Examination of the Muscular System
Stephanie J. Valberg
Clinical evaluation of the muscular system requires a systematic and routine method for examination. Often a veterinarian is asked to examine an animal with a history of a relatively nonspecific disease process that may be the result of muscular dysfunction.
Animals with electrolyte imbalances, pleuritis, colic, chronic wasting diseases, poor performance, weakness, and a number of lameness problems may initially have signs similar to those seen with some forms of muscular dysfunction.A thorough history of the animal or animals involved is an integral part of characterizing the muscle disorder, particularly because many disorders are intermittent in nature and triggered by certain environmental stimuli. A careful description of the animal's muscle tone, muscle mass, gait, degree of pain, exercise intolerance, and weakness while experiencing clinical signs should be obtained. In addition, the duration of illness, intermittency of clinical signs, factors precipitating clinical signs, exercise schedule, diet, current medications, vaccination history, and number of other animals affected and their familial relationships should all be recorded before the muscular system is examined.
Physical Examination
Initially the animal can be observed from all aspects at a distance while the horse is standing with forelimbs and hindlimbs exactly square. The examiner should observe the size, shape, and symmetry of all muscle groups and look for muscle fascicula- tions. This observation helps provide impressions about tropic changes, alterations in symmetry of particular muscle groups, and spontaneous muscle activity.
The animal can then be walked, trotted, or driven and evaluated for gait abnormalities. The symmetry of the gait and evidence of lameness, weakness, stiffness, and pain associated with movement can be noted.
Gait abnormalities may result from pain, muscle weakness, muscle cramping, spasticity, decreased range of joint motion, dysfunction of motor neurons, and ataxia.Following initial visual evaluation, muscles should be palpated to obtain an overall impression of muscle tone, consistency, sensitivity, swelling, atrophy, and heat. Firm, deep palpation of the lumbar, gluteal, and semimembranosus and semitendinosus muscles may reveal pain, cramps, or fibrosis. Comparisons between muscle groups and areas of the animal can then be made to identify atrophy or swelling. Some animals are tense and demonstrate apparent evidence of myalgia when palpation is first performed. However, given time and patience, many of these animals relax, and muscles or muscle groups that at first examination appeared to be very sensitive or hypertonic may in reality be normal. By this stage it can often be determined whether individual muscles, muscle groups, a limb or limbs, or the whole body musculature is involved. The symmetry or absence of symmetry of affected muscles or muscle groups is also important. Horses should stand perfectly square when comparing bilateral muscle groups.
Fine muscle tremors can be palpated and auscultated with a stethoscope. Concurrent signs of anxiety or pain should be noted, and the animal should be reevaluated in calm surroundings if necessary. In animals with spontaneous muscle activity, muscle groups should also be percussed with a percussion hammer. The triceps, pectoral, gluteal, and semitendinosus muscles are often easily accessed for percussion. A positive percussion sign occurs when the muscle holds a contracture for several seconds, creating a dimpled appearance below the contracted muscle (percussion myotonia) (Fig. 42.1). This occurs as the result of abnormal mechanical irritability and sustained contraction of the percussed fibers. Running a blunt instrument such as artery forceps, a needle cap, or a pen over the lumbar and gluteal muscles should illicit extension (swayback) followed by flexion (hogback) in healthy animals.
Guarding against movement may reflect abnormalities in the pelvic or thoracolumbar muscles or pain associated with the thoracolumbar spine or sacroiliac joints.A tail pull examination while the horse is standing still and walking can be used to assess rear limb weakness. If there is evidence of weakness, differentiation between muscular and neurologic origin is ideal. This requires a detailed neurologic examination and can often be extremely difficult. In general, muscular weakness is not associated with ataxia unless it is extremely severe. Weakness is often manifested by muscle fasciculations, knuckling at the walk, frequent recumbency with difficulty rising, and shifting of weight because of an inability to fix the stifles.
If the primary abnormality identified is related to exertion, a lameness evaluation including flexion tests is often indicated as part of evaluation of the muscular system. Muscle pain may be secondary to changes in movement caused by skeletal pain. The horse should be observed at a walk or trot for any gait abnormalities and in some cases lunged for 15 minutes or ridden until clinical signs are elicited.
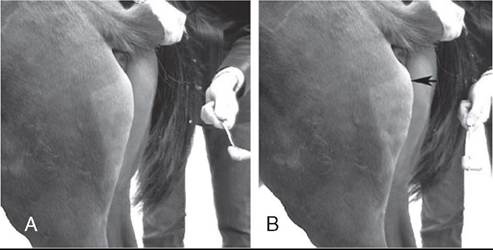
FIG. 42.1 Percussion of the semitendinosus muscle showing the muscle at rest (A) and an abnormal persistent firm contracture after tapping the muscle with a percussion hammer (B) in a horse with myotonia.
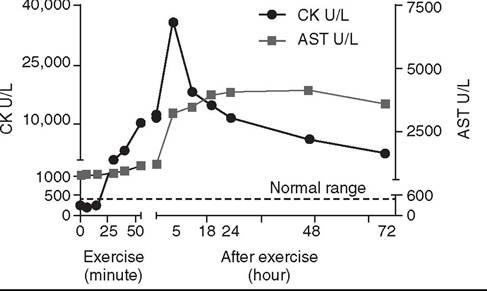
FIG. 42.2 Serum creatine kinase (CK) and aspartate transaminase (AST) activities over a 3-day period in a Standardbred trotter that developed exertional rhabdomyolysis during 55 minutes of trotting at 5 m/s. Serum CK activity increased during exercise and peaked in the sample obtained 5 hours after exercise. Serum AST was above normal range before exercise, increased after exercise, and peaked 48 hours following exercise.
Clinical Pathology
Serum Enzyme Activities and Myoglobin Concentrations
Serum enzyme activities can be extremely useful in determining whether muscle cell necrosis is a predominant feature of a suspected muscle disease.
Under normal conditions the serum activities of the enzymes used to assess muscle damage are low. However, leakage of the enzymes from myocytes into the bloodstream may occur if the cell membrane is disrupted through muscle cell necrosis or if the permeability of the cell membrane is increased. A number of other factors may influence the activities of enzymes within the circulation. These include rate of enzyme production, alternative sources of the enzyme, rates of enzyme excretion and degradation, and alterations to the pathways involved in enzyme removal or inactivation.Creatine kinase (CK), aspartate aminotransferase (AST), and lactate dehydrogenase (LDH) activities in serum are used to assess muscle damage in large animals. Serum CK offers remarkable sensitivity as an indicator of myonecrosis and is predominantly located in skeletal and heart muscle. It is intimately involved in energy production within the cytoplasm and is readily liberated into the extracellular fluid when the muscle cell membrane is disrupted. Serum CK activity increases within hours of a muscle insult and peaks within 4 to 6 hours after injury (Fig. 42.2). Limited elevations in CK may accompany training, transport, and strenuous exercise. Elevations of CK to 400 or 500 IU/L may occur when training commences or in response to moderate exercise. Extreme fatiguing exercise (e.g., endurance rides or the cross-country phase of a 3-day event) may result in CK activities being increased to more than 1000 IU/L but usually less than 8000 IU/L. These elevations are not typically reflective of an extensive myopathy, and serum activities of CK rapidly return to baseline activities (i.e., in the absence of hemolysis or RBCs in urine is highly suggestive of myoglobinuria. Further differentiation of myoglobin from hemoglobin is sometimes warranted, and, where available, electrophoresis, nephelometry, or spectroscopy may be used. Spectroscopy does not always reliably distinguish between myoglobin and hemoglobin.
Electrolyte, mineral, and creatinine concentrations in urine and blood have been used to determine electrolyte balance in horses with muscle cramping or exertional rhabdomyolysis.3 Problems often encountered, however, are the large fluctuations in daily electrolyte excretion that occur in the same horse and between horses, the interference of high urinary potassium concentrations with measures of sodium concentrations when an ion-specific electrode is used, and the presence of calcium crystals in equine urine, which artifactually decrease the calcium and magnesium measured if urine samples are not acidified.4 Renal fractional excretions (FEs) can be calculated using the following formula: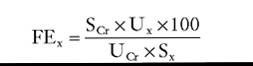
where U is urine, S is serum, x is measured electrolyte, and Cr is creatinine.
If urine calcium is to be determined, acidification of urine to dissolve all calcium oxalate crystals is recommended to provide exact calcium excretion. Determination of potassium, chloride, magnesium, and phosphorus concentrations can be performed using ion-specific electrodes or by inductively coupled plasma atomic absorption.
Normal values for FEs of electrolytes depend on a horse's diet. Normal values (%) for horses consuming grass, hay, and a sweet feed mix with available salt are FENa 0.04 to 0.08, FEk 35 to 80, FECi 0.4 to 1.2, FECa 5.3 to 14.5, FEp 0.05 to 4.1, and FEMg 14.2 to 21.4.4,5
Exercise Testing
Evaluation of muscle disorders that are precipitated by exercise may require an exercise challenge test. Horses should be observed for evidence of exercise intolerance, as well as muscle stiffness. An exercise test should not be used in horses with overt signs of rhabdomyolysis but rather to determine if horses not currently showing clinical signs are prone to exertional rhabdomyolysis. The goal is to induce subclinical elevations in serum CK activity.
Abnormal increases in CK are more likely to occur if slow trotting is performed rather than strenuous exercise.6 Often 15 minutes of exercise at a walk and trot in unfit horses or at a constant slow trot in fit horses will elucidate subclinical elevations of CK. If signs of stiffness develop before this, exercise should be concluded. CK activities in blood samples taken immediately after exercise do not reflect the amount of exercise-induced muscle damage. For best results, blood samples for CK activity should be taken before and 4 to 6 hours after exercise. In healthy horses, 15 to 30 minutes of light exercise rarely causes more than a threefold increase in CK activity.7,8 Elevations greater than fivefold are indicative of exertional rhabdomyolysis. Standardized treadmill exercise testing can also be used to evaluate muscle responses and measure metabolic responses to exercise.Electromyography
Electrodiagnostic studies detect spontaneous or evoked potentials of neurogenic or myogenic origin using electrodes positioned in the muscle. Electromyography (EMG) is particularly useful to evaluate large animals with altered muscle tone. EMG of normal skeletal muscle shows a brief burst of electrical activity when the needle is inserted (insertional activity) in muscle and then quiescence, unless motor units are recruited (motor unit action potentials) or the needle is close to a motor end plate (miniature end plate potentials). Normal muscle shows little spontaneous electrical activity unless the muscles contract or the horse moves. Horses with abnormalities in the electrical conduction system of muscle, or denervation of motor units, show abnormal spontaneous electrical activity in the form of fibrillation potentials, positive sharp waves, myotonic discharges, or complex repetitive discharges.9-12 Fibrillation potentials and positive sharp waves represent spontaneous firing of muscle fibers. Myotonic discharges are bursts of complex high-frequency potentials, whereas complex repetitive discharges are similar but have fixed amplitude and frequency. They both represent abnormal simultaneous firing of groups of muscle fibers. Motor unit action potentials can be evaluated to assess their amplitude, duration, phase, and number of phases. Myopathic changes include a decrease in duration and amplitude of motor unit action potentials.10,12 More information about the motor unit could be provided by nerve conduction velocities (NCVs); however, the inaccessibility of motor nerves makes measurement difficult in large animals. Both EMG and NCVs are used to classify the primary disease as neuropathic or myopathic, to determine the distribution of the disease, and to provide insight into the pathophysiologic mechanisms of the disease.9,13 Equipment costs are relatively high, and expertise is required in operation and interpretation of results. Readers are advised to consult Chapter 35 before considering the use of EMG.
Nuclear Scintigraphy
Nuclear scintigraphy is useful for identification of some forms of muscle damage, particularly an area of deep muscle damage that was not suspected on the basis of clinical examination.14 Technetium 99m methylene diphosphonate (MDP) is taken up in some damaged muscle in the horse and is best seen in the bone phase images (i.e., 3 hours after injection). Scintigraphy has been used in horses with a history of poor performance, with or without stiffness after exercise, to confirm a diagnosis of equine rhabdomyolysis.15 The mechanism of MDP binding is unknown, but the release of large amounts of calcium from damaged muscle or the exposure of calcium binding sites on protein macromolecules in the damaged muscle may be responsible. Scintigraphy may be helpful in some cases involving focal damage to either proximal forelimb or hindlimb muscles.14
Ultrasonography
Diagnostic ultrasonography is potentially useful for identification of muscle trauma, crepitus, fibrosis, and atrophy. Muscles have a rather typical striated echogenic pattern, but this varies according to the muscle group and careful comparisons must be made between similar sites in contralateral limbs, in both transverse and longitudinal images.14 The appearance of muscle is also sensitive to the way the animal is standing and whether the muscle is under tension, so it is important that the animal is standing squarely and bearing weight evenly. Muscle fascia appears as well-defined, relatively echodense bands.14 Care must be taken in identifying large vessels and artifacts created by them.
In an acute injury, muscle fiber disruption is seen as relatively hypoechoic areas within muscle, with loss of the normal muscle fiber striation. The jagged edge of the margin of the torn muscle may be increased in echogenicity.14 Tears in the muscle fascia may be identified. The defect in muscle may be filled by loculated hematoma that is hypoechoic. As the muscle repairs, it becomes progressively more echogenic. Relatively hyperechoic regions may be a result of increased connective tissue or loss of muscle cell mass. Hyperechoic shadowing artifacts usually represent mineralization or gas pockets.14
Muscle Biopsy
Examination of muscle fibers, neuromuscular junctions, nerve branches, connective tissue, and blood vessels within a biopsy sample can provide additional information necessary to fully characterize a neuromuscular disorder.16-18 Routine light and electron microscopic examinations, combined with histochemical evaluations, may provide insights into the particular manifestations of neuromuscular diseases and their rate of progression. A number of basic pathologic responses of muscle can be identified in paraffin-fixed sections. These include inflammatory infiltrates, muscle fiber necrosis, muscle fiber regeneration, increased number of central nuclei, variations in muscle fiber sizes and fiber shapes, vacuolar change, and proliferation of connective tissue. However, there are many pathologic alterations that cannot be detected in formalin-fixed tissue but can readily be seen in histochemical stains of fresh-frozen biopsy samples.16-18 These include muscle fiber types and their pattern of distribution, differentiation of neurogenic atrophy from disuse atrophy or a primary myopathy, characterization of vacuolar storage material, characterization of inclusion bodies, assessment of mitochondrial density, and additional clues that may allow identification of a specific disorder or category of muscle disorders. Furthermore, formalin fixation results in artifactual cracking, fiber shrinkage, and leakage of substrates such as glycogen, which can affect proper interpretation of muscle pathology.
When considering collection of muscle biopsies, some general guidelines apply. Preferably, samples should be collected from what is considered abnormal or diseased muscle. A 6-mm- outer-diameter (Jorgen Kruuse A/S, Langeskov, Denmark) percutaneous needle biopsy technique can be used to obtain small muscle samples through a ¼-inch skin incision using a local anesthetic subcutaneously. If this technique is used, enough muscle should be obtained to form a ½-inch-square sample at a minimum. These samples do not, however, tolerate shipment to an outside laboratory. The optimum biopsy for shipment of histopathology tissues to a laboratory is collected using surgical or open techniques, performed under local anesthesia. Care must be exercised to infiltrate only the subcutaneous tissues, not the muscle, with the anesthetic agent. The objective is to obtain approximately a ½-inch cube of tissue; hence a suitably long skin incision is required. Two parallel incisions ½ inch apart should be made longitudinal to the muscle fibers with a scalpel. The muscle should be handled only in one corner using forceps, and crushing should be avoided. The muscle sample is then excised by cross-section incisions ½ inch apart, and the tissue is fixed appropriately. Routine histopathology samples can be placed in formalin; fresh samples can be placed in a watertight hard container after being wrapped in gauze lightly moistened with saline and shipped chilled to laboratories for freezing. On arrival at specialized laboratories, fresh samples for histochemical analysis are fixed in isopentane (methylbutane) chilled in liquid nitrogen to ensure rapid freezing and minimization of freeze artifact. Samples that potentially may be used for biochemical analysis should be immediately frozen in liquid nitrogen. Other routine histopathologic techniques may also be of diagnostic value. A special fixative may be required if such practices are to be undertaken. Samples for electron microscopy (EM) require appropriate fixation in glutaraldehyde preparations. Ideally, thin sections of muscle for EM should be clamped in vivo to maintain fibers at a resting length before they are excised. However, if pathology other than the alignment of thick and thin myofilaments is to be investigated, small muscle pieces can be excised and placed directly in appropriate EM fixative.
Responses of strips of fresh muscle to stimuli such as caffeine, halothane, and a variety of other agents can also be performed by specialized laboratories to diagnose recurrent exertional rhabdomyolysis and susceptibility to malignant hyperthermia but are not routine diagnostic procedures.19-21