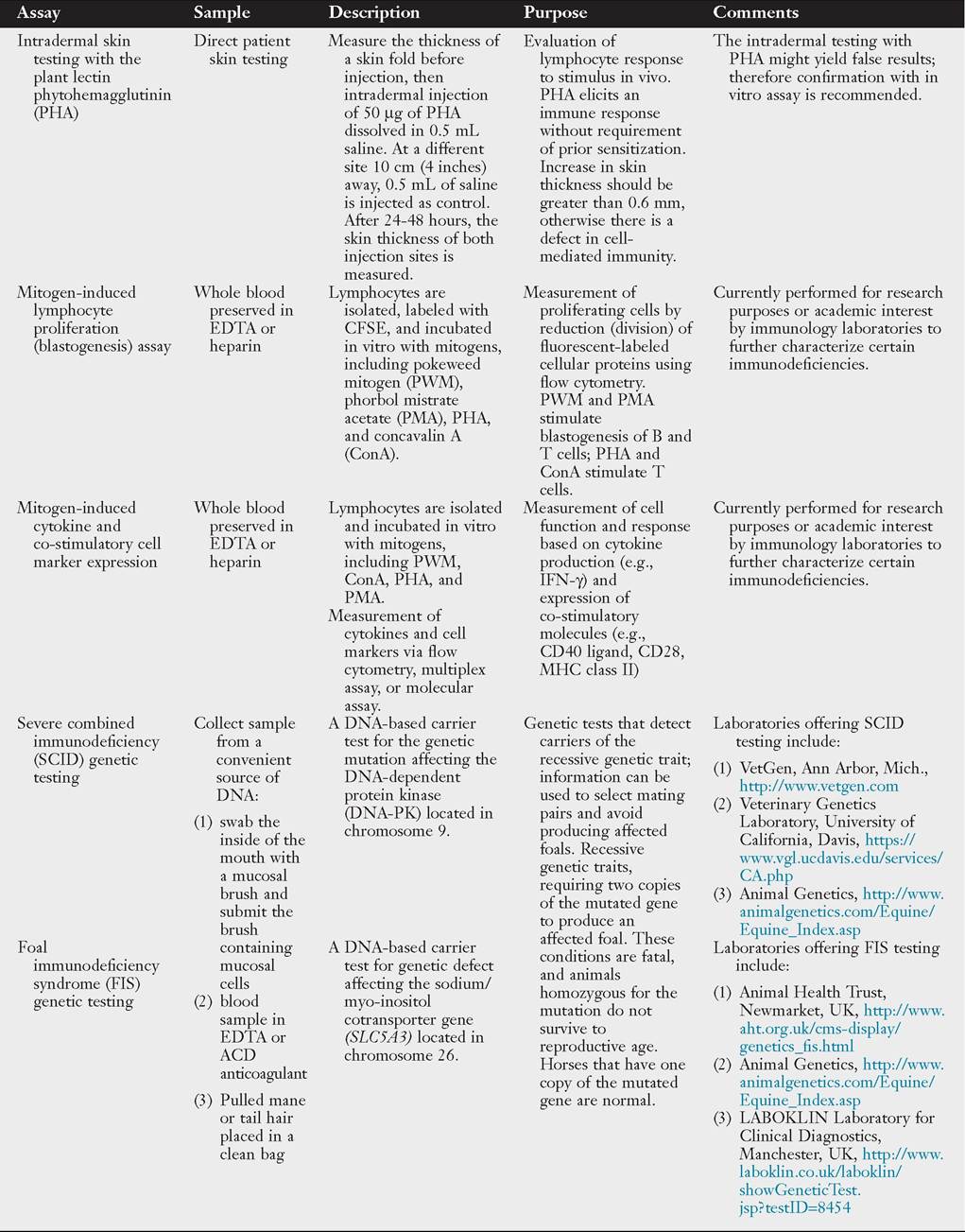
A comprehensive approach to the evaluation of humoral function in horses can be found elsewhere.4 Tests to evaluate humoral immunity include (1) determination of total serum concentration of each Ig isotype, namely IgG, IgM, and IgA17-20; (2) humoral response to vaccination by measurement of antigen-specific antibody titers prior to and at 15 to 21 days post vaccination4,10; (3) evaluation of gamma globulins by serum electrophoresis to determine the nature of gammopathies (monoclonal or polyclonal); (4) characterization of peripheral blood B-cell distribution by immunophenotyping and flow cytometry (FCM)4,21; and (5) detection of deficiencies of the CD4+ Th cell function that co-stimulates and helps B-cell differentiation and survival, leading to secondary humoral disorders.Assessment of cellular immunity is more challenging, and in vitro assays may fail to demonstrate dysfunction in cellular immune response. A comprehensive approach to the evaluation of cellular immune function in horses can be found elsewhere.5 Tests available to evaluate cellular immunity include (1) immunophenotyping and FCM of circulating lymphocytes, including determination of CD4+ and CD8+ T lymphocytes,22,23 (2) determination of cytokine profiles,24,25 (3) mitogen-induced lymphocyte proliferation or blastogenesis,21 and (4) mitogen- induced cytokines and expression of co-stimulatory markers.5
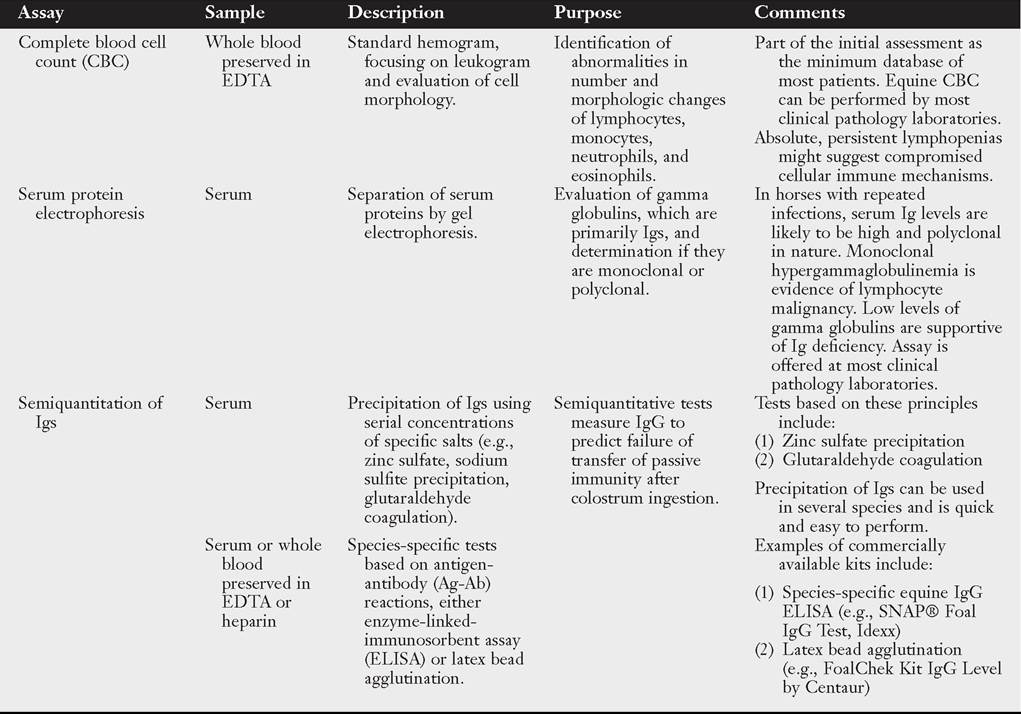
Table 53.5 lists assays used to assess and characterize the adequacy of adaptive (humoral and cell-mediated) and innate immune responses.
■ TABLE 53.5
Assays to Assess and Characterize the Adequacy of Immune Response in Horses
■ TABLE 53.5
Assays to Assess and Characterize the Adequacy of Immune Response in Horses—cont'd
■ TABLE 53.5
Assays to Assess and Characterize the Adequacy of Immune Response in Horses—cont'd
Continued
■ TABLE 53.5
Assays to Assess and Characterize the Adequacy of Immune Response in Horses—cont'd
ACD, Acid citrate dextrose as anticoagulant; CFSE, carboxyfluorescein succinimidyl ester; CSF, cerebrospinal fluid; EDTA, ethylenediaminetetraacetic acid; IFN, interferon; Ig, immunoglobulin; IL, interleukin; MHC, major histocompatibility complex.